
Abstract
Kawasaki disease (KD) is an acute systemic vasculitis that preferentially involves coronary arteries in young children, and predominantly affects young children. Cardiovascular lesions are the most severe complications of this disease. Even though giant aneurysms are rare, they can complicate thrombus formation, leading to myocardial ischemia, myocardial infarction, and even cardiac death. Later in life, it can lead to steno-occlusive lesions. Follow-up led to coronary artery stenosis. In this article, we report a case of a pediatric patient with KD who presented with a large thrombus within a giant coronary aneurysm as a consequence of delayed treatment with intravenous immunoglobulin (IVIG) and IVIG resistance, which contributed to the formation of coronary artery lesions. Transthoracic echocardiography is a valuable tool for detecting coronary artery abnormalities; however, computed tomography coronary angiography is valuable for precisely delineating coronary anatomy and complications. It is important to maintain a slightly higher international normalized ratio to decrease the risk of thrombosis in coronary artery aneurysms.
Keywords
Introduction
Kawasaki disease (KD) is an acute systemic vasculitis that affects mainly young children. 1 Cardiovascular lesions are the most important complications of this disease. 1 Giant aneurysms that occur in multiple coronary arteries are rare and are prone to complications, including thrombus formation, and can lead to coronary artery stenosis, thrombus formation, myocardial ischemia, myocardial infarction, and even cardiac death. In this article, we report a case of a child with KD who presented with a large thrombus within a giant coronary aneurysm that was diagnosed via transthoracic echocardiography (TTE) and confirmed via computed tomography coronary angiography (CTCA).
Case presentation
An early 3s male child presented with high-grade fever (39.8 °C), and cough was referred to his respective pediatrician, where he was diagnosed with respiratory infection and treated with antibiotics. However, he was referred to another hospital on the 11th day of illness with high-grade fever (39.1 °C), bilateral bulbar nonexudative conjunctivitis, strawberry tongue, truncal rash, and erythema of the palms and soles. He was diagnosed with KD on the 16th of illness and treated with intravenous immunoglobulin (IVIG; 2 g/kg). His TTE did not reveal any coronary artery abnormalities. Although no coronary artery lesions were detected by TTE, anticoagulation treatment with warfarin was performed with an international normalized ratio (INR) of 1.2 to prevent thrombosis. In addition, aspirin (80 mg × kg−1 × d−1) was added to the treatment protocol.
Despite active treatment, the patient continued to have fever and was referred to our institution in the third week of illness, and laboratory investigations revealed elevated C-reactive protein levels (18.9 mg/dL), elevated erythrocyte sedimentation rates (54 mm/h) and elevated platelet counts (430 × 109/L). Therefore, IVIG resistance was considered, and retreatment with IVIG (2 g/kg) was performed. He subsequently became afebrile, and his inflammation markers improved. No specific changes were found in either his chest X-ray or electrocardiogram. TTE examination performed immediately after admission to our institution revealed that the giant coronary artery aneurysms (CAAs) involved the left coronary artery (LCA), proximal left anterior descending artery (LAD; Figure 1(A)), and proximal right coronary artery (RCA; Figure 1(B)), and there was no thrombosis within the CAAs. The maximal diameters of the RCA, LCA, and LAD were 20 mm (Z-score of 19.17), 5 mm (Z-score of 5.99), and 12 mm (Z-score of 11.51), respectively. No associated regional wall motion abnormalities were found, and cardiac function was normal. The patient was subsequently treated with acetylsalicylic acid (3 mg/kg) and warfarin immediately at an adequate dose to maintain INR values from 2.0 to 3.0. As the patient was asymptomatic, with a normal electrocardiogram, he was managed conservatively and was under regular follow-up. During the follow-up period, the warfarin dosage for the patient was adjusted within an effective therapeutic INR range (2.0–3.0), along with daily administration of 75 mg of aspirin.

Transthoracic echocardiography parasternal short-axis view demonstrating (A) diffuse ectasia of the left main coronary artery (black arrow) and fusiformity of the left anterior descending artery (white arrow); (B) giant coronary aneurysm in the proximal segment of the right coronary artery. Ao: aorta.
Despite adequate antiplatelet and anticoagulation therapy with an effective therapeutic INR range, follow-up TTE at 2 months of fever onset revealed a large fusiform aneurysm in the LCA bifurcation (8.5 mm; Figure 2(A)) and a giant aneurysm at the proximal RCA; both were almost filled with a large thrombus (Figure 2(B)). The maximal Z scores in the proximal RCA and proximal LAD were 22.16 and 5.18, respectively. No global or regional myocardial motion abnormalities were noted in the left ventricle. Owing to the severity of the proximal coronary artery lesions, a CTCA was performed, and the giant aneurysm at the proximal segment of the RCA was delineated with no contrast material filled, suggesting thrombosis formation (Figure 3(A)), as were multiple saccular aneurysms on the distal segment of the LAD (Figure 3(B)). The reasons for not receiving intravenous coronary thrombolysis, intracoronary thrombolysis, or cardiac catheterization were as follows: (1) absence of clinical symptoms, including angina and shortness of breath, in the patient; (2) high echo of the thrombus revealing organization; and (3) limited family financial condition. To prevent further thrombus progression, anticoagulation therapy was intensified with an INR of 2.5–3.5. After a short period of uneventful clinical observation, the patient was further followed on an outpatient basis.

Transthoracic echocardiography parasternal short-axis view showing (A) a giant coronary aneurysm measuring 8.5 mm from the left coronary artery bifurcation (short arrow) and diffuse dilation of the left anterior descending artery (long arrow) and (B) a giant coronary aneurysm measuring 25 × 28 mm from the proximal right coronary artery almost completely filled with thrombus. Ao: aorta; AAO: ascending aorta artery; LCA: left coronary artery; LAD: left anterior descending artery; TH: thrombus; RA: right atrium; LA: left atrium; PA: pulmonary artery.
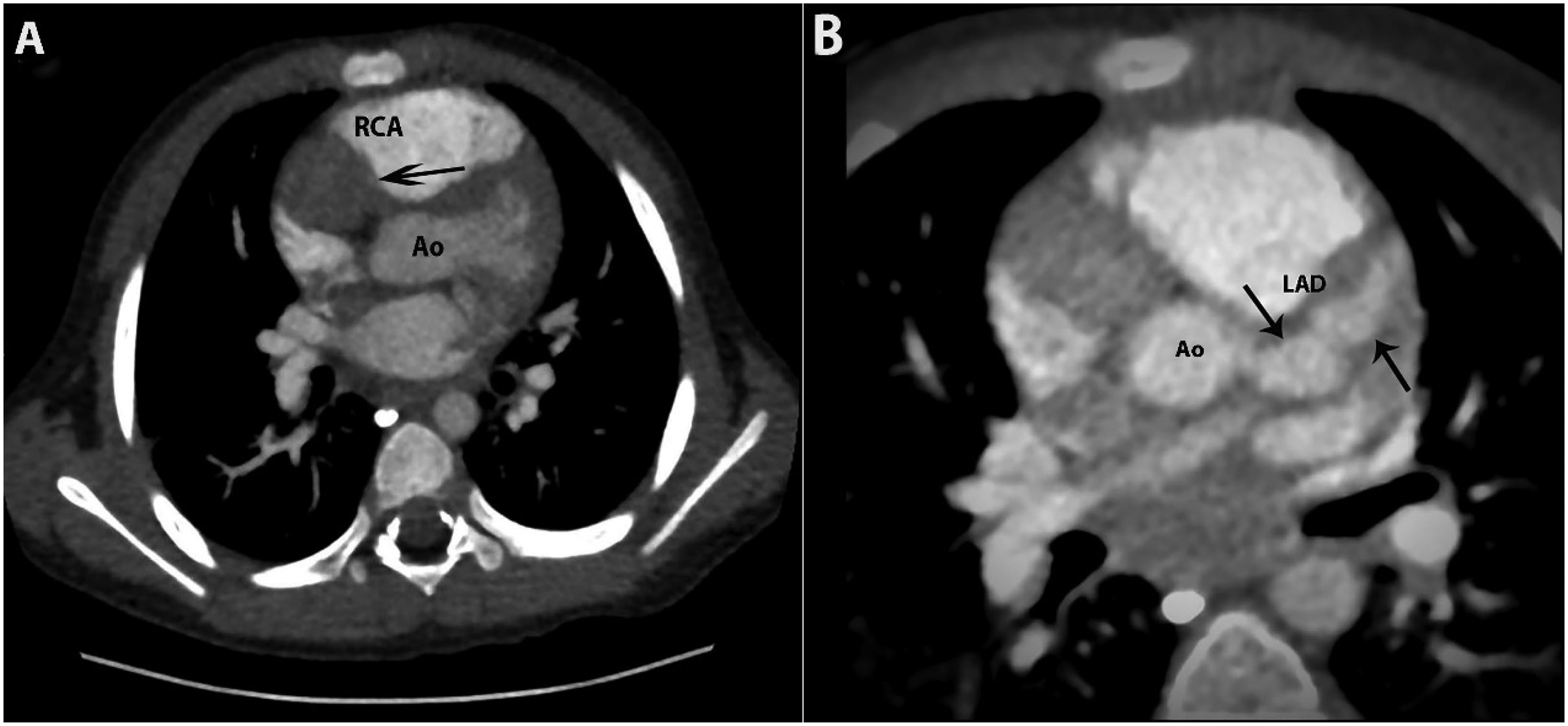
Computed tomography coronary angiography (CTCA) axis imaging demonstrating (A) multiple, saccular aneurysms of the left anterior descending coronary artery (arrow) and (B) giant coronary aneurysms in the proximal segment of the right coronary artery without contrast material filling, indicating thrombus formation (arrow). Ao: aorta; LAD: left anterior descending artery; RCA: right coronary artery.
The reporting of this study conforms to case report guidelines. 2 Written informed consent was obtained from a legally authorized representative for his anonymized information to be published in this article.
Discussion
KD is an acute systematic vasculitis that affects mainly small- and medium-sized arteries. 1 Coronary artery lesions are the most important complications of patients with KD. The occurrence of CAAs can reach 25% in untreated patients, and the most effective therapy is timely treatment with IVIG, which can decrease the percentage of CAAs to 5%.3,4 However, some adequately treated KD patients still develop CAAs. The CAAs with the highest frequency of occurrence are the proximal LAD and proximal RCA, followed by the LCA, left circumflex coronary artery, and distal RCA. 1 Giant CAAs are rare; moreover, 48% of patients with giant CAAs (both a Z score ≥10 and an absolute dimension ≥8 mm) develop thrombosis, stenosis, myocardial infarction, or death. Thus, patients with giant CAAs require life-long follow-up. 1
While TTE is a highly sensitive, specific, and noninvasive tool for proximal coronary artery anomaly evaluation and long-term follow-up, its sensitivity in the diagnosis of distal CAAs remains poor, 4 which leads to underrecognition of distal CAAs in KD patients. In addition, TTE is highly operator-dependent and has interobserver variability. The CTCA is now emerging as an important imaging modality with high sensitivity and specificity, which can allow comprehensive noninvasive evaluation of coronary arteries in KD patients, including luminal changes, intramural changes, and plaque morphology objectively throughout the entire course of coronary arteries at reasonably low radiation doses. 5 In a study conducted by Singhal et al., 6 who compared TTE and CTCA for the evaluation of distal CAAs in patients with KD, the authors reported that distal extension of proximal CAAs was identified in 11 patients and that isolated distal CAAs in the absence of any other coronary involvement in 4 patients who had been completely missed on TTE. Therefore, CTCA should be considered an important complimentary imaging modality in selected children with KD who have CAAs on TTE, which is the reason we chose CTCA for characterizing coronary artery lesions in this patient again after assessment by TTE.
Patients with IVIG resistance and late IVIG treatment are at high risk of developing CAAs. 7 Our case illustrates the largest thrombus within a giant CAA in a child with KD, in the context of a missed diagnosis, and delayed treatment with IVIG and IVIG resistance.
A unique finding of our study is that the child showed progressive clot formation despite repeatedly receiving adequate anticoagulation therapy. Treatment failure with clopidogrel has been reported in the adult population because of reduced pharmacological effects.8,9 However, the lower pharmacological effect of clopidogrel cannot explain the progressive nature of the clotting in our patient. Even after optimal dual antiplatelet therapy with platelet aggregometry and high-intensity anticoagulation, the thrombus progressed. Therefore, our case demonstrated that even adequate anticoagulant therapy may be insufficient for the treatment of acute coronary syndrome in the case of impending thrombotic occlusion of giant coronary aneurysms in KD patients, which can most likely be attributed to decreased blood flow and endothelial dysfunction. Percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) should be considered when such situations are encountered. However, the parents of this child gave up PCI and CABG therapy due to family financial conditions.
Conclusion
Our case demonstrates that anticoagulation may be insufficient for the treatment of acute coronary syndrome in the case of impending thrombotic occlusion of giant coronary aneurysms in KD patients and that decreased blood flow and endothelial dysfunction of the CAA may contribute to ongoing thrombus formation. It is important to maintain a slightly higher INR to decrease the risk of thrombosis in CAA patients. Although TTE can provide information about the anatomy, size, and position of aneurysms in the proximal segments along with thrombosis, the CTCA is the way forward for the precise evaluation of coronary abnormalities and complications throughout the entire course of coronary arteries.
Footnotes
Acknowledgments
I thank the anonymous reviewers, who made significant and appreciated contributions to the final article.
Author contributions
Both Nan Wang and Haiyong Wang contributed to data gathering involved in drafting the manuscript. Nan Wang drafted the initial manuscript. Haiyong Wang provided input and review of the manuscript. All two authors approve of the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethics approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The authors obtained written informed consent from a legally authorized representative(s) for the publication of the case information and any images.