
Abstract
Objective
The prevention and clinical management of fractures in the elderly have always been challenging issues in orthopedic practice. This study aims to explore the relationship between bone mineral density (BMD) and the types of proximal femoral fractures in elderly patients.
Methods
This study is a retrospective study. It included 876 patients with proximal femoral fractures (446 with femoral neck fractures and 430 with trochanteric fractures) who were admitted to the Affiliated Central Hospital of Shenyang Medical College between 1 January 2020 and 1 January 2023. The study compares the differences in BMD between the trochanteric fracture group and the femoral neck fracture group.
Results
The trochanteric fracture group had significantly lower average lumbar spine BMD and total BMD of both femoral heads compared to the femoral neck fracture group. In both groups, the BMD of the affected femoral head was higher than that of the healthy femoral head. The average BMD of the affected femoral head was higher than that of the healthy femoral head in all patients (P < 0.001).
Conclusion
In addition to fracture management, patients with trochanteric fractures should also receive treatment for osteoporosis. Furthermore, patients with proximal femoral fractures need to prevent secondary fractures in the healthy femur.
Keywords
Introduction
Proximal femur fracture is a common type of fracture in the elderly. With the intensification of global aging, the number of proximal femur fracture patients is increasing year by year. Issues related to clinical care, fracture prevention, and treatment are becoming increasingly prominent. Proximal femur fracture, one of the top 10 reasons causing the elderly to lose mobility and shorten their life span, is also known as the “last fracture” of the elderly and is extremely harmful to this population.1,2 Proximal femur fractures can be clinically divided into femoral neck fractures and intertrochanteric femoral fractures. There are certain differences between these two types of proximal femur fractures in their symptoms and surgical options. Currently, femoral neck fractures are mostly treated by artificial hip replacement; however, for intertrochanteric femoral fractures, internal fixation is considered the most effective method for treating elderly patients. This is due to the poor stability, loosening, and sinking of the hip prosthesis associated with artificial hip replacement.3,4
In younger people, proximal femur fractures rarely occur and are usually caused by high-energy trauma. Studies have found that the reason elderly individuals are prone to proximal femur fractures is closely related to osteoporosis and osteopenia in this population.5–7 In clinical practice, bone mineral density (BMD) examination is often used to measure the osteopenia of patients. However, whether the severity of BMD can directly affect the type of proximal femur fracture has not been reported yet.
This study collected data from patients aged 60 years and above with proximal femoral fractures who visited the Central Hospital affiliated with Shenyang Medical College over a period of three years. By measuring the T-score of BMD and comparing it with the classification of proximal femoral fractures, the study explored the correlation between BMD and the classification of proximal femoral fractures, providing guidance for the prevention and treatment of proximal femoral fractures in clinical practice.
Data and methods
Study data
The manuscript has already been submitted as a preprint on Research Square: https://www.researchgate.net/publication/377314490_The_Correlation_between_Proximal_femur_Fracture_and_Bone_Mineral_Density_in_the_Elderly/fulltext/659fe620af617b0d873be3f9/The-Correlation-between-Proximal-femur-Fracture-and-Bone-Mineral-Density-in-the-Elderly.pdf?origin=scientificContributions.
This study selected 876 patients admitted to the Central Hospital affiliated with Shenyang Medical College for the diagnosis of proximal femur fractures from January 2020 to January 2023. The cohort included 446 patients with femoral neck fractures and 430 patients with intertrochanteric femoral fractures, all of whom underwent BMD examination.
This study was approved by the Ethics Committee of the Affiliated Central Hospital of Shenyang Medical College (No. 20200918). The Ethics Committee is located at Central Hospital affiliated to Shenyang Medical College, 5 Nanqi West Road, Shenyang 110075, Liaoning, China. The approval was granted on 20 December 2019.
Inclusion criteria: Patients who:
① Were 60 years old or older. ② Suffered from proximal femur fractures caused by low-energy trauma. ③ Underwent BMD examination after admission. ④ Suffered from a unilateral proximal femur fracture.
Exclusion criteria: Patients who:
① Suffered from pathological proximal femur fractures caused by bone tumors. ② Had undergone surgical treatment on the opposite side of the fracture. ③ Suffered from bone metabolism disorders. ④ Had been using steroids for a long term. ⑤ Were bedridden for a long time and unable to move due to various reasons.
Methods
This study is a retrospective study. This study was conducted in accordance with the Declaration of Helsinki (1975, revised in 2024). This study has de-identified all patient information. The reporting of this study conforms to STROBE guidelines. 8
Time frame for BMD measurement
BMD measurements for all patients were completed within 24 h of admission and performed simultaneously with routine tests such as blood work and biochemical parameter assessments. The selection of this timeframe was aimed at excluding potential effects of acute-phase therapeutic interventions (e.g. glucocorticoid administration and immobilization) on bone metabolism, thereby ensuring the measurements reflect the patient's baseline bone status.
Standardized measurement protocol
All patients underwent dual-energy X-ray absorptiometry (DXA) scans of the lumbar spine and bilateral femoral heads using equipment manufactured by General Electric. Following registration of patient height and weight, DXA measurement parameters and exposure factors were automatically generated using Lunar Prodigy Primo software. During the examination, patients lay supine at the center of the scanning bed with arms crossed over the chest and feet secured in foot holders (knees inward and legs internally rotated), aligning the center line of the scanning bed with the line on the base of the foot holder. Laser lights were positioned approximately 5 cm below the patient's navel and 7–8 cm below the greater trochanter when measuring T-scores of the lumbar spine and bilateral femoral heads. Measurements included lumbar spine bone density (LS 1–4), total femoral head bone density, affected femoral head bone density, and healthy femoral head bone density, with corresponding T-scores recorded. All BMD measurements for all patients were performed and interpreted by a team of three radiology physicians from our hospital's imaging department.
Based on X-ray findings, patients were classified into proximal femoral fractures: femoral neck fractures and intertrochanteric fractures. Femoral neck fractures were defined as fractures between the femoral head and the base of the femoral neck, whereas intertrochanteric fractures were defined as fractures within 2 cm below the lesser trochanter and extending beyond the base of the femoral neck.
A comparison of lumbar spine bone density and bilateral femoral head bone density was conducted between the two patient groups. Additionally, the bone density of the injured and uninjured sides of the femoral head was compared between the groups.
Statistical methods
SPSS 26.0 software was utilized for statistical analysis. The Kolmogorov–Smirnov test assessed the normal distribution of the data. A P-value >0.05 indicates normal distribution, and measurement data is presented as mean ± SD (
Results
Comparison of BMD between two groups of patients
During the study phase, a total of 896 patients came to the hospital for treatment, out of which 20 patients met the exclusion criteria. This study included 876 patients with proximal femur fractures, comprising 430 cases of intertrochanteric femoral fractures and 446 cases of femoral neck fractures. There were no significant differences in gender, age, and body mass index between the two groups (P > 0.05), as detailed in Table 1.
Basic information on intertrochanteric femoral fracture and femoral neck fracture.

The lumbar spine BMD T-scores of the 876 patients with proximal femur fractures ranged from −4.8 to 2.9, with a mean of −1.99 ± 2.06; the lumbar spine BMD T-scores were −2.66 ± 1.63 for the 430 patients in the intertrochanteric femoral fracture group and −1.56 ± 1.42 for the 446 patients in the femoral neck fracture group. The lumbar spine BMD T-scores in the intertrochanteric femoral fracture group were significantly lower than those in the femoral neck fracture group, with a statistically significant difference (P < 0.001). The total femoral head BMD T-scores of both sides in the 876 proximal femur fracture patients ranged from −4.8 to 2.7, with a mean of −1.84 ± 1.13; the total femoral head BMD T-scores were −2.74 ± 1.38 for the 430 patients in the intertrochanteric femoral fracture group and −1.73 ± 1.57 for the 446 patients in the femoral neck fracture group. The total femoral head BMD T-scores in the intertrochanteric femoral fracture group were significantly lower than those in the femoral neck fracture group, with a statistically significant difference (P < 0.05). See Table 2 for details.
T values of intertrochanteric femoral fracture and femoral neck fracture.
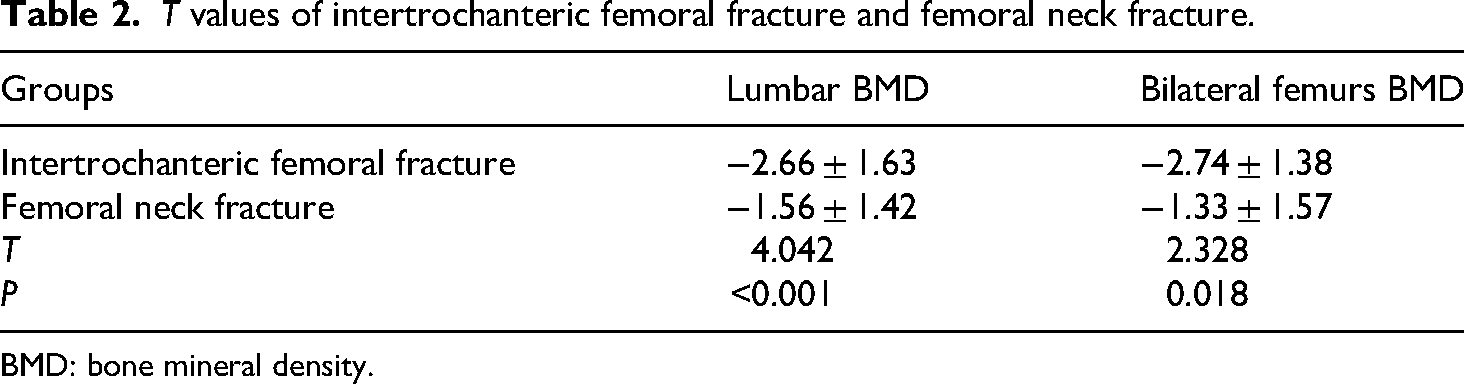
BMD: bone mineral density.
Comparison of BMD between the healthy and affected femurs of patients in the two groups
In this study, among 430 patients with intertrochanteric femoral fractures, the BMD T-scores of the affected femurs ranged from −4.3 to 3.1, with an average of −2.22 ± 1.49; whereas the BMD T-scores of the healthy femurs ranged from −5.8 to 2.3, with an average of −3.28 ± 1.58. The BMD T-scores of the healthy femurs were significantly lower than those of the affected femurs, with a statistically significant difference (P < 0.001). Among 446 patients with femoral neck fractures, the BMD T-scores of the affected femurs ranged from −3.2 to 4.1, with an average of −1.68 ± 1.26; while the BMD T-scores of the healthy femurs ranged from −4.6 to 3.9, with an average of −2.02 ± 1.09. Similarly, the BMD T-scores of the healthy femurs were significantly lower than those of the affected femurs, with a statistically significant difference (P < 0.001). See Table 3 for details.
T values of the affected femurs and healthy femurs.

BMD: bone mineral density.
Comparison of BMD between the affected and healthy femurs of all proximal femur fracture patients
Among the 876 proximal femur fracture patients included in this study, the BMD T values of the affected femurs ranged from −4.3 to 4.1, with an average of −1.898 ± 1.76, while those of the healthy femurs were within the range of −5.8 to 3.9, averaging −2.66 ± 1.33. The BMD T values of the healthy femurs were significantly lower than those of the affected femurs, with a statistically significant difference (P < 0.001). Refer to Table 4 for details. The Wilcoxon signed-rank test was used to compare the BMD T values between the affected and healthy femurs across all cases. See Figure 1.
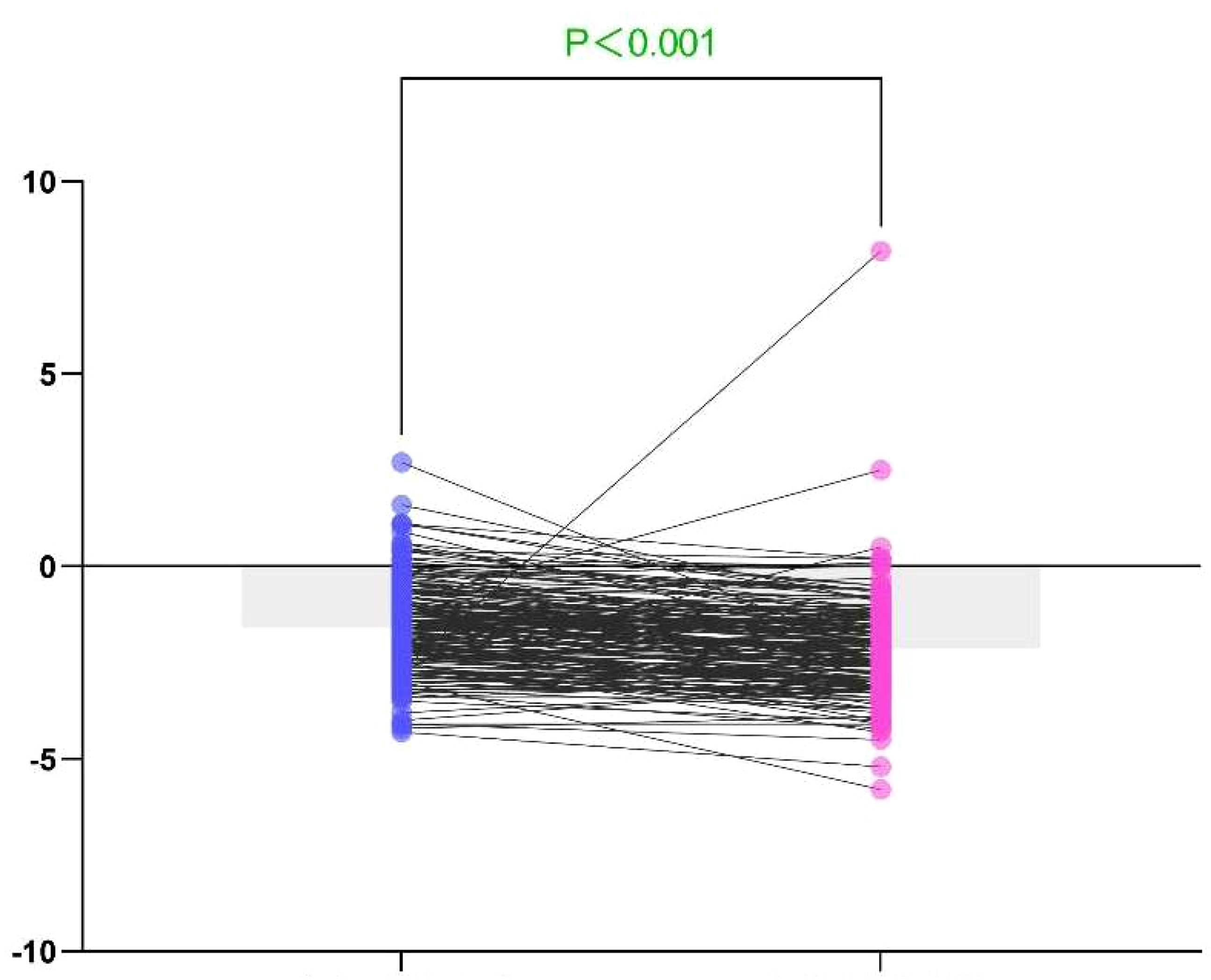
Comparison of bone mineral density (BMD) T values between the affected and healthy femurs with the Wilcoxon signed-rank test.
T values of affected and healthy femurs of all proximal femur fracture patients.

BMD: bone mineral density.
Discussion
Currently, the correlation between BMD and the type of proximal femur fracture has not been extensively reported. This study included a total of 876 proximal femur fracture patients, with 446 cases of femoral neck fractures and 430 cases of intertrochanteric femoral fractures, indicating a clinical preference for femoral neck fractures among the elderly. This research analyzed the differences in BMD between intertrochanteric femoral fractures and femoral neck fractures, as well as between the affected and healthy femurs of proximal femur fracture patients. The results revealed that patients with intertrochanteric femoral fractures had lower BMD compared to those with femoral neck fractures and that the BMD of healthy femurs in proximal femur fracture patients was generally lower than that of the affected femurs.
Osteoporosis, a systemic skeletal disease characterized by osteopenia and deterioration of bone tissue microstructure, increases skeletal fragility and susceptibility to fractures.9–11 Proximal femur, vertebral, and distal radius fractures are the most common osteoporotic fractures in middle-aged and elderly individuals.10,12 Due to global population aging, fractures pose an increasingly significant public health challenge.10,12 In clinical practice, there is no alternative method to quantitatively evaluate bone strength, and BMD remains the gold standard for diagnosing osteoporosis in middle-aged and elderly individuals.9,13,14 However, DXA equipment is expensive, limiting its availability in community and grassroots hospitals. Occult blood loss is a primary contributor to significant perioperative blood loss in intertrochanteric femoral fractures.15,16 Cui et al. 16 identified low BMD as a critical risk factor for occult blood loss in intertrochanteric femoral fractures, underscoring the importance of early intervention to prevent complications. Maeda et al. 17 used quantitative computed tomography to compare BMD differences between different types of proximal femur fractures, finding that intertrochanteric femoral fractures were associated with more severe osteoporosis characterized by cortical thinning of the femoral shaft compared to femoral neck fractures. This aligns with our study's finding of significantly lower BMD in patients with intertrochanteric femoral fractures compared to those with femoral neck fractures, highlighting the clinical importance of considering low BMD even in settings without DXA equipment.
Interestingly, our study found that in most proximal femur fracture patients, the BMD of healthy femurs was lower than that of affected femurs, contrary to the common perception that BMD is lower in affected femurs. Bone mass is significantly influenced by weight-bearing and muscle traction,18,19 with immobilization being a key factor in osteoporosis development. Studies have shown significant reductions in bone mass on the hemiplegic side of stroke patients due to reduced mobility.20,21 Nishizawa et al. 22 compared BMD differences between lower limbs in patients with knee osteoarthritis under different weight-bearing conditions, finding significantly higher BMD in limbs with greater stress. Our study suggests that the BMD of affected femurs may be higher due to unconscious favoring of the leg with more daily stress during falls among most proximal femur fracture patients. This finding also implies that BMD in the unfractured hip may be lower than in the fractured hip.
In clinical practice, contralateral fractures after surgery are not uncommon among proximal femur fracture patients, with a twofold increase in complications and postoperative infections compared to initial fractures.23,24 Müller et al. 23 conducted a cohort study revealing a high incidence of contralateral fractures and associated complications, emphasizing the need for osteoporosis prevention and treatment postoperatively to reduce such risks.
This study has several limitations. First, it is a single-center study with a relatively small sample size, which may limit the generalizability of the results. However, our orthopedic department is a provincially recognized specialty with a high reputation, attracting patients with hip fractures from both within and outside the province. This wide patient base enhances the representativeness and preliminary generalizability of our findings.
Second, data collection for this study coincided with the COVID-19 pandemic (2020–2023), which may have introduced potential selection bias. During the pandemic, patient healthcare-seeking behavior and access to medical services were affected, potentially leading to underrepresentation of certain patient groups or delays in fracture diagnosis. Therefore, future large-scale, multicenter studies are needed to further validate our findings.
Despite these limitations, the results of this study have important clinical implications for fracture prevention strategies. Our research not only reveals the differences in BMD between intertrochanteric and femoral neck fractures but also highlights the necessity of targeted interventions to improve bone health. These findings provide valuable insights for clinicians in developing individualized prevention and treatment strategies, helping to reduce the incidence of primary and recurrent fractures among high-risk populations.
Conclusion
There may be a correlation between BMD and the types of proximal femoral fractures in the elderly. Individuals with higher BMD may be more prone to femoral neck fractures, while those with lower BMD are more susceptible to intertrochanteric femoral fractures. Clinicians should consider conducting BMD tests in patients with intertrochanteric femoral fractures who have not undergone DXA scans and initiate early osteoporosis interventions. Notably, in most cases, the BMD of the healthy femur is lower than that of the affected femur in proximal femoral fracture patients, underscoring the importance of preventing contralateral fractures during the treatment of one side of a proximal femoral fracture.
Footnotes
Acknowledgements
We would like to express our gratitude to the patients who participated in this study for providing their BMD data.
Ethical considerations
This study was approved by the Ethics Committee of the Central Hospital Affiliated to Shenyang Medical College. As the study only involved the collection of BMD data without any personally identifiable information, the requirement for written informed consent was waived by the committee. Verbal informed consent was obtained from all participants prior to inclusion in the study.
Author contributions
All authors contributed to the preparation, design, and successful execution of the study. Hairui Liang contributed to data collection, manuscript writing, proofreading, and redrafting. Beibei Chen, He Zhang, and Ming Sun were responsible for data collection and data analysis. Rongda Xu and Siyu Duan handled reference arrangement and data collection. Zhencun Cai contributed to data collection, editing, fine arrangement, figure making, and overall article arrangement as the corresponding author. All authors have read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Science and Technology Plan Project of Shenyang City (Project No. 22-321-32-13), the Liaoning Provincial Department of Education Fund Project (JYTMS20231396), and the Science and Technology Fund of the Education Department of Liaoning Province (Project No. 2024-MS-222).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author upon a reasonable request.