
Abstract
Keywords
Introduction
Polyvascular disease (polyVD) is defined as atherosclerotic lesions in at least two arterial beds such as coronary artery, carotid artery, and lower extremity artery. 1 Recently, patients with polyVD have been categorized as “very high-risk,” and polyVD is gaining extensive attention. 2 Studies have been conducted on the prevalence of polyVD in various populations. Most recently, Pan and colleagues 3 reported the prevalence and vascular distribution of multiterritorial atherosclerotic plaque and stenosis in an old community-dwelling population.
Cardiovascular disease (CVD) has been correlated with systemic atherosclerotic vascular disease which raised the interest of screening polyVD in this population. 4 The prognosis of CVD patients with multi arterial beds involvement is significantly worse than those without polyVD.2,5,6 Meizels et al. 7 found that acute myocardial infarction (AMI) patients with PolyVD represented a significantly higher in-hospital mortality. Similarly, Arai and colleagues 8 reviewed 3411 AMI patients and reported that polyVD was significantly associated with 1-year all-cause death. Recently, Bansal and colleagues 9 reviewed 443 thousand patients with severe aortic stenosis undergoing transcatheter aortic valve replacement (TAVR) and found that polyVD is associated with worse outcomes, and the risk is highest in patients with three vascular beds involvement.
Carotid and lower extremity arteries are frequently used to implicate systemic vascular atherosclerosis involvement.1,10 In previous studies, magnetic resonance imaging (MRI) and ankle-brachial index (ABI) were frequently used to evaluate carotid artery disease and lower extremity artery disease, respectively.3,11 However, the application of MRI in carotid artery screening is limited in daily clinical use due to its time-consuming feature and expensiveness. 12 When detecting lower extremity artery disease, ABI could be falsely high in the presence of arterial wall calcification, a condition often observed in patients with severe cardiovascular disease. 13 As a convenient, cheap, and time-saving method, ultrasound makes it possible to reveal peripheral artery atherosclerotic lesions directly and accurately.14,15 Few studies evaluated polyVD using the method of ultrasound in CABG patients. Our previous study 16 is the first known to report the association of lipoprotein(a) with lower extremity artery disease diagnosed by ultrasound in a CABG population.
In this study, our aims include (1) to investigate the prevalence of polyVD, (2) to investigate the prevalence of plaque and arterial stenosis in different vascular territories, and (3) to find the association of polyVD with in-hospital all-cause death in a CABG population.
Methods
Patients
In this retrospective cross-sectional study, we reviewed 1500 consecutive patients undergoing CABG in the Department of Cardiology at Beijing Anzhen Hospital between 2018.1 and 2020.1. After excluding patients with incomplete or missing data, 1344 patients were finally included. All patients had established severe coronary artery disease (CAD). The patients were divided into groups G1, G2, and G3 according to the number of arterial beds involvement: G1 included patients with only CAD; G2 included patients with CAD and one peripheral arterial bed (either carotid, vertebrate, or lower extremity artery) involvement; G3 included patients with CAD and two or three peripheral arterial beds involvement. Patients ≥65 years were defined as the elderly group, and patients <65 years were defined as the young group. The flow chart of the study is shown in Figure 1.

Flow chart of the study.
Baseline characteristics including age, sex, family history of CAD, smoking history, hypertension (HTN) history, and diabetes mellitus (DM) history were collected from hospital records. Venous blood samples were obtained from fasting patients early in the morning. Beckman AU5400 (US) and Cobas8000 c701 (GER) automatic biochemical analyzers were used to measure novel and traditional lipid parameters and biochemical indicators, including small dense low-density lipoprotein (sdLDL-C), Lp(a), total cholesterol (TCHO), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG). The Sysmex XE-2100 was used to determine complete blood counts. The measurements were all accomplished following the manufacturer's instructions.
Triglycerides and glucose (TyG) index was calculated as ln [TG (mg/dl) × fasting plasma glucose (mg/dL)/2], 17 and TyG-BMI was calculated as TyG×BMI (kg/m2). 18 CKD was defined as having a history of renal failure or an admission estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2 according to modification of diet in renal disease (MDRD) formula. 19 In-hospital all-cause death was chosen as the main adverse outcome and was defined as death from any cause during the period of hospitalization.
Each patients received preoperative peripheral vascular ultrasound examination (carotid, vertebrate and lower extremity peripheral arteries). Carotid and vertebral artery examination included extracranial segments of carotid artery (common carotid artery and internal carotid artery) and extracranial segments of vertebral artery. Lower extremity artery examination included femoral (common femoral artery and superficial femoral artery), popliteal, posterior tibia, and anterior tibia arteries. All images were acquired with Philips (Bothell, WA, USA), GE (Waukesha, Wisconsin, USA) or Hitachi (Tokyo, Japan) ultrasound imaging system by certified experienced ultrasound clinicians. Atherosclerotic plaque is defined as the presence of focal wall thickening that is at least 50% greater than that of the surrounding artery wall. 14 Carotid artery stenosis (CAS) was defined as ≥50% diameter stenosis of internal or common carotid artery. 20 Vertebrate artery stenosis (VAS) was defined as ≥50% diameter stenosis according to local guideline. Lower extremity artery disease (LEAD) is defined as ≥50% diameter stenosis of artery segments from femoral artery to tibial artery.15,21 For each artery bed ≥50–69% diameter stenosis was defined as moderate stenosis, and ≥70% diameter stenosis (includes occlusion) was defined as severe stenosis. 9
The reporting of this study conforms to STROBE guidelines. 22
Statistical analysis
Continuous variables were assessed for normality using Shapiro-Wilk test and were described as mean ± standard deviation if normally distributed. For continuous variables not normally distributed, results were expressed as median with interquartile range. Categorical variables were described as numbers and percentages. For continuous variables, results were compared among the groups using one-way ANOVA followed by LSD post-hoc comparison. For categorical variables, comparisons among the groups were performed using the chi-square test. Receiver operating characteristic (ROC) analysis was performed to analyze the association of polyVD with in-hospital all-cause death in the overall patients and subgroups. Multivariate logistic regression analysis was used to investigate potential risk factors for in-hospital all-cause death in the overall patients and subgroups. Analyses were performed using SPSS 26.0 (SPSS, Chicago, IL, USA); p < .05 was considered statistically significant.
Ethics approval statement
The protocol of this study was performed in accordance with the ethical standards of the 1975 Declaration of Helsinki and its later amendments in 2013. The study was approved by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University as an observational and retrospective study (Date: 1/15/2024; Number: 2024148X). The committee waived the need for informed consent from the patients for the retrospective nature of this study. All patient details have been de-identified.
Results
Baseline characteristics
The overall patients (N = 1344) had a mean age of 61.4 ± 8.5 years and male patients accounted for 76.1%. 700 patients (52.1%) had polyVD: 429 patients (31.9%) had one additional arterial bed involvement and 271 patients (20.2%) had two or three additional arterial beds involvement. Prevalence of polyVD was 53.4% in men and 48.0% in women (Shown in Table 1). Prevalence of polyVD in the elderly patients was higher (65.2%) than that in the young patients (43.0%)(Shown in Table 2).
Baseline characteristics of the patients.
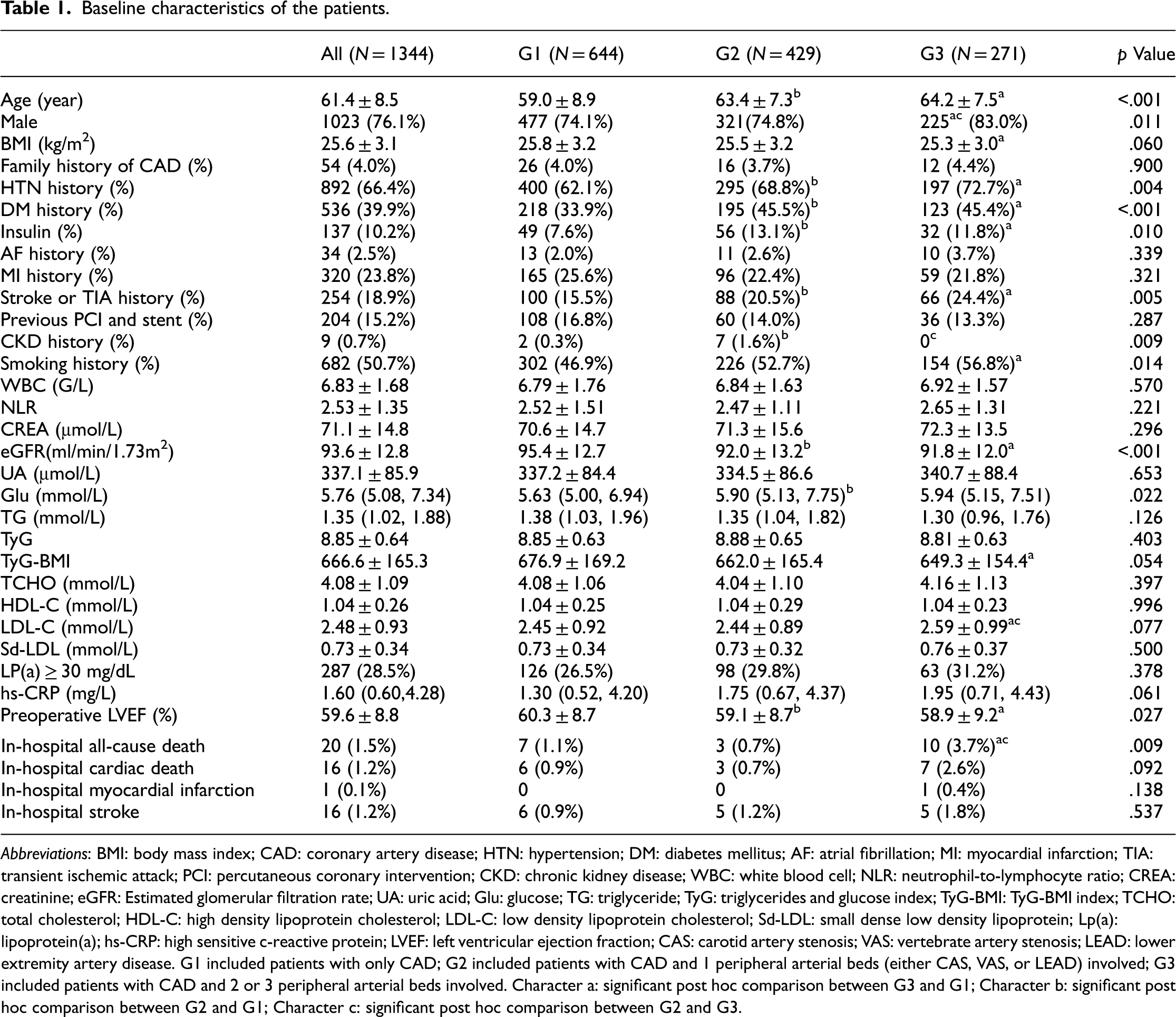
Abbreviations: BMI: body mass index; CAD: coronary artery disease; HTN: hypertension; DM: diabetes mellitus; AF: atrial fibrillation; MI: myocardial infarction; TIA: transient ischemic attack; PCI: percutaneous coronary intervention; CKD: chronic kidney disease; WBC: white blood cell; NLR: neutrophil-to-lymphocyte ratio; CREA: creatinine; eGFR: Estimated glomerular filtration rate; UA: uric acid; Glu: glucose; TG: triglyceride; TyG: triglycerides and glucose index; TyG-BMI: TyG-BMI index; TCHO: total cholesterol; HDL-C: high density lipoprotein cholesterol; LDL-C: low density lipoprotein cholesterol; Sd-LDL: small dense low density lipoprotein; Lp(a): lipoprotein(a); hs-CRP: high sensitive c-reactive protein; LVEF: left ventricular ejection fraction; CAS: carotid artery stenosis; VAS: vertebrate artery stenosis; LEAD: lower extremity artery disease. G1 included patients with only CAD; G2 included patients with CAD and 1 peripheral arterial beds (either CAS, VAS, or LEAD) involved; G3 included patients with CAD and 2 or 3 peripheral arterial beds involved. Character a: significant post hoc comparison between G3 and G1; Character b: significant post hoc comparison between G2 and G1; Character c: significant post hoc comparison between G2 and G3.
Baseline characteristics of the subgroups by age.

Abbreviations: BMI: body mass index; CAD: coronary artery disease; HTN: hypertension; DM: diabetes mellitus; AF: atrial fibrillation; MI: myocardial infarction; TIA: transient ischemic attack; PCI: percutaneous coronary intervention; CKD: chronic kidney disease; WBC: white blood cell; NLR: neutrophil-to-lymphocyte ratio; CREA: creatinine; eGFR: estimated glomerular filtration rate; UA: uric acid; Glu: glucose; TG: triglyceride; TyG: triglycerides and glucose index; TyG-BMI: TyG-BMI index; TCHO: total cholesterol; HDL-C: high density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; Sd-LDL: small dense low-density lipoprotein; Lp(a): lipoprotein(a); hs-CRP: high sensitive c-reactive protein; LVEF: left ventricular ejection fraction; CAS: carotid artery stenosis; VAS: vertebrate artery stenosis; LEAD: lower extremity artery disease. G1 included patients with only CAD; G2 included patients with CAD and 1 peripheral arterial beds (either CAS, VAS, or LEAD) involved; G3 included patients with CAD and 2 or 3 peripheral arterial beds involved. Character a: significant post hoc comparison between G3 and G1; Character b: significant post hoc comparison between G2 and G1; Character c: significant post hoc comparison between G2 and G3.
Patients with polyVD had worse baseline characteristics. Age, prevalence of HTN history, DM history, and smoking history increased with the number of involved arterial beds. Left ventricular ejection fraction (LVEF) and eGFR decreased with the number of involved arterial beds. Uric acid (UA), glucose (Glu), TCHO, LDL-C, sd-LDL, and hs-CRP levels increased with the number of involved arterial beds (with or without significance). The proportion of patients with elevated Lp(a) also had similar trend among the three groups. TyG and TyG-BMI were comparable among the groups (shown in Table 1).
In the elderly patients (≥65 years), the trends of age, smoking history, and blood lipid levels remained, but prevalence of HTN and DM history and eGFR were comparable among the groups. In the young patients (<65 years), trends of most of the cardiovascular risk factors remained. Patients with polyVD had higher prevalence of CAD family history although the difference was not significant (shown in Table 2).
Prevalence of plaque and arterial stenosis in different vascular territories
Prevalence of atherosclerotic plaque: Atherosclerotic plaque was frequently observed in carotid artery (96.9%) and lower extremity artery (87.6%). The prevalence of plaque was only 18.7% in extracranial vertebrate artery. Generally, plaque prevalence was higher in men and the elderly patients (shown in Table 3).
Prevalence of plaque and stenosis of various arterial territories in subgroups by age and sex.

Prevalence of CAS and VAS: 24.4% of the patients had ≥50% CAS and 6.9% had ≥70% CAS. In general, prevalence of CAS of the elderly patients outnumbered that of young patients. However, young women had higher prevalence of CAS compared with young men. Although plaque was not frequently seen in extracranial vertebrate artery, 10.9% of the patients had ≥50% stenosis and 4.8% had ≥70% stenosis (results are shown in Table 3, Figure 2, and Figure 3).

Prevalence of stenosis in various arterial beds: (A) ≥50% stenosis; (B) ≥70% stenosis.

Prevalence of stenosis in various arterial beds in the overall patients, men and women.
Prevalence of LEAD: The population had a high prevalence of stenosis in lower extremity artery territory. Approximately half of the patients (40.8%) had ≥50% lower extremity artery stenosis and 31.9% had ≥70% stenosis. The stenosis was more likely to appear in tibial arteries: prevalence of ≥50% tibial artery stenosis outnumbered that of femoral popliteal artery (37.2% vs 23.1%); the prevalence of ≥70% tibial artery stenosis was far more higher than that of femoral popliteal artery (30.6% vs 4.8%). For both femoral popliteal and tibial territories, men generally had higher prevalence of stenosis (≥50% and ≥70%) than women (shown in Table 3 and Figures 2 and 3).
Association of polyVD with in-hospital all-cause death
In the overall patients, in-hospital all-cause death rate was significantly higher in G3 compared with the other groups (3.7% vs 1.1% and 0.7%, p = .009) (shown in Table 1). All-cause death rates were comparable between patients with only cerebral vascular stenosis (carotid, vertebrate or both) and patients with only lower extremity artery stenosis (0.7% vs 0.7%) (shown in Table S1). In the elderly patients, G3 had the highest in-hospital all-cause death rate (5.1% vs 0.5% and 0.5%, p = .003). ROC analysis showed that AUC of affected artery number was 0.761 (95%CI: 0.601, 0.921; p = .007). In young patients, all-cause death rate in G3 was still the highest among the three groups but without significance (2.2% vs 1.3% and 1.0%, p = .609) (shown in Table 2 and Table S2). Multivariate logistic regression confirmed that polyVD was an independent risk factor for in-hospital all cause death in the overall patients. Patients in G3 (with two or three peripheral arterial beds involvement) had about three times higher risk of in-hospital death compared with G1 (with only coronary artery involvement) [OR, 3.013, 95%CI (1.075, 8.445), p = .036].
Discussion
We are the first known to investigate the prevalence of polyVD using the method of ultrasound in a CABG population. The main findings are as follows: (1) PolyVD is common among CABG patients: 52.1% of the patients had at least one additional arterial bed involvement and 20.2% had two or three additional arterial beds involvement; (2) In-hospital all-cause death rate increased with the number of involved arterial beds, and this trend was more obvious in the elderly (≥65 years) group; (3) Atherosclerotic plaque and stenosis were frequently observed in carotid artery and lower extremity artery.
Numerous studies have reported the high prevalence of polyVD in CAD patients and the results varied due to the heterogeneity of the population and diagnostic method. Syed and colleagues 23 reported that 35% of acute coronary syndrome (ACS) patients had concomitant cerebral vascular disease, LEAD, or both. Song and colleagues 24 reported polyVD was present in nearly 30% of CABG patients. Our data showed that the prevalence of polyVD in CABG patients was 52.1% which was higher than previous result. One of the possible reasons might be that we chose a different method. Ultrasonic device makes it possible to reveal the lesion directly and clearly. Thus, asymptomatic stenosis that had invisible impact on ABI (frequently used by most studies) could be detected by ultrasonic device. Additionally, some study reported sex-based disparity of polyVD prevalence. 21 Our data showed the prevalence of polyVD is similar between men and women in this population. We assume the reason might be that most female patients in our study were in a postmenopausal status.
Atherosclerosis is a systemic disease and involvement of one arterial territory indicates involvement of other arterial territories. 25 The presence of CAD often coexists with atherosclerotic lesions in other arterial beds.1,26,27 Our result confirmed the high prevalence of plaque and stenosis in different artery territories in CABG patients (with established CAD) and the ultrasound-based result provided supplementary information to this field. Additionally, previous study proposed the distribution disparity of polyVD in various populations. 3 Our data showed that LEAD was more frequently observed, and tibial lesions contributed greatly to the prevalence of LEAD. As we mentioned before, the application of ultrasound-based method made it possible to reveal stenosis which maybe neglected by ABI examination. Although the importance of preoperative examination of carotid artery has been proposed, 28 lower extremity artery examination is not a routine according to the guidelines of CABG which should not be underestimated according to our result.
Correlation between polyVD and increased risk of adverse outcomes among CAD patients has been well established.29,30 In our data, all-cause death rate was 1.1% in patients with only CAD and 3.7% in patients with two or three additional arterial beds involvement. Results from both ROC analysis and multivariate logistic regression analysis confirmed the significant correlation between number of affected vascular beds and all-cause death and this correlation was more obvious in the elderly patients. Our result was consistent with previous researchers8,31,32 who proposed the number of arterial beds affected might be a potential risk factor for adverse outcome. Additionally, Weissler et al. 33 reported the difference of adverse outcomes in different polyVD phenotypes. They found patients with CAD and LEAD had the worst outcome. However, we found all-cause death rates of patients with CAS/VAS and patients with LEAD were of no significant difference.
There are possible explanations for the association of polyVD with adverse outcomes. First, patients with polyVD often have a greater burden of cardiovascular risk factors including smoking, HTN history, DM history and high level of various biomarkers.11,34–38 In our study, we also found patients with two or three vascular territories involvement had higher prevalence of HTN and DM history. Song and colleagues 24 proposed that high Lp(a) was independently associated with polyvascular disease in CABG patients. Tmoyan and colleagues 39 included 1288 healthy subjects and proposed Lp(a), hs-CRP, circulating immune complexes, and neutrophil-to-lymphocyte ratio (NLR) were associated with the stenotic atherosclerosis of different vascular beds. We also found various biomarkers including UA, LDL-C, sd-LDL, hs-CRP levels and proportion of patients with elevated Lp(a) increased with the number of involved arterial beds (with or without significance). Additionally, it has been reported that polyVD patients had prominent microvascular endothelial dysfunction which may be an essential characteristic except the already present systemic atherosclerosis. Thus, the existence of peripheral microvascular endothelial dysfunction might contribute to the poor outcomes of polyVD patients. 35
Our study has several limitations. First, this is an observational study and inherent limitations could not be avoided. In addition, we did not evaluate long-term adverse outcome and future study is needed; Secondly, the impact of medication history on the prevalence of poyVD and adverse outcomes was not included, but we assume this would not influence the final result of the study; Third, in-hospital all-cause death was around 1% in our data. Although this is consistent with previous studies, the low incidence of death rate may have influenced the power. However, the focus of our study was to report the prevalence of polyVD in a certain population; The next limitation was that we only included extracranial segments of carotid and vertebrate artery for analysis. Thus, the prevalence of carotid and vertebrate artery atherosclerosis in our data may be underestimated. However, we provided sufficient information and confirmed the association of polyVD and adverse outcome. The fifth limitation was that in our data most patients were male. Although in CABG patients male always outnumbered female, this may have introduced bias.
Conclusion
In conclusion, we reported a high prevalence of polyVD assessed by ultrasound in a CABG population and atherosclerotic plaque and stenosis were frequently observed in carotid artery and lower extremity artery. We found in-hospital all-cause death increased with the number of arterial beds involvement and this trend was more obvious in the elderly patients. For preoperative evaluation of CABG patients, physicians always pay attention to the severity of coronary artery stenosis as well as carotid artery stenosis. Our study may have provided additive information and proposed the necessity of examining various arterial territories preoperatively in this population.
Supplemental Material
sj-docx-1-sci-10.1177_00368504241297206 - Supplemental material for Ultrasound-based prevalence of polyvascular disease and its association with adverse outcome in patients undergoing coronary artery bypass grafting
Supplemental material, sj-docx-1-sci-10.1177_00368504241297206 for Ultrasound-based prevalence of polyvascular disease and its association with adverse outcome in patients undergoing coronary artery bypass grafting by Junyi Gao and Yi Cheng in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504241297206 - Supplemental material for Ultrasound-based prevalence of polyvascular disease and its association with adverse outcome in patients undergoing coronary artery bypass grafting
Supplemental material, sj-docx-2-sci-10.1177_00368504241297206 for Ultrasound-based prevalence of polyvascular disease and its association with adverse outcome in patients undergoing coronary artery bypass grafting by Junyi Gao and Yi Cheng in Science Progress
Footnotes
Authors' contributions
Junyi Gao: conceptualization, formal analysis, methodology, writing-original draft. Yi Cheng: data curation, formal analysis, writing-review and editing.
Data availability statement
The data of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.