
Abstract
Objective
Finding accessible diagnostic tools for the diagnosis of atherosclerosis is necessary due to its rising incidence rate. The correlation of perirenal fat thickness (PRFT) and atherosclerosis has been investigated in previous studies using different imaging modalities including ultrasound and CT-scan, but their results have been equivocal. Therefore, we performed a systematic review and meta-analysis of observational studies to determine this potential correlation.
Methods
This study is a systematic review and meta-analysis of observational studies. A comprehensive search was conducted up to 2 July 2024, across articles published in the Scopus, Web of Science, Cochrane Library, and PubMed databases. The protocol for this research has been registered in the PROSPERO international database under registration number CRD42024532843. Articles that examined the association between perirenal fat and atherosclerosis, and reported correlation coefficients (r), beta coefficients (β), and odds ratios (ORs) in cross-sectional and case-control designs, involving adult or pediatric human populations, were included. The pooled ORs (95% CI), the log OR, and its standard error were calculated.
Results
Following the identification of 10 eligible articles, meta-analysis and subgroup analysis were performed for different conditions, including adults, children, gender, atherosclerosis site, and comorbidity. One study reported the association between perirenal fat weight and atherosclerosis, while the remaining articles measured PRFT. The pooled estimated OR among 4767 adults was 1.24 (1.06–1.45) with I² = 83.6%. Among 929 adults, the pooled correlation coefficient (r) was 0.412 (p < 0.0001, I² = 63.3%). Among 1221 children, it was 0.291 (p < 0.0001, I² = 0%).
Conclusion
PRFT is significantly associated with carotid intima-media thickness, suggesting its potential as a non-invasive biomarker of atherosclerosis. Further large-scale, longitudinal studies are needed to confirm its predictive value.
Introduction
Atherosclerosis is a well-recognized chronic inflammatory arterial vascular disease characterized by the accumulation of lipids, fibrous elements, and calcification in the large arteries. 1 It is a leading risk factor for cardiovascular diseases (CVDs), ranking as one of the most common causes of death worldwide, with mortality rate of 34.9%. 2 With an age-standardized prevalence ranging from 5881.0 per 100,000 in South Asia to 11,342.6 per 100,000 in Central Asia in 2023, 2 atherosclerosis remains a major global health concern despite recent declines in clinical manifestations such as ischemic heart disease, stroke, and peripheral arterial disease.3–5 In the last decades, ∼9% of (CVD) deaths have been observed to surpass the expected mortality rate. 6 Moreover, atherosclerosis might also be able to impact the development and risk of other CVD risk factors, such as hypertension, and is associated with increased body mass index.7–10
Obesity has become one of the major contributors to the pathogenesis of atherosclerosis.11–14 However, intra-abdominal fat, according to recent research, is a better predictor of CVD risk and has a higher metabolic activity that can impact the development of cardiometabolic disorders, including hypertension and atherosclerosis.15,16 Perirenal fat thickness (PRFT) represents a fat pad located within the retroperitoneal space surrounding the kidneys and is bound by renal fascia. This anatomical aspect can be useful in the radiological diagnosis of the exact position of the kidneys. 17 In addition, such fat depositions can easily be detected by ultrasound studies, which are more available and economically viable compared to other radiological diagnostic tools. 18 A number of studies use surrogate markers such as carotid intima-media thickness (IMT), coronary artery calcium scores, ophthalmic artery-resistive index (OARI), and arterial stiffness to detect atherosclerosis.19–22 These indicators are widely applied in clinical and research settings due to their non-invasive nature and established association with cardiovascular risk. 23 However, some prior evidence suggests PRFT as a possible surrogate marker for atherosclerosis and CVD.24,25 The potential relationship between PRFT and the risk of atherosclerosis and CVD, as observed with carotid IMT, has been studied in previous studies. However, those studies have focused on different populations.24,26–28
The exact role of PRFT in the development of atherosclerosis is important to understand for the management and prevention of its complications. Moreover, PRFT may be an invaluable marker for the diagnosis of atherosclerosis directly. The sensitivity and specificity of PRFT in identifying subclinical atherosclerosis were previously reported to be 66.7% and 76.2%, which is superior to the sensitivity and specificity of other diagnostic biomarkers of atherosclerosis. 24 Thus, we aimed to systematically review evidence from observational studies regarding this association. The outcomes of this review are likely to provide important insights into the complex relationship between PRFT and the risk of atherosclerosis.
Materials and methods
This study was designed to investigate the relationship between perirenal fat and atherosclerosis based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) checklist. The protocol of this research is registered in the Prospero international database with the code CRD42024532843.
Search strategy
A comprehensive search was conducted among articles published in Scopus, Web of Science, Cochrane Library, and PubMed databases (via keywords and MeSH terms) until 2 July 2024. To find more eligible articles, the reference lists of included articles were manually screened. The search keywords were a combination of Peripheral Arterial Disease, Arteriosclerosis, Atherosclerosis, Cardiovascular, Vascular Calcification, Remodeling, Tunica Intima, Carotid Intima-Media Thickness, fat, fat thickness, adipose tissue, fat tissue, surrounding fat, renal size, perinephric, perirenal, and renal size. Figure 1 shows the step-by-step implementation of the search strategy.

PRISMA flow chart. The flow chart represents the number of studies evaluated according to PRISMA guideline.
Eligibility criteria
All English-language human studies that correlated perirenal fat (thickness or weight) with atherosclerosis and other indicators, such as arterial thickness or stenosis, were included in this systematic review.
Study selection
All search and screening steps were done by two separate reviewers. In cases of disagreement, they were resolved by holding a meeting with third reviewer. The quality of the articles was evaluated with the help of the Newcastle-Ottawa Scale (NOS) for observational studies and adapted version for cross-sectional studies. The NOS scale examines the possibility of bias in observational studies in terms of three areas of selection, comparability, and outcome; and obtains a range of scores from 0 to 9. Score of 7–9, 4–6, and 0–3 are considered excellent, moderate, and poor, respectively. In the adapted version of The NOS scale for cross-sectional studies, articles are given a score of 0–7. The score of 7 is considered as good quality.29,30 Table 1 represents quality assessment of the included studies (via the NOS tool).
Quality assessment of the included studies (the NOS tool).

NOS: Newcastle-Ottawa Scale.
Data extraction
The following data were extracted from each article by two reviewers separately: first author, year of publication, country, population, age of subjects, thickness or weight of perirenal fat, main findings of the research including correlation coefficient (r), regression coefficient (β), odds ratio (OR) (95% CI), and adjusted variables in the analysis.
Definition of terms
The protocols used to measure the indices of atherosclerosis and perirenal fat in different articles are almost similar to each other and are generally performed by the same operator(s). Therefore, we considered the following protocols to measure the mentioned parameters as a reference:
Perirenal fat thickness using CT scan: the maximum average distance between the posterior wall of the kidney (right, or average if both sides) to the inner wall of the abdomen in the supine position. 35
Perirenal fat thickness using ultrasound: by an ultrasound technician with a gentle pressure of 3–5 MHz transducer on the skin and measuring the inner surface of the skin to the posterior perinephric space (right or average of both sides). 28
Perirenal fat weight: by autopsy by a trained technician and accurate weighing with Sunford® digital balance, model FEH5000. 34
Carotid intima media thickness with ultrasound: in the supine position of the patient with head slightly upward or hyperextension towards the contralateral side and with the help of gentle pressure 7.5–12 MHz transducer in the one centimeter proximal to common carotid bifurcation by calculating the distance between the media-adventitia interface and the lumen-intima interface in the right carotid or the average of both sides. 36
Coronary artery stenosis using angiography: Coronary artery stenosis with the help of serial cutting from the autopsy sample and its histological and microscopic study. 32
Arterial calcification score using CT scan: A non-invasive measure of coronary artery calcium using CT imaging, calculated by summing the area of calcified plaques multiplied by a density factor, as defined by the Agatston method. 37
Ophthalmic artery resistance index with ultrasound: In the supine position with closed eyes using a 7.5 mHz transducer and calculating ophthalmic artery resistance index with a minimum pressure of the transducer on the upper eyelid. 26
Quantitative analysis
All quantitative analysis was performed using Stata software version 17. In order to investigate the main objective of this meta-analysis study, the pooled ORs (95% CI), the log OR and its standard error was calculated. The Fisher z transformation was used to calculate pooled correlation coefficient (r). 38 If an article reported beta coefficient instead of correlation coefficients (r), the beta coefficient was converted to r using the following formula 39 :
r = 0.98β + 0.05λ (if β is positive, λ = 1; if β is negative, λ = 0)
Obvious heterogeneity is defined as an I2 value higher than 50% and an I2 value less than 50% is considered to indicate no significant heterogeneity, respectively. In case of significant heterogeneity, estimates pooled using the random-effect model. Otherwise, the fixed model was used. In order to identify the source of heterogeneity, subgroup analysis was performed based on gender, comorbidity, and site of atherosclerosis. P-values less than 0.05 were considered statistically significant and Publication bias was calculated using Egger's test. The trim-and-fill-method was performed in a case of possible publication bias.
Results
Figure 1 shows the schematic summary of the study selection process. At the end of the primary search, a total of 577 articles were initially identified. After removing 144 duplicates, the remaining articles underwent a screening process based on their titles and abstracts. Non-English language articles, in vitro studies, case reports, reviews, editorials, commentaries, correspondence, and posters were excluded. This left 35 articles for full-text review. Of these, 23 were excluded for the following reasons: unrelated content (N = 21) and lack of access to full text (N = 2). Ultimately, 10 articles were included in the study.18,24–28,31–34 Among the 10 observational studies included, there was one case-control study, one cohort study, and eight cross-sectional studies. Geographically, three studies were conducted in Spain, two in Italy, and one each in China, Egypt, the United States, Nigeria, and Thailand. Only one study investigated the relationship between perirenal fat weight and atherosclerosis, while the others focused on PRFT in relation to atherosclerosis. Various modalities were used to measure perirenal fat, including CT scans,24,27 ultrasound,18,25–27,31–33 and autopsied perirenal fat weighing. 34 Two studies were performed in children, while the remaining studies were conducted in adults. All the included studies reported a significant relationship between perirenal fat and atherosclerosis or its representative indexes. More detailed information about the included articles is presented in Table 2.
Characteristic of included studies.

CIMT: carotid intima media thickness; PRFT: perirenal fat thickness; OARI: ophthalmic artery resistance index; OR: odds ratio; CT-scan: computed topography scan; BMI: body mass index; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; SCCA: subclinical carotid atherosclerosis; TG: triglyceride; TC: total cholesterol; LDL-c: low-density lipoprotein; HDL-c: high density lipoprotein; UA: uric acid; HOMA-IR: homeostatic model assessment for insulin resistance; SFA: subcutaneous fat area; VFA: Visceral fat area; LCX: Left circumflex artery; RCA: right coronary artery; LAD: left anterior descending artery; T2DM: type 2 diabetes mellitus.
Meta-analysis
The pooled estimated correlation coefficient among 1221 children from two studies28,33 was 0.291 (p < 0.0001, I2 = 0%). Among 929 adults from five studies,18,24–26,31 the pooled estimated correlation coefficient was 0.412 (p < 0.0001, I² = 63.3%) (Figure 2). According to Egger's test (p = 0.531), no publication bias was detected. To identify the source of heterogeneity, a subgroup analysis was performed based on comorbidity and the site of atherosclerosis. However, due to an insufficient number of studies in each subgroup, the analysis could not determine the source of heterogeneity (Table 3). According to Table 3, male gender and asymptomatic subjects showed no significant relationship between PRFT and atherosclerosis.

Forest plot of association between perirenal fat thickness and atherosclerosis with subgrouping based on comorbidity. ES: effect size (fisher z); CI: confidence interval.
Subgroup analysis of perirenal fat thickness with atherosclerosis.

PRFT measured using sonography in these studies.
PRFT measured using CT-scan in these studies.
PRFT measured using CT-scan and sonography in these studies.
PRFT: perirenal fat thickness; CIMT: carotid intima-media thickness; OARI: ophthalmic artery-resistive index.
The pooled estimated OR with a 95% confidence interval (CI) among 4767 adults from four studies24,26,27,32 was 1.24 (1.06–1.45) with I2 = 83.6% (Figure 3). Egger's test (p = 0.022) indicated possible publication bias for the association between PRFT and atherosclerosis in adults. After applying the trim-and-fill method, the overall effect size (ES) was adjusted to 1.95 (1.066–1.324). Excluding the study by Hazem et al., 32 which had a large 95% CI, the pooled estimated OR (95% CI) was 1.19 (1.07–1.32) with I² = 74.9%. Based on Table 3, only carotid intima-media thickness (CIMT) had a significant relationship with perirenal fat (OR 1.177, 95% CI: 1.103–1.257, p < 0.0001).
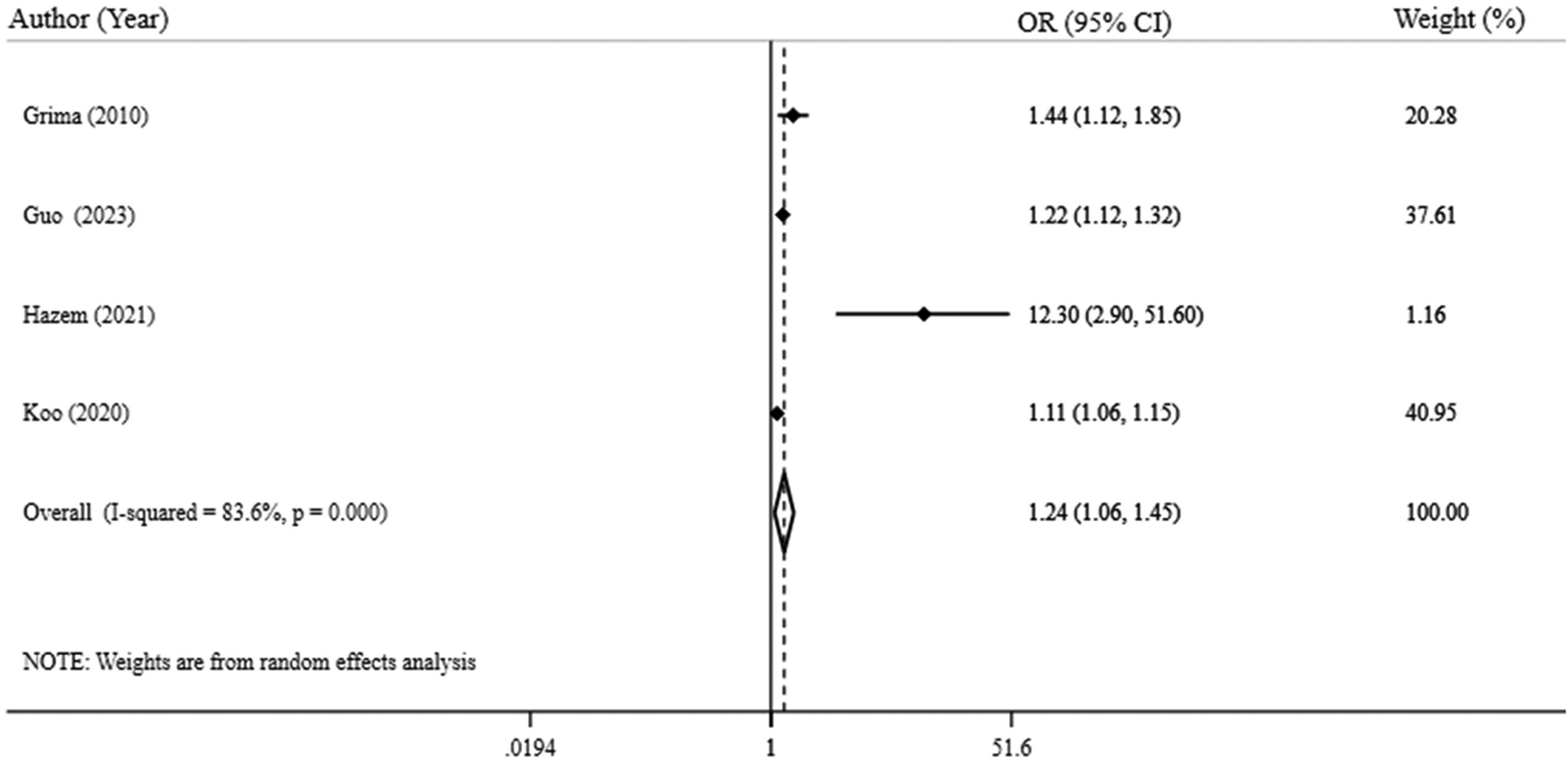
Forest plot of association between perirenal fat thickness and atherosclerosis. OR: odds ratio; CI: confidence interval.
Discussion
In this systematic review and meta-analysis of observational studies, we found that PRFT is significantly and positively associated with CIMT, a well-established marker of atherosclerosis in the overall adult population. Known predictor of atherosclerosis, was significantly positively correlated with PRFT in adults. However, this association was not observed in subgroup analyses of male participants or asymptomatic individuals, suggesting possible variation by sex or symptomatic status. In terms of correlation coefficients, both adult and child populations tended to have a greater impact on the development of atherosclerosis. The results of our meta-analysis, which assessed both ORs and ESs of the included studies, consistently indicated that PRFT significantly affects the development of atherosclerosis. According to the results of our study, although we found a positive correlation between PRFT and atherosclerosis, the variability in study populations, imaging methods, and comorbidities reflects the complexity of this relationship.
Many studies have investigated the possible association between atherosclerosis and perirenal adipose tissue thickness, especially in the last decade. However, the target groups of these studies differ in terms of age, sex, and comorbidities. It should be noted that perirenal adipose tissue thickness can be measured using different imaging techniques, such as ultrasound, CT scan, and MRI. Nevertheless, in the studies included in our systematic review and meta-analysis, PRFT was assessed using ultrasound and CT scan, mainly ultrasound The reason for this may be that ultrasound is more accessible, cheaper, and more suitable for large-scale imaging needs.40,41
Prior research literature has demonstrated that both peri- and intra-organ fat depots may be associated with CVD risk. 42 However, although the potential role of visceral adipose tissue in atherosclerosis and cardiovascular risk has been widely recognized, 43 to the best of our knowledge, no previous research has conducted a systematic review and meta-analysis specifically evaluating the correlation between perirenal fat and atherosclerosis. Additionally, numerous studies have indicated that regional adiposity may be a more accurate predictor of atherosclerosis than generalized adiposity. 44 Furthermore, a recent meta-analysis reported increased epicardial fat tissue thickness among patients with metabolic syndrome. 45 Contrary to our findings, a systematic review by Rosa et al. found no significant association between epicardial fat thickness and the risk of stroke, a potential complication of atherosclerosis. 46
Moreover, the relationship between PRFT and atherosclerosis was investigated among different subgroups in our meta-analysis. Consistent with the understanding that HIV-infected patients are potentially more susceptible to cardiovascular disorders, including atherosclerosis, 47 our analysis showed a significant association between atherosclerosis predictors, such as CIMT and the aortic arch calcification index (OARI), and PRFT [ES 0.54, 95% CI: 0.38–0.70, I² = 0.00%]. It should be noted that antiretroviral therapy for HIV patients can lead to lipodystrophy and its related cardiometabolic complications, including atherosclerosis. 48 Previous research indicates that PRFT tends to manifest earlier than fat accumulation in other body regions. 49 Regarding healthy and asymptomatic participants, our study found no significant association. The limited number of studies in this subgroup and the heterogeneity of these populations may explain these results [ES 0.60, 95% CI: −0.31–1.51, I² = 82.6%]. Another important subgroup in our meta-analysis was diabetic patients.
Atherosclerosis can be measured using various diagnostic tools. CIMT is recognized as one of the main surrogate markers for atherosclerosis. The CIMT is determined by measuring the distance between the innermost layer of the carotid artery and the middle layer, known as the intimal-luminal and medial-adventitial interfaces, using carotid ultrasound. 19 However, as mentioned in our study, the diagnosis of atherosclerosis can also be determined using other indicators, including coronary artery calcification and the OARI.50,51 Notably, previous data have shown that OARI can also be an important predictor of CIMT. 26
Our systematic review showed that in addition to the thickness of this fat deposit, the weight of perirenal fat also predicted coronary artery stenosis. Accordingly, Prompetch et al. stated that the weight of mesenteric and perirenal fat was better correlated with atherosclerosis compared with other visceral fat deposits (10). However, due to the limited availability of data, we are unable to perform a comprehensive meta-analysis on the weight of perirenal fat.
To our knowledge, the present study is the first meta-analysis to examine the association between perirenal adipose tissue thickness and atherosclerosis among research literature. This study also, highlights a notable strength in its focus on PRFT as a non-invasive marker associated with established surrogates of atherosclerosis, including CIMT and arterial calcifications. Incorporating data from multiple studies, our findings suggest that PRFT may play a significant role in determining cardiovascular risk. PRFT assessment through ultrasound presents several benefits, including affordability, wide availability, and straightforward implementation, which enhances its utility in everyday clinical practice and in settings with limited resources. The emphasis on a clinically feasible and scalable risk marker underscores its practical significance and contribution to preventive cardiovascular care.
Despite the above advantages of our study, some limitations should be considered. The number of studies included in the subgroup meta-analysis was not notable enough. Moreover, in our meta-analysis, not all publications used similar imaging techniques to measure perirenal adipose tissue thickness. Thus, there is a known considerable heterogeneity in our results, which may be due to the observational design of the included studies. Moreover, although the results of our meta-analysis were statistically significant, the strength of the observed association between PRFT and atherosclerosis is modest. These findings should therefore be interpreted with caution, particularly in the context of clinical significance. This small yet significant association underscores the role of PRFT as a potential contributing factor in the multifactorial pathogenesis of atherosclerosis, while also highlighting the necessity for larger, more robust studies to validate these findings.
Conclusion
In conclusion, our findings suggest that PRFT shows a significant association with markers of atherosclerosis, such as CIMT, across various populations. While these results indicate PRFT's potential role as a non-invasive biomarker, it is essential to note that further research is necessary to establish its predictive capabilities definitively. Observational studies with larger sample sizes, diverse diagnostic methods, and longitudinal designs will be crucial in substantiating the clinical utility and relevance of PRFT in atherosclerosis risk assessment.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251346566 - Supplemental material for The correlation of perirenal fat and atherosclerosis: A systematic review and meta-analysis
Supplemental material, sj-docx-1-sci-10.1177_00368504251346566 for The correlation of perirenal fat and atherosclerosis: A systematic review and meta-analysis by Melika Golmohammadi, Parynaz Parhizgar, Farid Javandoust Gharehbagh and Legha Lotfollahi in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504251346566 - Supplemental material for The correlation of perirenal fat and atherosclerosis: A systematic review and meta-analysis
Supplemental material, sj-docx-2-sci-10.1177_00368504251346566 for The correlation of perirenal fat and atherosclerosis: A systematic review and meta-analysis by Melika Golmohammadi, Parynaz Parhizgar, Farid Javandoust Gharehbagh and Legha Lotfollahi in Science Progress
Footnotes
Acknowledgements
Not applicable.
Author contributions
MG and LL conceptualized the study. MG, LL, and PP researched and screened data. MG and PP drafted the initial manuscript. PP analyzed the data. MG and PP generated figures and tables. FJG revised the manuscript. LL edited, finalized, and supervised the manuscript. All authors reviewed and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.