
Abstract
Objective
The aim of this study was to investigate the association between angiotensin I converting enzyme gene polymorphism and coronary artery disease in the Pakistani population, given the early onset and aggressive nature of coronary artery disease in this region.
Methods
A case-control study was conducted involving 540 Pakistani patients with established coronary artery disease and 224 healthy controls. DNA samples were amplified using polymerase chain reaction with primers targeting the insertion (I)/deletion (D) sites of intron 16 of the angiotensin I converting enzyme gene. The polymerase chain reaction products were analyzed for the presence of 490-bp (II), 190-bp (DD), or both (ID) fragments.
Results
The frequency of the homozygous insertion (II) genotype was 9% in the control group and 25% in coronary artery disease patients, while the homozygous deletion (DD) genotype was 26% in controls and 24% in patients. A significant association was found between the angiotensin I converting enzyme II genotype and coronary artery disease (odds ratio = 7.963, p < 0.0001).
Conclusion
The angiotensin I converting enzyme II genotype is significantly associated with an increased risk of coronary artery disease in the Pakistani population, suggesting a potential genetic predisposition to early and aggressive coronary artery disease in this group.
Keywords
Introduction
Coronary artery disease is one of the most common cardiac disorders with more than 60% of its global burden occurring in developing countries and is projected to become the leading cause of global morbidity and mortality by 2020. 1 According to the World Health Organization, the number of deaths from cardiovascular diseases (CVDs) in 2004 was 17.1 million and it is predicted that by 2030, about 23.6 million deaths will be reported due to CVDs, mainly from CAD and stroke. 2 The broad clinical spectrum of coronary artery disease (CAD) includes angina and myocardial infarction (MI) and is caused by atherosclerosis, a degenerative disease condition affecting arterial vessel walls. 3 A population-based survey conducted on CAD in Pakistan has shown an overall prevalence of 26.9% in men and 30% in women. This indicates that one in four middle-aged adults in Pakistan has prevalent coronary artery disease with the risk being uniformly high in the young population. 4 It has also been shown that 50% of patients presenting with an acute coronary event in Pakistan suffer from premature coronary artery disease: additionally, an unusually high prevalence of acute MI and high-risk coronary artery anatomy also points to a more aggressive pattern of disease in this population. 5 This pattern of coronary artery disease in Pakistan with a predilection for the onset of disease suggests the importance of genetic components along with interaction of the environmental factors.
An understanding of the genetic factors involved in CVDs could eventually lead to improved therapeutic as well as diagnostic and predictive tools. Many studies have focused on the involvement of the renin-angiotensin system in the development of CVDs, especially the angiotensin I converting enzyme (ACE). ACE plays a key role in blood pressure regulation and in the maintenance of cardiovascular homeostasis. It catalyzes the conversion of angiotensin I to angiotensin II, a potent vasoconstrictor, and is involved in the degradation of the vasodilator bradykinin. 6 Rigat et al. 7 reported that the ACE gene contains an Alu insertion/deletion (I/D) polymorphism in intron 16. This polymorphism was shown to be associated with variability in ACE plasma levels and studies reported that the homozygous deletion (D/D) genotype increases plasma ACE levels.7,8 This led to studies to investigate whether this polymorphism was associated with a predisposition to various CVDs. The DD genotype was found associated with a higher risk for MI and CAD in some studies,9–11 whereas other studies have shown that the DD genotype does not predispose towards CAD 12 and that in some populations the I allele may confer protection against CAD. 13 In another study, the homozygous insertion (II) genotype was associated with a delay in the onset of acute coronary syndrome. 14
Here we present the result of a study carried out to investigate the association of the ACE I/D polymorphism in patients with CAD in Pakistan.
Materials and methods
Subjects
The patients were recruited from the Department of Cardiology, Islamabad, Pakistan from the year 2005 to 2008 from the outpatient department. The present study is a case-control study. The sample size was calculated using a power analysis to ensure statistical significance. Based on a significance level (α) of 0.05, a power of 80%, and an estimated effect size from prior studies of the association between ACE gene polymorphism and CAD, the required sample size was calculated using standard formulas for case-control studies. 15 The calculation suggested that a minimum of 200 CAD patients and 200 healthy controls would provide adequate power to detect a meaningful difference in the genotype distribution between the groups. To account for potential dropouts and incomplete data, the sample size was increased, resulting in the inclusion of 540 CAD patients and 224 healthy controls. The patients included were between the age group of 25 to 70 years and had angiographically proven CAD (≥ 60% stenosis of ≥ 1 major coronary artery angiography). Patients selected were with the absence of significant comorbid illness, as determined by a clinician. The present study included 540 CAD patients (435 males and 105 females). Fasting blood samples were tested for levels of: total cholesterol, high-density lipoprotein, low-density lipoprotein, cholesterol, and triglycerides. Creatinine and uric acid levels were also tested. Waist-hip ratio and body mass index (BMI) were calculated for all subjects. A history of diabetes and hypertension was also taken. Smoking habits (smoker and non-smoker), family history, and consanguinity were self-reported by study participants. The reporting of this study conforms to STROBE guidelines. 16
The inclusion criteria for ethnically matched controls (n = 224) were the normal electrocardiogram and exercise tolerance test and declared as not suffering from CAD by a cardiologist. Controls were matched to patients for age, gender, and ethnic background and ≥ 2 of the following risk factors:
hypertension diabetes BMI smoking family history of premature CAD dyslipidemias
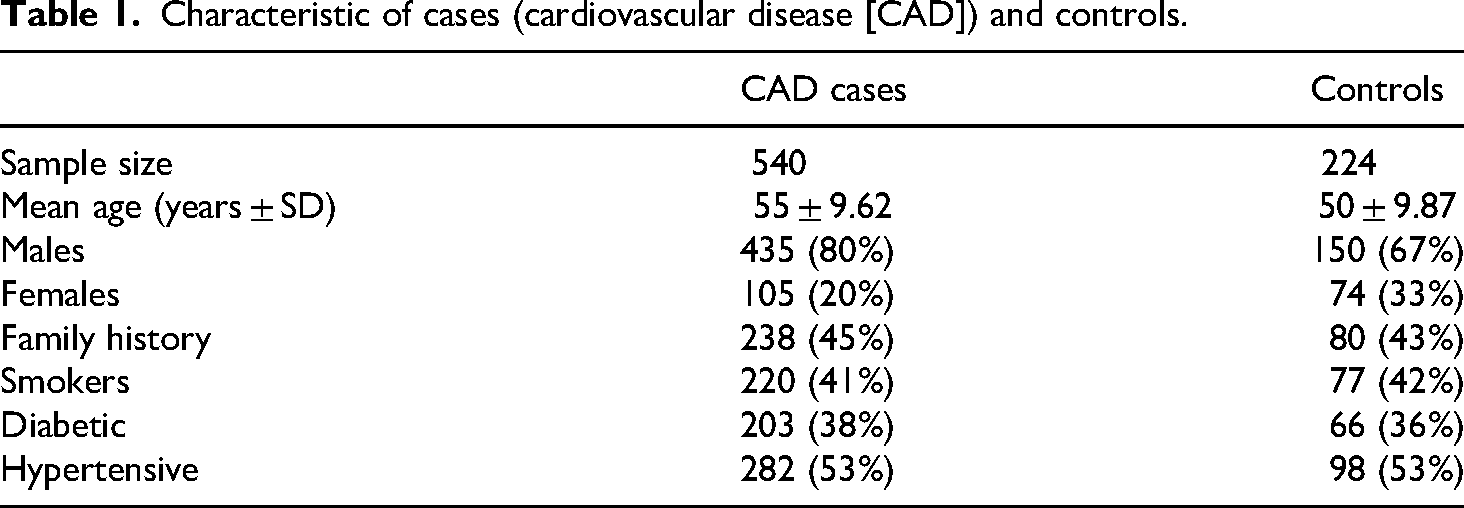
All subjects were Pakistani and gave their written informed consent to take part in this study. The study was approved by the Ethical Committee of the parent organization—Institute of Biomedical and Genetic Engineering (Reference No. IBGE/IEC/04/01/16). All research was performed in accordance with relevant guidelines/regulations in accordance with the Declaration of Helsinki 1975 as revised in 2024. The demographical characteristics of cases and controls are listed in Table 1. All details of cases and controls are de-identified for publication purposes.
Characteristic of cases (cardiovascular disease [CAD]) and controls.
Genetic analyses
DNA was extracted from 10 mL of peripheral venous blood by the phenol-chloroform extraction method. 17 The ACE I/D polymorphism was typed by polymerase chain reaction (PCR) using the primers ACE F 5′-CTGGAGACCACTCCCATCCTTTCT-3′ and ACE R 5′-GATGTGGCCATCACATTCGTCAGAT-3′. 7 The PCR conditions were as described by Batzer et al. 18 The amplified PCR product was size fractionated on a 1.5% agarose gel containing ethidium bromide and visualized using UV transillumination (Supplemental Figure 1).
Statistical analyses
The one-way parametric analysis of variance option of the Statistical Package for Social Sciences (SPSS; version 13) was used to calculate significant variation between the genotype and allele frequencies in the patients and controls. 19 Odds ratios (ORs) with 95% confidence intervals (CIs) were estimated using the calculator for CIs (http://www.hutchon.net/ConfidOR.htm) for OR. 20 The chi-square test and ORs in patients and controls are calculated. The Hardy-Weinberg equilibrium was calculated by an online calculator (http://www.oege.org/software/hwe-mr-calc.shtml).
Results
In this study, CAD was significantly correlated with sex (more frequent in males) and increased BMI of the patients as well as smoking and hypertension. The association of CAD with diabetes was statistically insignificant. The ACE alleles were in Hardy-Weinberg equilibrium in the patients but not in the controls, where an excess of heterozygotes was observed (Table 2). The allele frequencies of the ACE gene I/D polymorphisms in CAD patients and controls are presented in Table 3. The ACE I allele was more frequent in the patients than in the controls (p < 0.000). The frequencies of the three ACE genotypes, II, ID, and DD, along with the results of the chi-square test and ORs in patients and controls are listed in Table 4. The ACE homozygous I/I polymorphism was observed in 25% of the CAD patients compared to only 4% in the controls. This difference was highly significant (p < 0.0001) and an OR of 7.963 (CI = 3.97–15.95; p < 0.0001) was obtained for this genotype. The difference between patients and controls for the homozygous D/D genotypes was not significant (p = 0.33; OR = 1.11). A protective effect was observed for the ID genotype, which was present at a significantly higher frequency in the controls as compared to the CAD patients (p < 0.0001; OR = 0.356, CI = 0.25–0.51, p < 0.0001).
Hardy-Weinberg equilibrium of cases (cardiovascular disease [CAD]) and controls.

Alleles of cases (CAD) and controls.

CAD: cardiovascular disease; I: insertion; D: deletion.
Genotypes, χ2 and OR of cases (CAD) and controls.
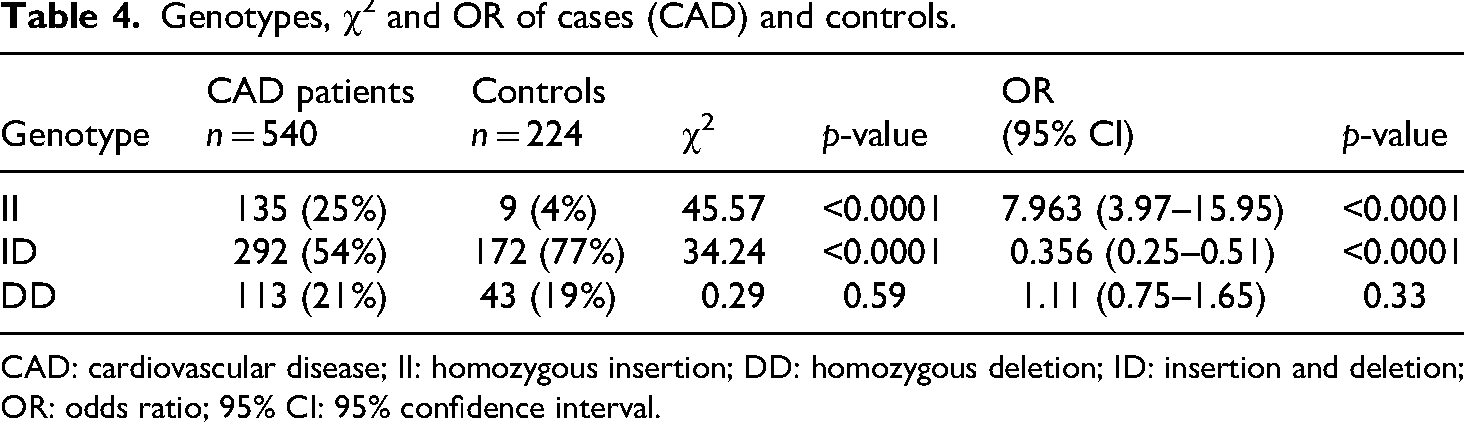
CAD: cardiovascular disease; II: homozygous insertion; DD: homozygous deletion; ID: insertion and deletion; OR: odds ratio; 95% CI: 95% confidence interval.
Discussion
CAD has a complex etiology, with various environmental and genetic factors contributing to the pathogenesis of the disease state. ACE is one of the most widely investigated candidate genes for CAD and conflicting results have been obtained from different studies. A meta-analysis of 118 studies involving 43,733 CAD cases and 82,606 controls 21 demonstrated evidence of a modest positive association of the ACE I/D polymorphism with CAD. To date most studies have reported an association of the homozygous deletion variant, DD with susceptibility to various CVDs such as MI, CAD, and left ventricular hypertrophy by several groups. A study carried out in Iranian patients did not find an association of the DD genotype with CAD although the frequency of the ID genotype was significantly raised and the II genotype was significantly reduced in the patients as compared to the controls. 22 Our study on 540 CAD patients and 224 healthy controls with at least two risk factors for CAD has also shown that the DD genotype is not associated with CAD in this population. A strong association of the II genotype with susceptibility to CAD was observed and results indicate that individuals with the II genotype are over seven times more likely than ID or DD individuals to develop CAD. The ID genotype is significantly more prevalent in the control population and seems to have a protective effect (OR = 0.36, p < 0.0001). There was no difference in the distribution of the ACE I/D genotypes between the male and female subjects. Interestingly, the control population which was ethnically matched with the patient pool, is not in Hardy-Weinberg equilibrium due to an excess of heterozygotes (Table 1). It may be argued that it is the protective effect of the ID genotype that is resulting in the selection of individuals with this genotype. Previous studies in Pakistani populations have shown a deviation from HWE due to an excess of homozygotes and generally attributed amongst other factors to centuries of inbreeding amongst individuals as well as low-resolution typing methods.23,24 In a recent study on diabetic cases in the Pakistani population it is reported that ACE I/D polymorphism influences the risk of diabetes in CVD patients and ACE II increases this risk by ∼2 fold. 25 In the present study, diabetes was a risk factor for CVD as described in Table 1. There is no significant difference in diabetics between the cases and control percentage in the total studied samples. No significant association due to only diabetes risk factors is reported in the present study.
In different studies, an association between this polymorphism and coronary atherosclerosis has been reported in populations ranging from 152 to 1162 participants26–28 and some other studies did not report such an association.29,30 Contrary to the present finding in another study on the Indian population the ACE DD polymorphism was found associated with CAD. 11 This may be due to the reason that the samples of the Indian population are having obesity too and in Pakistani samples the BMI and obesity are not very significant in the studied population. It is suggested that these inconsistent results could be due to the genetic differences among various populations studied and other inclusion criteria of samples. Further, they have recommended that potential gene-gene and gene-environment interaction should be considered 31 in such cases. The strong association observed between the ACE I/I genotype and patients with ischemic heart disease from Pakistan in the present study supports the above validation. Interestingly, in a previous study on Pakistani hypertensive young patients, a similar significant association of the I/I genotype was reported. 32
Given the potential for artificial effects, it is critical to ensure that the control group is comparable to the patient population in terms of ethnicity and genetic predisposition. For instance, studies by Zaidi et al. 33 and Iqbal and Ashraf 34 provide valuable data on the distribution of ACE I/D polymorphism in Pakistani populations. These studies show that the frequency of I/D heterozygotes in Pakistani controls is indeed significant and can serve as a reliable comparison to the patient group in this study. Similarly, Ali et al. 35 have examined the correlation between ACE gene polymorphisms and CVDs in the South Asian population, providing insight into how genetic variation in this population impacts disease risk.
Despite the strengths of this study, several limitations are noted. First, while the sample size of 540 CAD patients and 224 controls was calculated to ensure adequate statistical power, the study was restricted to a specific population in Pakistan. Therefore, the results may not be directly generalizable to other populations with different genetic or environmental factors. The findings in this study are specific to the Pakistani population, which has a unique genetic background and a history of consanguineous marriages. Further studies in diverse populations are needed to confirm the validity and relevance of these results in different ethnic and geographic groups.
Second, although the study investigates the association of the ACE gene polymorphism with CAD, it does not account for the full spectrum of potential confounding variables. Factors such as lifestyle, diet, and environmental exposures could also influence CAD risk, and these were not controlled for in this study. Additionally, the study did not examine the impact of gene-environment interactions, which could provide deeper insights into the role of ACE gene polymorphisms in CAD development.
Secondly, while the study demonstrates a strong association between the I/I genotype and CAD, the exact mechanism by which the ACE gene polymorphism contributes to CAD risk remains unclear. It has been suggested that corticosteroid hormones could influence ACE gene activity, 21 but further studies are needed to investigate the underlying biological mechanisms and their interactions with other risk factors such as hypertension, obesity, and diabetes.
Lastly, this study did not include long-term follow-up or functional studies to assess the impact of the ACE I/I genotype on disease progression or treatment outcomes. Longitudinal studies with larger, diverse cohorts are essential to explore the temporal relationship between ACE polymorphisms and CAD, as well as to evaluate the potential for personalized treatment strategies based on genetic markers.
Conclusion
Despite these limitations, this study provides valuable insights into the association between ACE gene polymorphism and CAD in the Pakistani population, highlighting the role of genetic factors in the early onset and aggressive nature of CAD observed in this region. Our findings add to the growing body of evidence supporting sex-specific genetic risk factors for CAD and underscore the importance of considering metabolic factors, such as hypertension, obesity, and diabetes, when assessing genetic risk. By validating these findings in the Pakistani population, the study strengthens the case for incorporating genetic information into future CVD prevention and treatment strategies tailored to this region.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251338935 - Supplemental material for Association of angiotensin I converting enzyme gene I/D polymorphism and coronary artery disease in the Pakistani population
Supplemental material, sj-docx-1-sci-10.1177_00368504251338935 for Association of angiotensin I converting enzyme gene I/D polymorphism and coronary artery disease in the Pakistani population by Nusrat Saba, Sadia Rehman, Saeeda Munir and Amna Noor in Science Progress
Footnotes
Acknowledgements
The authors are thankful to IBGE for giving them all the facilities to carry out the work. We are also thankful to all the patients and controls for giving the blood samples for our study.
Ethical considerations
The ethics committee of the parent organization for the use of human subjects approved the study.
Consent to participate
Written informed consent from each participant was obtained before collecting blood samples and clinical information.
Consent for publication
Consent from each participant was obtained for publication of data.
Author contributions
NS carried out all the sampling, the molecular genetic studies, participated in the data analysis, and drafted the article. SR participated in the study design and helped to draft the article. SM participated in the design of the study and helped in molecular genetic studies. AN participated in sample records and helped with clinical information for studies. All authors read and approved the final article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data of cases and controls used in the present study are available with the corresponding author and can be reproduced when requested.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.