
Abstract
Objective
Percutaneous vertebroplasty (PVP) is a primary treatment for osteoporotic vertebral compression fractures (OVCF). Historically, surgeons preferred a bilateral approach for PVP; however, this approach may impose greater financial strain on patients. This retrospective study examines the efficacy of the unilateral approach compared to the bilateral approach.
Methods
A total of193 patients were categorized into Group A (unilaterally extrapedicular approach) and Group B (bilateral approach) based on the operative method. Efficacy was evaluated using perioperative indicators, follow-up results, and imaging evaluation results.
Results
Out of the 193 patients involved, 169 were eligible for analysis. All patients completed follow-up visits lasting 49–70 months. Compared to Group B, Group A exhibited significantly shorter operation time, puncture duration, amount of bone cement injected, and number of X-ray fluoroscopies (P < 0.05). While initial pain reduction, as measured by the visual analog scale and Oswestry Disability Index scores, was lower in Group A, the difference between the groups narrowed by the final follow-up. At the final imaging follow-up, no statistically significant differences were observed between the two groups regarding the relative height of the injured vertebral bodies and local Cobb angle measurements.
Conclusions
This technique holds the potential for accelerated patient rehabilitation and reduced hospitalization expenses, presenting a promising treatment option for OVCF patients.
Introduction
Osteoporosis, a metabolic bone disorder, is characterized by reduced bone mass, deteriorated bone tissue quality, and abnormal bone metabolism. This condition frequently leads to fractures, particularly of the hip, spine, and wrist, with vertebral fractures being notably prevalent. 1
Historically, osteoporotic vertebral compression fracture (OVCF) was treated conservatively with bed rest, analgesics, and osteoporosis medications. However, prolonged bed rest could result in complications such as pressure ulcers, pulmonary infections, and urinary tract infections.2,3 In cases of multiple thoracic fractures, the consequent loss of vertebral height causes severe kyphosis, impacting lung capacity and significantly diminishing quality of life. In instances of multiple thoracic fractures, the resultant reduction in vertebral height leads to severe kyphosis, which can compromise lung capacity and markedly reduce the quality of life.
The first vertebroplasty was conducted in 1984, and a pivotal advancement occurred in 1987 when Galibert et al.. 4 reported successful bone cement injection for vertebral hemangioma. Subsequently, in 1990, Galibert introduced vertebroplasty for OVCF, which demonstrated pain relief, improved quality of life, and reduced mortality, and respiratory failure risk in elderly patients.5,6 The following introduction of kyphoplasty in 2001 by Garfin et al. exhibited rapid pain management, better cement leakage control, and partial restoration of vertebral height.7,8
While Steinmann et al. 9 found no significant difference in stiffness and strength between unilateral and bilateral percutaneous kyphoplasties (PKP), PKP has become a standard surgical treatment for OVCF.10,11 Traditionally, retrobulbar kyphoplasty involved bilateral pedicle access for the injection of polymethylmethacrylate bone cement. Recently, unilateral access vertebroplasty has gained increasing popularity due to its shorter operative time, reduced risk of cement leakage, decreased radiation exposure, and lower cost. 12
Percutaneous vertebroplasty (PVP) is now a well-established and efficacious intervention for OVCF, recognized by both orthopedic surgeons and patients.13,14 C-arm navigation technology improves surgical safety and accuracy, yet its high equipment costs impede its broader adoption. Additionally, repeated intraoperative fluoroscopy is time-consuming and increases radiation exposure. Noa Dagan et al. 15 introduced the use of simulated puncture paths based on computed tomography (CT) images for treating vertebral compression fractures, which demonstrated improved puncture safety and success rates. The utilization of imaging data for preoperative needle entry point planning is deemed critical.
Compared to the bilateral transforaminal approach, the unilaterally extrapedicular approach for PVP offers shorter operative times and reduced X-ray fluoroscopy use. Yet, the comparability of surgical outcomes between these approaches is not well established. To address this, the study conducted a retrospective analysis of 163 cases of osteoporotic thoracolumbar compression fractures treated with PVP between January 2017 and December 2018, and the surgical results of unilateral and bilateral arch root puncture approaches were compared. This study has been published as a preprint. 16
Materials and methods
It is a retrospective study. Upon approval from the local ethics committee (Cangzhou Hospital of Integrated Traditional Chinese Medicine and Western Medicine), a retrospective review of medical records was hereby conducted, involving193 patients having undergone PVP at the department. Patient inclusion criteria were (1) preoperative radiographs, CT, and magnetic resonance imaging (MRI) confirming a recent OVCF with complete pedicle and posterior vertebral body wall and (2) the absence of spinal diseases such as inflammation, tuberculosis, or tumors. All eligible patients (163) were grouped according to their admission dates. Patients admitted between January 2017 and December 2017 were assigned to Group B, while those admitted between January 2018 and December 2018 were assigned to Group A. The study was conducted in strict accordance with the Helsinki Declaration of 1975 as revised in 2013. The study de-identified all patient details and followed relevant Equator guidelines. 17
Surgical procedure
All surgeries were performed at the same institution, Hebei Cangzhou Integrated Traditional Chinese and Western Medicine Hospital, by the same lead surgeon.
Group A: A specific puncture path was planned based on preoperative CT scans and reconstructed images (Figure 1).
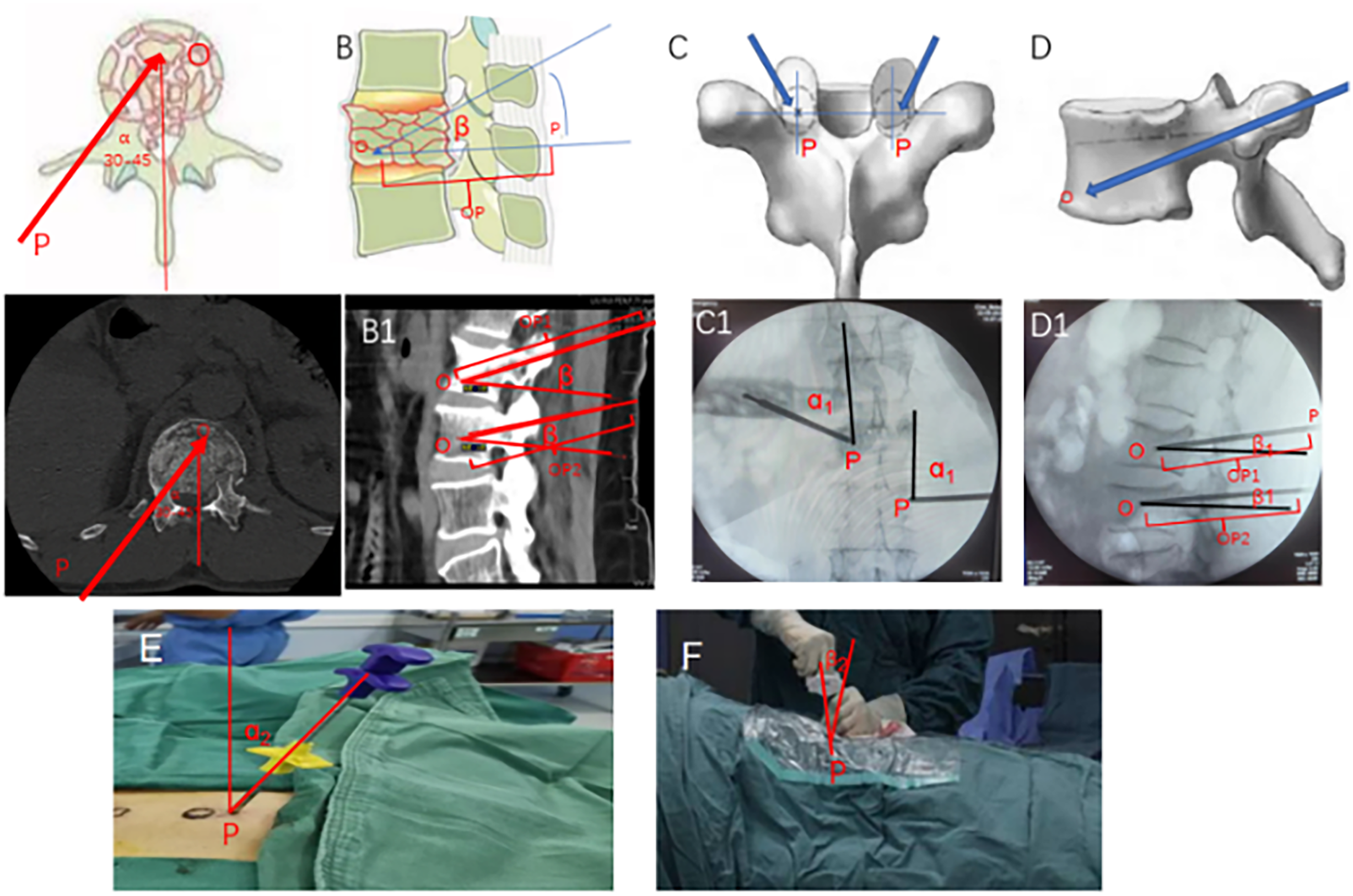
(A–D) Schematic diagram for preoperative planning of puncture location and angle. (A1–B1) Preoperative planned puncture angle and location on computed tomography images. (C1–D1) Intraoperative implementation of the preoperative planning. (E–F) Adjustment of puncture angle during PVP surgery.
The puncture needle was introduced through the incision, positioned at an angle of abduction with 30°‒45°. The needle's trajectory should be adjusted based on fluoroscopic guidance. In the anteroposterior view (Figure 1-A1), the tip of the puncture needle was positioned at the outer edge of the vertebral pedicle, with the lateral fluoroscopic image verifying its alignment along the pedicle midline. The needle was further adjusted according to the fluoroscopic images. In the lateral view, the needle was inserted parallel to the superior endplate (Figure 1-B1 and 1-D1). In the anteroposterior view, the needle tip position was carefully monitored to prevent inadvertent entry into the spinal canal. The puncture needle was advanced through the outer wall of the vertebral pedicle until it reached the junction between the pedicle's outer wall and the vertebral body. In the anteroposterior view, the puncture needle tip aligned with the projection center of the vertebral pedicle, and the lateral image confirmed its position at the posterior edge of the vertebral body. The needle was then advanced approximately 1 cm further, after which the inner core was removed to facilitate bone cement injection. The injected bone cement volume constituted 15–25% of the vertebral volume as determined by CT imaging (4–6 mL).
Point ‘P’ was designated as the skin entry point for the needle (Figure 1-1B, C, and A1) and Point ‘O’ as the target location for bone cement injection (Figure 1-1B, D, A1, and B1), forming the P–O line (Figure 1-A1 and B1). The puncture needle angle (α, β) and P–O line length were determined (Figure 1-C1, D1, E, and F). Intraoperatively, C-arm fluoroscopy was employed to achieve the planned angles (α=α1=α2, β=β1=β2) and needle trajectory (P–O = P–O1 = P–O2). Patients were placed in a prone position, and the affected vertebra was identified with C-arm fluoroscopy. Image optimization was achieved through adjustments to the X-ray tube and patient positioning. Subsequent to standard disinfection and draping, the side of the vertebral body showing greater compression was chosen for needle insertion. Local anesthesia was administered, and 10 points were marked on the left side and 2 on the right side under fluoroscopic guidance. A skin incision was performed, followed by the insertion of a puncture needle. The needle position and direction were fluoroscopically adjusted until it reached the anterior middle third of the vertebral body. A working channel was then inserted, and bone cement was administered under continuous fluoroscopic monitoring. The injected volume ranged 2–4 mL for the lower thoracic spine and 3–6 mL for the lumbar spine. Injection was immediately suspended in the event of cement leakage, resuming only after solidification.
Group B: Patient positioning and preparation mirrored those of Group A. In this cohort, the standard bilateral pedicle approach was selected as the surgical pathway. Bilateral punctures were performed under fluoroscopic guidance, followed by bone cement injection from both pedicles with continuous fluoroscopic oversight. The working channels were extracted post-solidification of the cement.
Clinical and radiographic examination
Perioperative indicators, follow-up results, and imaging findings (relative heights of the injured vertebral bodies and local Cobb angles) were recorded for both groups. Data from the patients were recorded at multiple time points, including preoperatively, at 3 days postoperatively, 1 month postoperatively, 6 months postoperatively, 12 months postoperatively, 3 years postoperatively, and during the final follow-up.
The relative height of the injured vertebral bodies was assessed using preoperative and postoperative lateral X-rays. This measurement was calculated by taking the sum of the height of the anterior edge and the height of the posterior edge of the injured vertebra, divided by two, and then multiplied by the mid-height of the injured vertebra before and after surgery (Figure 2).

Description of vertebral body height and Cobb angle.
Cobb angles were ascertained by employing a protractor to measure the angle between the line segment connecting the curve's initial and terminal points and the horizontal plane, with the vertical lines intersecting the spinal curvature at these points.
Statistical analysis
Measurement data were presented as mean ± standard (x̅
Results
A total of 169 cases fulfilled the specified criteria and were included in the study: 76 with unilaterally extrapedicular approach using puncture route planning-assisted access PVP (Group A) and 93 with bilateral pedicle puncture access PVP (Group B) with a follow-up period exceeding 3 years. Patient characteristics are detailed in Table 1. Both groups successfully completed the puncture procedure without complications, such as nerve, vascular injury, or bone cement allergy, as depicted in Figure 3.

Level of fracture in patient A, B, C, and D is L3, T12, T12, and L1, respectively. (A–B) Two patients in Group A (unilaterally extrapedicular approach); (C–D) Two patients in Group B (bilateral approach). (A1–2, B1–2) Preoperative X-ray showing loss of vertebral body height. (A3, B3) Preoperative magnetic resonance imaging showing vertebral body edema. (A4–5, B4–5) Postoperative X-ray showing bone cement injection via unilateral approach. (C1–2, D1–2) Preoperative X-ray showing loss of vertebral body height. (C3, D3) Preoperative magnetic resonance imaging showing vertebral body edema. (C4–5, D4–5) Postoperative X-ray showing bone cement injection via bilateral approach.
Patients characteristics in two groups.

Abbreviations: BMI: body mass index; Character superscript “a”: Student t test; P < 0.05 demonstrates significance. Character superscript “b”:: Fisher exact test; P < 0.05 demonstrates significance.
Perioperative indicators
Group A had a mean operation time of 29.80 ±
Comparison of perioperative data between two groups of patients.
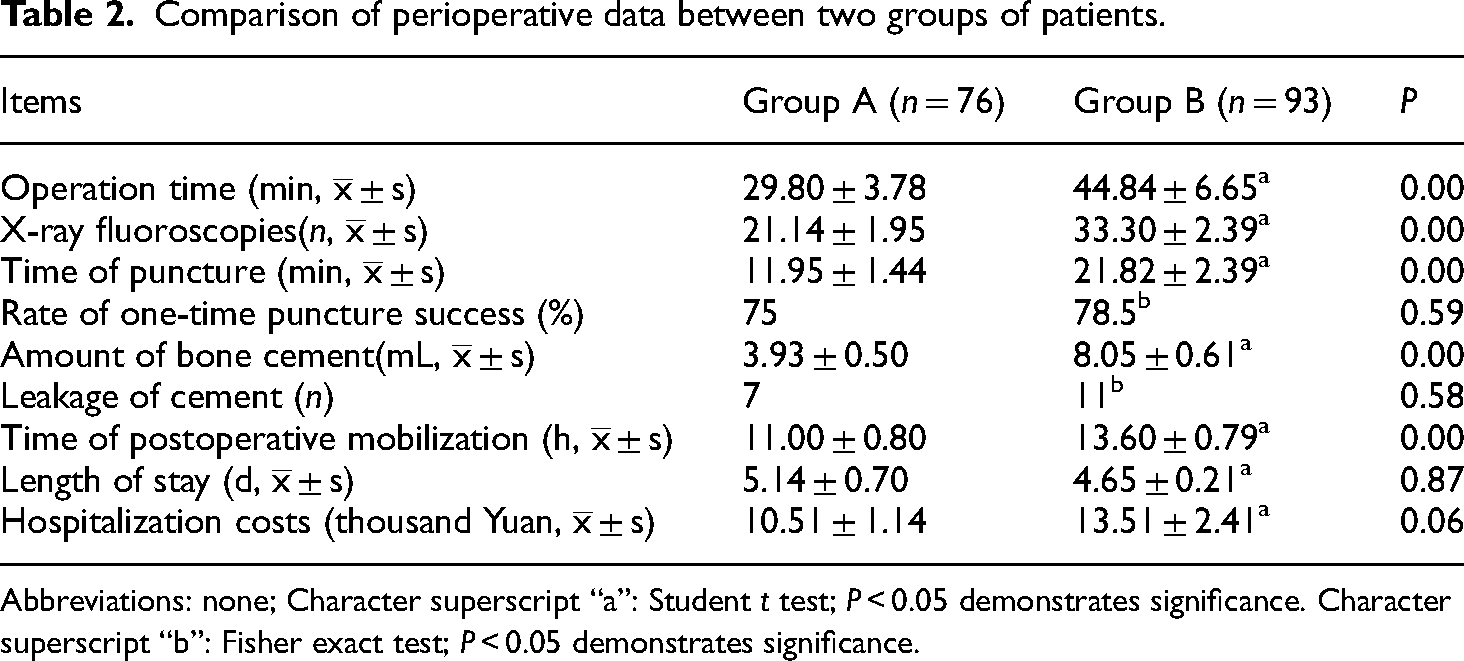
Abbreviations: none; Character superscript “a”: Student t test; P < 0.05 demonstrates significance. Character superscript “b”: Fisher exact test; P < 0.05 demonstrates significance.
Follow-up results
Follow-up time averaged 22.07
Follow-up information and comparison between the two groups of patients.

Abbreviations: VAS: visual analogue scale; ODI: Oswestry disability index; Character superscript “a”: Student t test; P < 0.05 demonstrates significance. Character superscript “b”: Fisher exact test; P < 0.05 demonstrates significance.
Imaging evaluation
There were no statistically significant differences between Groups A and B in terms of relative heights of the injured vertebral bodies (P = 0.60) or postoperative local Cobb angles (P =
Comparison of imaging indicators between two groups of patients.

Abbreviations: none; Character superscript “a”: Student t test; P < .05 demonstrates significance.
Discussion
Herein, no cement leakage was observed in the unilaterally extrapedicular group, consistent with the findings of Tang et al..
11
The unilateral group exhibited shorter operation times, reduced fluoroscopy use, and lower volumes of bone cement compared to the bilateral group, with statistical significance (P <
Traditionally, PVP has employed a bilateral pedicle puncture approach. It has demonstrated no increased risk in new vertebral fractures. 18 However, the unilateral pedicle puncture technique has gained popularity due to shorter operative times and reduced fluoroscopy exposure, minimizing risks to both patient and surgeon.11,12 Researchers have challenged the efficacy of unilateral puncture, positing that it could result in uneven vertebral body height secondary to lateral cement distribution. 13 The bilateral pedicle PVP approach stands out as a standard interventional technique. Liang et al. 8 highlighted the significance of balanced stress distribution on the injured vertebra for pain relief.
No significant difference in clinical efficacy was observed between unilateral and bilateral approaches. However, the unilaterally extrapedicular group exhibited reduced operation times, puncture durations, and hospital stays, alongside lower bone cement volumes, compared to the bilateral group. Initial short-term VAS and Oswestry Disability Index scores were initially lower in the unilateral group, with minimal long-term differences observed between the groups. Patients with even bone cement dispersion reported better postoperative symptom improvement due to increased stability of the vertebral body.16,18–22 The unilateral transpedicular approach is constrained by the anatomical structure of the vertebral pedicle, which limits the ability to increase the abduction angle during the procedure. Consequently, the puncture needle is typically positioned on one side of the vertebral body, resulting in bone cement accumulation on that side and preventing it from reaching the opposite side. 23 This can lead to a stress imbalance across the vertebral body, potentially accelerating the degeneration of the vertebral body and adjacent segments. Meanwhile, the risk of re-fracture in both the affected vertebra and adjacent vertebrae is increased. In contrast, the bilateral transpedicular approach allows for symmetrical cement distribution on both sides, effectively reducing uneven bone cement distribution within the vertebral body and maintaining its balance, which further contributes to improved long-term outcomes for patients.24–27 However, this approach is still subjected to the disadvantage of requiring longer surgical times, increased fluoroscopy, and greater bilateral puncture trauma.
The approach was first proposed by Brugieres et al. 20 in 1990, originally designed for percutaneous biopsy of mid-to-upper thoracic vertebrae under CT guidance. The procedure has developed into a novel access route, known as the paravertebral or pedicle-external route, and is commonly termed the extrapedicular or parapedicular approach. Subsequently, this puncture route has been utilized by scholars for surgical intervention in thoracic vertebral osteoporotic compression fractures, 21 demonstrating favorable clinical outcomes. Ryu et al. 22 further refined this technique, enhancing the accuracy of the needle entry point. In this method, the puncture needle is advanced along the outer wall of the pedicle, passing through the pedicle's base to enter the vertebral body. This approach overcomes the limitations of the pedicle, with the puncture point positioned more laterally, allowing the operator to use a larger caudal inclination angle. As a result, the puncture needle can easily reach the vertebral body's midline or even the contralateral side, ensuring uniform distribution and optimal filling of bone cement. In the traditional approach, the operator typically experiences two sensations of cortical bone penetration: the first occurs when the needle breaks through the costotransverse joint, and the second when it punctures the posterolateral cortical bone of the vertebral body. Upon the initial breakthrough, it is indicative that the needle has entered the joint space between the transverse process and the rib head. At this point, the needle's direction is constrained; any attempt to forcibly adjust its angle poses a risk of spinal cord injury. Therefore, research suggests that shifting the puncture site approximately 1 cm laterally is preferable. This adjustment allows the needle to enter the vertebral body directly through the paravertebral tissues, bypassing the bony constraints of the pedicle and enabling the needle to reach the midline or contralateral side of the vertebra with adjusted angles of inclination or cephalad/caudad tilt. The study's strengths include precise preoperative puncture point localization, optimal puncture angle design, and calculated bone cement dosage, all contributing to reduced procedural duration, improved clinical outcomes, and increased surgical safety.
Effective utilization of preoperative CT image guidance hinges on several key factors: confirmation of a fresh fracture, comprehensive three-dimensional CT imaging of the injured vertebra to assess posterior spinal canal integrity, CT-based bone cement volume calculation, precise puncture point and injection angle planning, and diligent postoperative anti-osteoporosis management.
Compared to the bilateral PVP approach, the unilaterally extrapedicular PVP technique requires more specialized surgical techniques.28–30 Experience involves optimizing preoperative imaging with X-ray, CT, and MRI to determine the optimal lateral pedicle puncture site, carefully inserting the needle along the ventrolateral pedicle edge to achieve maximum abduction angle, ensuring fracture access without spinal canal penetration, maximizing bone cement's thermal and mechanical effects, and injecting 3–4
The unilaterally extrapedicular approach addresses the limitations of vertebral pedicle anatomy. By increasing the abduction angle of the puncture needle, it provides access to the opposite side of the diseased vertebra, facilitating bone cement diffusion into both sides and achieving the benefits of bilateral puncture. This approach may avoid bilateral puncture, thereby significantly shortening the surgical duration and accelerating patient recovery. Additionally, unilateral puncture reduces the number of intraoperative fluoroscopic exposures for both the patient and the operator, which in turn minimizes radiation exposure for both parties. The unilateral PVP via the extrapedicular approach confers benefits to both the surgeon and the patient, with advantages in patient cost-effectiveness, operative duration, blood loss minimization, and reduced fluoroscopy utilization.
To successfully complete clinical promotion and ensure patient safety during surgery, the following points should be emphasized: (1) Prior to surgery, the distance and abduction angle should be measured using imaging data. (2) It should be ensured that the puncture needle reaches the outer wall of the vertebral pedicle and connects to the vertebral body. The upright fluoroscopic image should show the needle tip positioned at the projection center of the vertebral pedicle, while the lateral image should verify its position at the posterior edge of the vertebral body. (3) In the event of bone cement leakage, particularly into the spinal canal, the injection must be stopped immediately. (4) To prevent damage to paravertebral structures, it is important to note that blood vessels and puncture pathways are located in the middle and upper portions of the vertebral body. (5) The surgeon possesses extensive clinical experience. All surgeons participating in this study have practiced for over 5 years and have substantial surgical expertise, as surgical experience may impact both the clinical efficacy and the reliability of the results.
The puncture point of the unilaterally extrapedicular approach may be adjusted outward, and the puncture abduction angle may be increased to ensure that the needle reaches or crosses the midline of the vertebral body. 31 The procedure allows for the adjustment of penetration depth based on the observed bone cement diffusion. This modification facilitates more comprehensive perfusion and distribution of the bone cement, leading to a more uniform distribution that enhances vertebral body stiffness, stabilizes the injured vertebra, and improves spinal stability overall. Consequently, this approach may reduce the incidence of residual low back pain in the short term following surgery.
Postoperative re-fracture is one of the common complications following PVP, posing significant safety risks for patients. By analyzing the risk factors for re-fracture in elderly patients with osteoporotic OVCF after PVP treatment, targeted interventions can be implemented in advance to reduce the risk of postoperative re-fracture and improve long-term prognoses. The results revealed that advanced age, low bone mineral density, a higher number of fractured vertebrae, and cement leakage were independent risk factors for re-fracture in these patients. During PVP, suboptimal bone cement dispersion and uneven stress distribution were identified as critical factors contributing to subsequent adjacent vertebral fractures in the long term.
In this study, no significant difference in the incidence of long-term re-fractures was observed between the two patient groups, which might be attributed to the use of a unilateral approach. This approach achieved better cement dispersion and a lower rate of cement leakage. These findings underscore the importance of precise procedural techniques and risk management to optimize long-term outcomes for elderly patients undergoing PVP.
Conclusions
In conclusion, the extrapedicular unilateral approach offers advantages over the bilateral approach. The unilaterally extrapedicular PVP effectively treats elderly osteoporotic thoracolumbar compression fractures by reducing X-ray exposure, operation time, bone cement volume, and leakage, ultimately improving clinical outcomes and safety. This approach warrants wider clinical application. However, this study may not fully represent the broader population, as it is limited to the specific demographic and clinical characteristics of the patients treated at that institution. The applicability of the findings may be limited to settings with distinct patient demographics or treatment protocols. Furthermore, the small sample size increases the risk of selection bias and reduces the statistical power of the study, potentially leading to inaccurate or unreliable conclusions. To enhance generalizability and minimize bias, future research should endeavor to conduct large-sample, multi-center randomized controlled trials to further validate the effectiveness of this surgical method.
Footnotes
Authors’ contributions
Conceptualization: Xuequan Zhao, Xixi Han, and Chenxu Li; Methodology: Xuequan Zhao; Software: Xixi Han; Formal analysis: Chenxu Li; Investigation: Qinglie Liu; Data curation: Baoguo Han, Tianjiao Zhu, and Yuxue Shi; Original draft preparation: Shuzhang Yao; Review and editing: Yafeng Zhang. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The datasets used and analyzed during the present study are available from the author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the project of Jiangsu Clinical Innovation Centre for Traditional Chinese Medicine (Key Project): Research on Integrated Diagnosis and Treatment System of Traditional Chinese Medicine for Degenerative Spondylolisthesis and Osteoarthropathy (2021040501).
Institutional review board statement
The study was conducted in strict accordance with the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of local Clinical Research Ethics Committees (Ethics Committees of Cangzhou hospital of integrated Traditional Chinese Medicine and Western Medicine NO.2019020; Time:2017.06-2020.06; Location: Cangzhou Hospital of Integrated Traditional Chinese Medicine and Western Medicine, Hebei Province).
Statement on consent
The requirement of obtaining Consent was waived by the Ethics Committees of Cangzhou hospital of integrated Traditional Chinese Medicine and Western Medicine because it was a retrospective study.