
Abstract
Objective
The study aimed to explore the predictors of vascular complications (VCs) associated with transradial access, as the occurrence and severity of these complications were found to be significantly lower compared to femoral access. However, it is important to note that the occurrence of these complications still has a negative impact on clinical outcomes. Nevertheless, there is limited available data on the predictors of complications specifically related to radial access.
Methods
A retrospective case-control study was conducted on individuals who underwent percutaneous coronary diagnostic or therapeutic procedures at Daping Hospital, following the inclusion and exclusion criteria. The study compared demographic characteristics, VC types, ankle brachial index (ABI), and severity of coronary artery stenosis between the two groups.
Results
We enrolled 300 subjects with VCs and 300 age- and sex-matched subjects without VCs as controls. There were no differences in the baseline characteristics or comorbidities between the groups. Compared to the control group, the VC group has a higher portion of left radial access (6.0%) and previous radial artery puncture history (29.7% vs. 18.3%, p<0.001). The ABI was significantly lower than the non-VC group (1.17 ± 0.17 vs. 1.23 ± 0.14, p<0.001). In the multivariate logistic regression analysis, several factors were found to be independently associated with the occurrence of VC. These factors include ABI (OR=0.060, 95% CI: 0.014–0.249, p<0.001), the procedure being performed by junior operators (OR=1.892, 95% CI: 1.314–2.745, p<0.001), and previous access on the same radial artery (OR=1.795, 95% CI: 1.190–2.707, p<0.01).
Conclusions
Patients who exhibit a lower ABI and have a history of prior radial access procedures may be at an increased risk of developing radial access VC. Therefore, it is recommended to routinely measure ABI prior to these procedures, as it may serve as a predictive tool for assessing the risk of VC.
Keywords
Introduction
Over the years, percutaneous coronary angiography has become widely utilized for the diagnosis of coronary artery diseases. 1 It is now common to access the heart via the peripheral artery during interventional cardiac procedures. As a means to mitigate access-site vascular issues and enhance patient comfort, transradial access has now become the standard technique employed in most catheterization laboratories for percutaneous coronary diagnostic and/or therapeutic procedures.2,3
The radial method has been associated with an increased risk of access crossover and procedural failure, which may require a more extensive learning process. Despite a gradual decrease in the frequency of radial-related vascular complications (VCs), their occurrence still has the potential to impact clinical outcomes and should be given greater consideration. 4 However, there is a lack of comprehensive data on the predictors of entry-site complications. Therefore, this retrospective case-control study was conducted to assess the predictors associated with transradial VC.
Methods
Study population
The present study was conducted as a retrospective observational single-center case control investigation, specifically chosen from the cardiovascular catheterization database of Daping Hospital, spanning the period from January 2019 to December 2021. The study encompassed consecutive patients diagnosed with coronary artery disease (CAD) who were admitted to our institution and underwent percutaneous coronary diagnostic or interventional procedures utilizing transradial access. Patients who underwent procedures via femoral access were deliberately excluded from the study. Patients with a history of documented radial artery thrombosis or prior surgical procedures in close proximity to the access site were also excluded from the study. Despite the potential benefits of distal radial access in reducing the risk of radial occlusion, we have chosen to exclude these cases from our study in order to minimize any potential bias. 5 Additionally, all CAD patients were advised to undergo an ankle-brachial index (ABI) measurement before the procedure.
Ankle brachial index measurement
A standardized oscillometric device was utilized to assess the blood pressure of the ankle and brachial artery in patients who were in a supine position following a period of rest lasting between five and ten minutes. The ABI was calculated using the established methodology, which involved dividing the highest systolic blood pressure recorded in the pedal and tibial arteries by the highest brachial systolic blood pressure value. 6 An ABI below 0.90 was classified as indicative of peripheral artery disease, while an ABI above 1.4 indicated a higher risk of cardiovascular issues. ABIs within the range of 0.9 to 1.4 were considered normal.7,8
Radial approach technique
Prior to the procedure, the Allen's test was routinely employed to assess the patient's suitability for radial artery catheterization. 9 In cases where the Allen test yielded abnormal results, the Barbeau test was conducted. 10 Ultrasound was not routinely utilized to evaluate radial artery blood flow or diameter before or after the procedure, unless specifically indicated. For radial artery catheterization, a specialized arterial puncture kit containing a plastic cannula and hydrophilic wire, as well as a long (16 cm) hydrophilic sheath (Radifocus, Terumo, Japan), was employed. Local anesthesia was administered using lidocaine. A standard practice involved the utilization of a singular 6F catheter sheath for both diagnostic and therapeutic procedures. Prior to diagnostic angiography, each subject received a combination of aspirin and a P2Y12 inhibitor (minimum loading dose of 300 mg clopidogrel or ticagrelor 180 mg if 3 days of pretreatment) unless there were high-risk factors for bleeding. During diagnostic procedures, a bolus of 2000 IU of unfractionated heparin was introduced through the sheath. For patients undergoing therapeutic procedures, a weight-adjusted bolus of heparin (ranging from 80–100 IU/kg) was administered at the beginning of the procedure, with additional doses given to maintain an activated clotting time between 250 and 300 s. Alternatively, in patients at high risk for bleeding, bivalirudin was administered through the sheath. A standard practice involved the regular administration of a 200 μg nitroglycerin drug through intra-arterial means to prevent radial artery spasm, unless contraindicated. Following the completion of the procedure, the arterial sheath was removed. To ensure hemostasis, a hemostatic radial compressor was utilized. The compression bandage was loosened after a period of 2 h and left in place for a duration of 3 to 4 h post-procedure. The right radial artery is usually the first choice for vascular access. If unsuccessful, other sites on the same arm are attempted before considering the left radial artery. In cases needing multiple access points during PCI, bilateral radial artery puncture is considered. Trans radial puncture and angiography procedures were conducted either by highly skilled operators with extensive experience (over 500 total cases) or under the supervision of senior operators in the case of trainee junior operators (with fewer than 500 total cases of trans radial puncture). The percutaneous coronary therapeutic procedures were conducted by experienced operators who had extensive experience with the radial route, having performed over 1000 cases of percutaneous coronary intervention. Vascular access site for the procedure was defined as the site of successful vascular entry of the sheath. The procedure time was calculated from the first radial artery puncture to catheter withdrawal.
Vascular complications definitions
VCs were operationally defined as any documented vascular damage identified through specific instrumental investigations. This encompassed various types of complications, such as vessel perforation, radial artery occlusion, arterial-venous fistula, pseudoaneurysm, arterial dissection, compartmental syndrome, local hematoma without documented specific vessel damage, as well as any other vessel damage or entry-site complication (e.g. access-site infections, peripheral ischemia, etc.). Radial artery bleeding and hematoma formation were visually assessed and classified according to the EASY criteria, Class I and II are considered minor, while III and above are major bleeding events.
11
The classification of VCs was further categorized into two groups:
Major complications, which necessitated surgical intervention and/or blood transfusions, or resulted in a decrease in hemoglobin levels of 3 g/dL or more. Minor complications, which necessitated instrumental investigations, were managed conservatively without resorting to surgical interventions or blood transfusions, and not resulting in a decrease in hemoglobin levels exceeding 3 g/dL.
2
The medical records underwent thorough examination by two experienced interventional cardiologists, who were entrusted with the ultimate determination of vascular complication occurrence and classification. The VCs were assessed and measured after hemostasis device removal within 24 h and twice daily over a period of 3 days, and again assessed at the one-month follow-up visit. Doppler ultrasound examinations of the radial artery to assess blood flow and detect potential occlusions, dissections, or the formation of pseudoaneurysms were used as indicated.
Ethics and data collection
This study was conducted in accordance with the ethical principles outlined in the Helsinki Declaration of 1975, as revised in 2013. The research protocol was approved by the institution's human research committee of the Daping Hospital (Clearance No.: 2022-221). All patients provided written informed consent for participation in clinical studies with their de-identified data to be used for future research purposes, and all procedures detailed herein were conducted in accordance with the approved guidelines. All patient data were de-identified to protect individual privacy by removing any potentially identifying information such as names, dates of birth, addresses, and other personal details before analysis. Demographic, baseline clinical, preprocedural, and vascular access characteristics, as well as angiographic and procedural data, were recorded in a dedicated database unanimously agreed upon by all center operators. To ensure the utmost accuracy, all data underwent a thorough double-checking process. The reporting of this study conforms to the Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 12
Statistical analysis
The categorical variables were summarized using counts and percentages. To compare mean values and percentages across different groups, χ2 tests were employed. The Kolmogorov-Smirnov test was utilized to assess the adherence of each variable to a Gaussian distribution. 13 Continuous variables that did not conform to a Gaussian distribution were expressed as medians (interquartile range, IQR) and were compared between two groups using the Mann-Whitney U test. 14 A multivariate analysis was conducted utilizing binary logistic regression to assess the predictive variables that may influence the incidence of VCs. Only those values that demonstrated a p value <0.05 in the univariable analysis were included in the multivariable model. All data were analyzed using IBM SPSS Statistics version 19.0 (SPSS, Chicago, IL, USA). A significance level of p < 0.05 (two-tailed) was deemed statistically significant for all tests.
Results
Baseline demographics
A total of 5387 consecutive patients who underwent percutaneous coronary diagnostic and/or therapeutic procedures at our hospital from January 2019 to December 2021 were included in our screening. The study population consisted of 300 individuals with VCs and 300 age- and sex-matched individuals without VCs, serving as the control group (Figure 1). Demographic and clinical characteristics of the two groups are presented in Table 1. Among the patient groups with or without VCs, there were 159 and 143 females, respectively, and the mean age was 66.7 ± 10.0 and 65.6 ± 9.7 years. The age, gender, body mass index, systolic blood pressure, and diastolic blood pressure at admission were found to be comparable between the two groups. Furthermore, no significant differences were observed in terms of cardiovascular risk factors such as diabetes, atrial fibrillation, hypertension, smoking/drinking habits, or prescription medicines including beta blockers, calcium-blockers, angiotensin-converting enzyme inhibitors and/or angiotensin receptor blockers, or diuretics. 85.3% of patients with VCs and 81.0% without VCs were treated with aspirin, while 46% and 42% of patients, respectively, received P2Y12 inhibitors (clopidogrel or ticagrelor). (refer to Table 1). Prior to PCI, each subject received a combination of aspirin and a P2Y12 inhibitor (minimum loading dose of 300 mg clopidogrel or ticagrelor 180 mg if 3 days less of pretreatment) unless there were high-risk factors for bleeding. Patients with atrial fibrillation were assessed for thrombotic risk using the CHA2DS2-VASc score, and those deemed at risk are prescribed oral anticoagulants (dabigatran or rivaroxaban) unless contraindicated. There were no statistically significant variations observed in the laboratory analyses, encompassing total cholesterol, low density lipoprotein cholesterol, high density lipoprotein cholesterol, triglyceride, creatinine, platelet counts, fasting glucose.

Study flowchart.
Baseline characteristics of the study participants.

Values are mean SD, median (interquartile range) or n (%). BMI, body mass index; ACEI, angiotensin-converting enzyme inhibition; ARB, angiotensin receptor blocker; TC, total cholesterol; LDL-c, low density lipoprotein cholesterol; HDL-c, high density lipoprotein cholesterol; TG, triglyceride; STEMI, ST-elevation myocardial infarction; NSTEMI, non ST-elevation myocardial infarction.
Vascular complications and consequences
The characteristics of the transradial access procedure are presented in Table 2. There were no significant differences observed in the prescription of intravenous heparin dose (p=0.273) or the proportion of bivalirudin use (p=0.730) between the VC and non-VC groups. Although the total procedure time was slightly longer in the VC group (p=0.013), angiography was successfully performed in all patients following successful cannulation.
The procedure characteristics of the study participants.
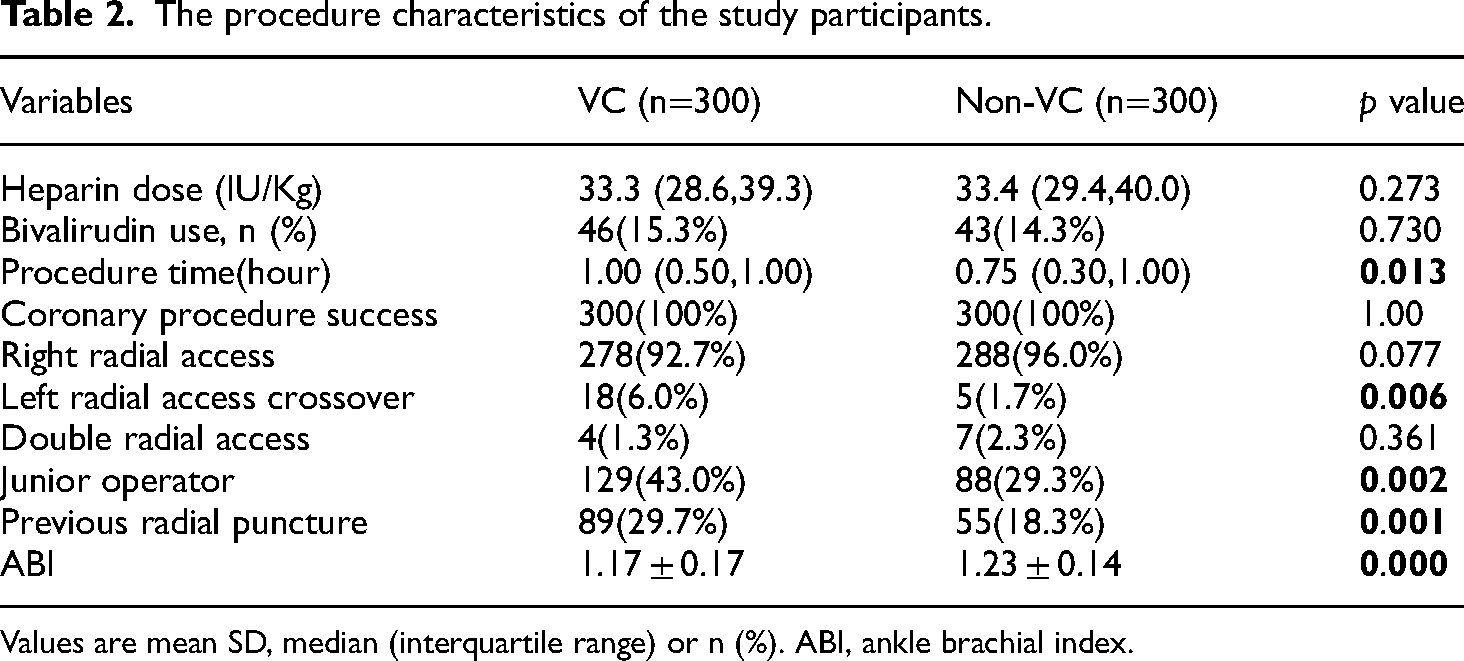
Values are mean SD, median (interquartile range) or n (%). ABI, ankle brachial index.
Among the patients who were enrolled in the study, the initial approach of using the right radial access was employed in 566 cases, accounting for 94.3% of the total. In the VC group, there was a slightly higher proportion (6.0%) of the need to switch to a secondary left radial access than the non-VC group (1.7%). In 11 patients (3.8%), both radial accesses were intentionally utilized. This included three cases where one-side radial artery total occlusion was present, and eight cases where the initial guide wire could not be passed due to arterial loops, tortuosity, aberrations, or arterial spasm. Notably, the VC group exhibited a higher rate (43%) of radial access performed by junior operators compared to the non-VC group (p<0.001). The ABI was found to be 1.17 ± 0.17 in the group of patients with VC, which was significantly lower than the group without VC (1.23 ± 0.14, p<0.001). Out of the studied patients, 15 individuals exhibited an ABI below 0.9, indicating peripheral artery disease, but only 7 of them complaint symptoms of lower limb claudication, while the rest were asymptomatic. A higher proportion of patients in the VC group (29.7%) had previous access on the same radial artery compared to the non-VC group (18.3%, p<0.001).
Among the 300 patients with VCs, the most common complications observed were swollen hands and local hematoma (90%) around the access site, primarily classified as minor (EASY I and II) without necessitating specific invasive treatments. EASY III-V grade bleeding was noted in a smaller subset of 16 cases, but were still amenable to conservative management strategies. Early radial artery occlusion within the first 24 h post-procedure was confirmed in 13 cases. However, spontaneous recanalization was observed in six of these cases by the 30-day follow-up. Luckily, most VCs were managed conservatively and resolved with compressive bandaging and pain relief, they significantly impacted patient comfort due to distress and edema, requiring attentive topical care. Notably, one case necessitated surgical intervention for a pseudoaneurysm, highlighting the spectrum of VCs from transient discomfort to conditions requiring immediate surgical repair.
Risks of vascular complication
Table 3 displays the angiographic findings, specifically pertaining to the interventional procedures. Notably, there were no statistically significant disparities observed in the rate of percutaneous coronary diagnostic or therapeutic procedures (p=0.739). To investigate the potential association between the occurrence of VC and the severity of coronary artery disease, the Gensini score and the number of diseased coronary arteries with luminal stenosis exceeding 50% were calculated to semi-quantitatively assess the severity of the coronary arteries. It is worth mentioning that the VC group exhibited a significantly higher prevalence of multi-vessel lesions, characterized by stenosis in more than one vessel (p=0.013). The Gensini score exhibited a slight increase, although lacking statistical significance, in the VC groups (p=0.069). In order to conduct a more comprehensive analysis of the factors that may impact the incidence of radial access VCs, we employed the occurrence of VCs as the dependent variable and considered other potential influencing factors, such as left radial access, multi-vessel lesion, ABI, junior operator, procedure time, Gensini score, and previous access on the same radial artery, which demonstrated statistical significance in the univariable analysis, as independent variables for the multivariate regression analysis. In this model, the study found that ABI was independently and negatively associated with the occurrence of VC (OR=0.060, 95% CI: 0.014–0.249, p<0.001). This suggests that subclinical peripheral arterial disease, as indicated by a low ABI, is the strongest predictor of vascular complications and should be given special attention during the procedure. Additionally, the involvement of junior operators in the procedure was also identified as a significant predictor of VC (OR=1.892, 95% CI: 1.314–2.745, p<0.001). Furthermore, a history of previous percutaneous radial access on the same artery (OR=1.795, 95% CI: 1.190–2.707, p=0.005) was also associated with the occurrence of VCs. The severity of coronary artery disease was assessed using the Gensini score and the number of diseased coronary arteries with more than 50% luminal stenosis. Logistic regression analysis revealed that neither the Gensini score (OR=0.993, 95% CI: 0.985–1.002, p=0.142) nor the presence of multi-vessel lesions (OR=1.795, 95% CI: 1.190–2.707, p=0.070) was significantly associated with VC, as shown in Table 4.
Angiographic findings of the study participants.

Values are mean SD or n (%). PCI, percutaneous coronary intervention.
Logistic regression analysis of the predictor of vascular complications.

Adjusted for left radial access, multi-vessel lesion, ABI, junior operator, procedure time, Gensini score and previous radial puncture. Abbreviations as in Tables 2.
Discussion
As a result of its lower occurrence of VC and greater acceptability among patients, an increasing number of medical centers have adopted radial access as the standard approach for performing coronary angiography. 15 While previous studies have identified certain factors, such as ABI and female sex, there remains a dearth of comprehensive risk investigations conducted on a large-scale cohort. 16 Our current study has revealed that several risk factors, including lower ABI, prior radial access at the same artery, and less experienced operators, warrant careful consideration in order to mitigate the occurrence of VC.
The incidence of vascular complications related to radial access varies from 0.5% to 3.5%, depending on the definition of vascular complications, observation period, and research methodologies. 17 Consistent with previous research, the majority of access complications are non-fatal and can be resolved through extended external compression, with surgical intervention rarely required. However, limited studies have explored the predictive factors associated with the occurrence of vascular complications. Patient-related factors, such as age, female gender, and a history of hypertension, have been commonly identified as risk factors for the development of vascular complications. 18
The female gender is associated with a smaller artery caliber and increased difficulty in catheter manipulations due to a heightened risk of artery spasm. In contrast to previous research, our investigation found that being female or having a history of hypertension were not significant risk factors for VC. 19 This discrepancy may be attributed, in part, to the fact that our study employed an age and sex-matched design. Several additional factors, including peripheral arterial atherosclerosis, arterial tortuosity, periprocedure anticoagulant protocols, artery compression techniques, and procedure duration, have been identified as potential contributors to the occurrence and severity of VCs during radial approach procedures. In addition to operator proficiency, our study reveals a significant association between lower ABI values and an increased risk of VC. This finding highlights the importance of considering the possibility that patients with VC may have subclinical PAD that cannot be detected through routine clinical examinations. Given that atherosclerosis is a systemic ailment, it has the potential to impact both peripheral and coronary arteries. The presence of atheroma in the coronary arteries, cerebral arteries, and lower limb arteries serves as the principal catalyst for clinical manifestations and symptoms. 20 Previous studies have indicated that patients with concurrent CAD and PAD who underwent PCI experienced a higher incidence of post-procedural and long-term complications compared to those without PAD at the time. Earlier research has reported that PAD is present in 5% to 40% of patients undergoing PCI. 21
Among catheter laboratories, the ABI has become the gold standard for PAD detection due to its ease of use, reproducibility, and affordability. An abnormal ABI has been linked to atherosclerosis severity and adverse cardiovascular outcomes. 22 In our study, we also found that a lower ABI predicts the occurrence of VC. Operators need to pay close attention during procedure when they have abnormal ABIs. The ABIs on both sides can also guide the preferred choice of radial artery access site. For most operators, the default choice is the right radial artery, as this approach is more familiar and associated with a lower incidence of periprocedural complications. However, when there is a significant discrepancy between the ABIs on both sides, the side with the normal ABI should be chosen as the preferred vascular access site. 23 In addition, the use of ABI may prove advantageous in determining whether femoral or radial access should be employed. 24 In instances where ABI values indicate extreme abnormality, femoral access would be a justifiable option. Furthermore, the selection of proficient operators to conduct procedures on patients categorized as high-risk due to their ABI scores is crucial. Based on the results obtained from our investigation, it is recommended that non-invasive PAD screening be universally implemented as a standard procedure for all patients undergoing elective PCI for CAD. This is particularly crucial for novice operators, as it can enhance their capacity to predict VCs and expedite the learning process for inexperienced practitioners.
In addition to considering the patient's clinical condition and the operator's proficiency in radial access, the periprocedural antithrombotic technique has been recognized as a significant determinant of both the VCs and periprocedural mortality.25,26 The selection of procedural anticoagulation in PCI procedures has an impact on access-site bleeding. Unfractionated heparin has traditionally been the most commonly utilized anticoagulant in interventional procedures. However, a direct thrombin inhibitor known as bivalirudin has recently gained approval for its superior performance compared to unfractionated heparin, as it reduces the overall risk of bleeding events during percutaneous coronary intervention procedures.27,28 However, our research findings indicate that the utilization of bivalirudin did not result in a reduction of vascular puncture site incidents. This outcome can be attributed, in part, to the primary focus of our study on access site complications, which predominantly involved ischemic rather than hemorrhagic complications. Additionally, it is worth noting that a significant proportion of the patients included in our analysis underwent diagnostic procedures that necessitated minimal levels of procedural anticoagulation.
Limitations of the study
There are several noteworthy limitations that should be acknowledged in this study. Firstly, it is important to consider the potential occurrence of selection bias due to the retrospective nature of the study and its confinement to a single center. As an observational study, our research cannot establish causality, only associations. The study population is relatively small and lacks long-term clinical follow-up. Secondly, the analysis did not encompass the likelihood of VC in individuals with either too low (<0.9) or high (>1.4) ABI values, as these extremes represent heterogeneous underlying pathophysiology and clinical significance. Furthermore, the investigation was unable to account for any additional medical history factors that could have influenced the development of peripheral artery disease, such as the use of vascular dilators. However, the robustness of our findings is enhanced by the inclusion of a substantial sample size in this population-based research.
Conclusions
This study identified both patient-specific and procedure-related predictors of VCs in patients undergoing transradial coronary intervention. Patients with a lower ABI exhibited a significantly higher incidence of radial access VC. The routine measurement of ABI prior to coronary diagnostic and/or therapeutic procedures may enable operators to anticipate the risk of VC and opt for a more suitable artery as the access route. In instances where radial access has been previously employed, the repetition of puncture heightens the probability of VC. Consequently, skilled operators may prioritize the contralateral side as the preferred artery route.
Supplemental Material
sj-doc-1-sci-10.1177_00368504241261853 - Supplemental material for The importance of ankel-brachial index in prediction vascular complications in transradial access procedures
Supplemental material, sj-doc-1-sci-10.1177_00368504241261853 for The importance of ankel-brachial index in prediction vascular complications in transradial access procedures by Chuanwei Li, Wen Zhang, Jun Xiao, Chunyu Zeng and Chunmei Xu in Science Progress
Footnotes
Acknowledgements
The authors thank Yingying Jiang for critically revising the manuscript for important intellectual content.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by grants from the National Science Foundation of China (81930008), Natural Science Foundation of Chongqing Municipality (CSTB2023NSCQMSX0348) and Science and Technology Research Program of Chongqing Municipal Education Commission (KJQN202300114), Joint Medical Research Programs of Chongqing Science and Technology Bureau and Health Commission Foundation (2023CCXM002).
Natural Science Foundation of Chongqing Municipality, National Science Foundation of China, Science and Technology Research Program of Chongqing Municipal Education Commission,Joint Medical Research Programs of Chongqing Science and Technology Bureau and Health Commission Foundation (grant number CSTB2023NSCQMSX0348, 81930008, KJQN20230011, 2023CCXM002).
Authors’ contributions
CL and CX performed the data analyses and wrote the manuscript. WZ contributed significantly to analysis and manuscript preparation. JX helped perform the analysis with constructive discussions. CL and CX collected the date. CL contributed to refining the ideas and finalizing this paper. CX contributed to the conception of the study. All authors read and approved the final manuscript.
Data availability statement
The shared data of this study can be obtained by emailing the corresponding authors.
Supplemental material
Supplemental material for this article is available online.
Author biographies
Chuanwei Li received his Bachelor's degree in medicine from Sichuan university in 2008 and Master's degree in medicine from the same school in 2011. Then he got his MD in internal medicine from the Third Military Medical University in Chongqing, China in 2017. He has practiced cardiology for over 13 years. His primary interests are in cardiac arrhythmias, engaging full range of catheter-based ablation therapies.
Wen Zhang is an associate chief physician at the Department of Pulmonary and Critical Care Medicine, Xinqiao Hospital, The Third Military Medical University (Army Medical University) in Chongqing, China. She completed her doctoral degree in Medicine from The Third Military Medical University in 2021, and holds a Master of Medicine and a Bachelor of Medicine in Clinical Medicine from Sichuan University. She research focuses on chronic obstructive pulmonary disease (COPD), and evidence-based medicine. She has been recognized for her contributions to the field with awards such as the National Pulmonary Chronic Disease Management Challenge Champion in 2018.
Jun Xiao is a professor of the Cardiology Department at Chongqing University Affiliated Center Hospital (Chongqing Emergency Medical Center). He has an extensive educational background, having trained at the University of California, San Francisco, and Berlin Heart Center. He specializes in cardiovascular disease research and interventional cardiology, with significant achievements in coronary intervention. His research has been published in numerous prestigious journals. He work also includes several national patents and software copyrights related to medical devices and applications.
Chunyu Zeng is the director of the Cardiovascular Disease Specialty Hospital at Daping Hospital, Third Military Medical University in Chongqing, China. He is also the Director of the Chongqing Cardiovascular Disease Research Institute. A distinguished professor and doctoral supervisor, he has received prestigious awards such as the National Outstanding Youth Science Fund and the Chongqing Outstanding Youth Science Fund. He has made significant contributions to the fields of hypertension and coronary heart disease through both clinical and basic research. He expertise includes coronary intervention and radiofrequency ablation for arrhythmias. He serves on editorial boards of several international journals and is a key member of multiple national and international cardiovascular committees.
Chunmei Xu is a prominent researcher and professor specializing in cardiovascular diseases. With extensive experience in clinical practice and research, she has contributed significantly to the understanding and treatment of heart conditions. She has been involved in several high-impact studies and projects funded by national and regional science foundations. She work has been recognized with numerous awards and honors, highlighting her commitment to advancing cardiovascular health and improving patient outcomes.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.