
Abstract
Objective
To evaluate the clinical efficacy of the direct posterior approach (DPA) with seagull-shaped plate fixation for treating posterior wall acetabular fractures.
Methods
A retrospective cohort study of 17 patients (8 male, 9 female) with posterior wall acetabular fractures treated with DPA seagull-shaped plate fixation was conducted. Postoperative pelvic X-ray imaging and computed tomography were performed, and the quality of acetabular reduction was evaluated using the Matta score. The Merle d’Aubigné & Bone score, as modified by Matta, was used to assess hip joint function.
Results
The mean ± standard deviation surgical incision length, operating time, and intraoperative blood loss were 9.7 ± 0.6 cm, 48.7 ± 9.1 min, and 235.3 ± 65.6 mL, respectively. According to the Matta score, 11 patients achieved excellent reduction quality, and six had good reduction quality, resulting in a 100% combined excellent or good reduction rate. All patients had good fracture healing, with a healing time of 9.7 ± 1.6 weeks. The modified Merle d'Aubigné & Bone score was 17.0 ± 1.6, with 11, 4, 2, and 0 patients rated as excellent, good, fair, and poor, respectively, yielding an 88.2% excellent or good outcome rate. Postoperative complications included fat liquefaction in one patient and deep vein thrombosis in the lower limbs of two patients, with an overall complication rate of 17.6%.
Conclusions
DPA with seagull-shaped plate fixation provides satisfactory clinical outcomes for posterior wall acetabular fractures, improving patients’ living ability and quality of life.
Keywords
Introduction
Acetabular fractures, a special type of pelvic fracture characterized by a break in the cortical bone of the hip, are caused by various factors, such as a high-energy direct impact or femoral head impact. They are intraarticular fractures and are often accompanied by hip dislocation. Acetabular fractures account for < 2% of all fracture cases; however, they cause substantial damage to the anatomical structure of the hip joint, and are often associated with injuries to nearby organs, blood vessels, and nerves, leading to high mortality and disability rates. 1 Posterior wall acetabular fractures are simple fractures according to the Letournel classification 2 of acetabular fractures; nonetheless, damage often extends to the acetabular joint surfaces. The anatomical location of the injury is relatively deep and is frequently accompanied by surrounding soft tissue damage. 3 Therefore, research on posterior acetabular wall fractures has led to the introduction of several innovative internal fixation treatments.
The Kocher–Langenbeck (K–L) approach is a classic surgical technique used for treating posterior wall acetabular fractures that requires making an incision in the gluteus maximus muscle and releasing its tendon attachment point from the femur. Unfortunately, this approach carries high risks of severe soft tissue dissection, ectopic ossification, and disruption of the blood supply to the femoral head, increasing the likelihood of femoral head necrosis. 4 To address these issues, the improved K–L approach establishes two surgical windows: one between the gluteus medius and piriformis muscles, and one between the short external rotator muscles and the ischial tuberosity. Utilizing these windows avoids the separation of the external rotator and abductor muscles and prevents iatrogenic damage to the femoral head and associated vessels. Nevertheless, this approach is unsuitable for comminuted posterior wall fractures, fractures lasting more than 10 days, and fractures with edge impact. 5 In contrast, the improved Gibson approach reduces the risk of vascular and nerve damage to the gluteus maximus, and minimizes the need for trochanteric osteotomy, making it applicable in nearly all cases where the K–L approach would be used. 6
The direct posterior approach (DPA) was first proposed and used by Professor Shi Cai Fan. 7 This approach involves making a surgical incision from the midpoint between the posterior superior iliac spine and the posterior edge of the apex of the greater trochanter, extending to the greater trochanter of the femur, entering through the gluteus medius-piriformis gap without detaching the gluteus medius or external rotator muscles. It directly exposes the entire posterior wall of the acetabulum, part of the hip joint capsule, and much of the posterior column of the acetabulum. The DPA offers advantages, such as minimal invasiveness, reduced intraoperative bleeding, shorter surgical time, and fewer complications, relative to other approaches. 7
The type of plate and/or screws used during surgical treatment is also an important factor to consider. Due to the strong plasticity of reconstructed steel plates and their flexibility in bending, including lateral bending, and rotation, a combination of reconstructed steel plates and tension screws is often used for the treatment of acetabular posterior wall fractures. However, the toughness of reconstructed steel plates is poor, and they cannot balance the shaping effect while ensuring strong fixation. 8 Spring steel plate treatment for acetabular posterior wall fractures is commonly used for edge fractures of the posterior wall and can have a relatively stable fixation effect. However, simple edge fractures are not common, and very small fractures that cannot be fixed with screws can also be treated conservatively because they rarely damage the stability of the hip joint.9–11 In the seagull-shaped plate treatment, the main body of the plate is a locking hole structure, with cutting and bending functions on the distal end and both sides. It is made of a titanium alloy, which has a similar elastic modulus to bone tissue and good compatibility with bone tissue. 12 Although the seagull-shaped locking steel plate is largely used in ankle fusion surgery, our team has discovered that the distal and bilateral characteristics of the seagull-shaped locking steel plate are very suitable for the treatment of acetabular posterior wall fractures after cutting. Intraoperative cutting and bending can be completed quickly, and the distal end of the seagull-shaped locking steel plate can be attached to the posterior part of the acetabulum according to the anatomical structure of the acetabular posterior wall.
Since 2020, our team has used the DPA with seagull-shaped plate fixation for treating posterior wall acetabular fractures. 7 However, its outcomes and efficacy have not yet been assessed. Herein, we evaluate the quality of fracture reduction, hip joint function, and early clinical efficacy of the DPA with seagull-shaped plate fixation for treating posterior wall acetabular fractures.
Materials and methods
General information
From January 2020 to June 2021, there were 17 patients with posterior wall acetabular fractures at Qinghai University Affiliated Hospital. All 17 patients were selected consecutively, including eight male and nine female patients, with a mean ± standard deviation age of 38.4 ± 8.7 years. The fracture was caused by a car accident in 11 patients, a high-altitude fall in six patients, and this includes one case of hip dislocation. A retrospective cohort study was conducted among these patients. The average waiting time for fractures before surgery is 5.5 days. All patients in this study underwent surgery performed by the same surgical team. This study was approved by the Ethics Committee of Qinghai University Affiliated Hospital (School of Clinical Medicine) on 1 July 2022 (review number: P-SL-2022-040), and all participants signed informed consent forms. This article has removed all patient details. I conducted this study in accordance with the Helsinki Declaration of 1975 as revised in 2024. The reporting of this study conforms to STROBE guidelines. 13
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) imaging diagnosis of posterior wall acetabular fracture based on the Letournel classification; (2) surgical approach adopting the DPA; (3) internal fixation using a seagull-shaped plate; and (4) follow-up period exceeding 1 year.
The exclusion criteria were as follows: (1) non-simple posterior wall acetabular fracture (combined with anterior column, acetabular top, and other fractures); and (2) patients with incomplete follow-up data.
Surgical methods
Preoperative preparation
Preoperative X-ray (plain pelvic film, sacroiliac joint oblique film, and iliac bone oblique film) and three-dimensional computed tomography (CT) examinations of the hip joint were performed. Low-molecular-weight heparin sodium was subcutaneously injected for anticoagulation before surgery. Cefuroxime sodium (1.5 g) was added to 100 mL of physiological saline for intravenous infusion 30 min before surgery to prevent infection, and tranexamic acid 100 mL (100:1.0 g) was intravenously infused 15 min before surgery to reduce intraoperative bleeding.
Surgical procedure
The patient entered the room and was placed in the prone position after induction of general anesthesia. During the operation, the patient maintained a flexed knee and extended hip position to relieve sciatic nerve tension. 14 Routine iodine disinfection was performed twice in the surgical area. The skin was marked with a line connecting the posterior superior iliac spine to the posterior edge of the apex of the greater trochanter of the femur. A straight incision, ∼10 cm long, was made along the midpoint of the line towards the posterior edge of the greater trochanter of the femur.
The skin, subcutaneous, and fascial tissues were cut open, and the gluteus maximus muscle was split along the direction of its fibers to expose the gluteus medius and piriformis muscles. The dissection proceeded through the space between these muscles without detaching the external rotation and abduction muscle groups. Pull the gluteus medius upwards, revealing the posterior portion of the gluteus minimus and the superior gluteal nerve vascular bundle. A bone-membrane stripper was used to adhere closely to the bone and peel off the periosteum, exposing the entire posterior wall of the acetabulum. During exposure, care was taken to protect the superior gluteal nerve and vascular bundle. After separating the gluteus maximus muscle and pulling it apart to both sides, exposing the sciatic nerve first, and performing subsequent operations under direct visualization and protection of the sciatic nerve can reduce the risk of sciatic nerve injury.
The fracture block was lifted in the direction of connecting the soft tissue, and the joint cavity was rinsed and cleaned. Larger fracture fragments were reduced, and bone grafting was considered if the fracture fragment was compressed and if the compressed part could be reset to maintain joint surface flatness. After resetting the fractured fragment, it was temporarily fixed with Kirschner wires or top rods.
The proximal locking hole, the farthest nail hole, and the wing parts on both sides of the seagull-shaped plate were cut according to the degree of soft tissue exposure and the structure of the hip socket. The cutting effect is illustrated in Figure 1. The middle section can cover the posterior wall of the acetabular, and 3–4 nail holes were reserved on both sides of the wing plate. Generally, the steel plate was placed along the edge of the back wall of the hip socket. The distal end of the steel plate was close to the outer edge of the posterior wall of the acetabulum, and the proximal end was close to the inner side of the posterior wall. The steel plate was temporarily fixed using a Kirschner wire. After observing fracture reduction under the C-arm and a good internal fixation position, 2–3 ordinary screws were placed along the hip socket direction at the upper end of the steel plate, and 2–3 ordinary screws were placed along the hip socket direction at the lower end of the steel plate. C-arm fluoroscopy showed a good reduction of the fracture, and the positions of the steel plate and screw were in good condition. The hip joint capsule was fixed to the seagull-shaped plate using ETHIBOND 5 sutures. After rinsing, the wounds were soaked in tranexamic acid for 1 min. A drainage tube was then inserted, and the negative pressure ball was set to a positive pressure state. The fascia, subcutaneous tissue, and skin were sequentially sutured to complete the surgery.
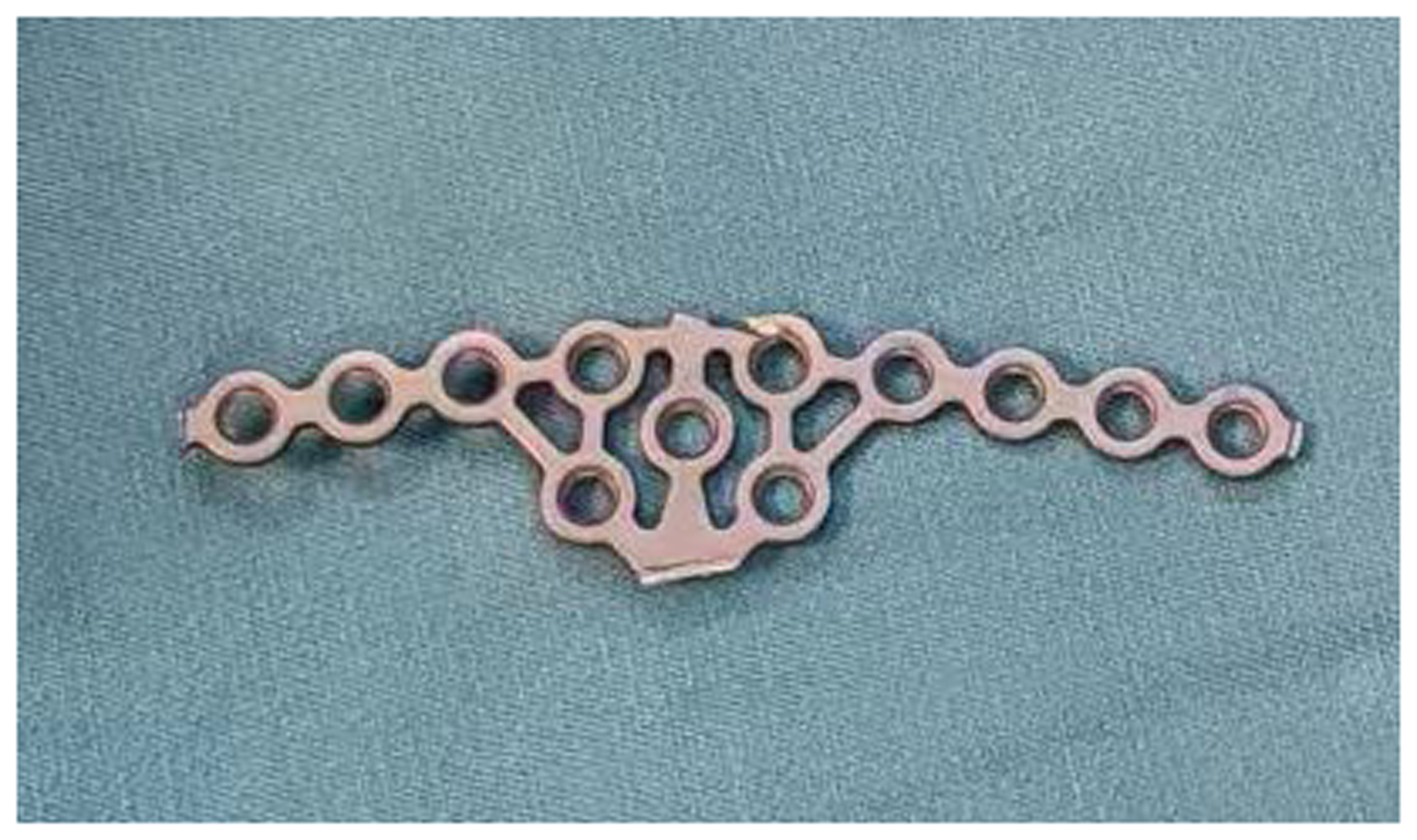
Photograph of the seagull-shaped plate after cutting. The middle section can cover the posterior wall of the acetabular, and the side wings are nail holes.
Postoperative treatment
Following surgery, the patient was placed in the supine position and received an intravenous infusion of tranexamic acid 100 mL (100:1.0 g). Once transferred to the ward, the negative pressure ball was activated 6 h after surgery, while blood flow and sensation in the distal end of the affected limb were monitored. Cefuroxime sodium (1.5 g) was diluted in 100 mL of physiological saline and intravenously infused twice within 8 h of surgery.
On the second day after surgery, X-ray images (pelvic plain film, sacroiliac joint closed-foramen oblique film, and iliac bone oblique film) and a three-dimensional CT scan of the hip joint were obtained to assess the fixation effect. Starting from this day, low-molecular-weight heparin was administered for anticoagulant therapy, provided there was no substantial bleeding from the surgical site. The patients were advised to perform ankle flexion and extension exercises to prevent deep vein thrombosis in the lower limbs.
Active and passive hip joint exercises also began on the second day. For pain management, intramuscular Dezocine (10 mg) injections were administered twice daily (morning and evening) for 2–7 days after surgery. After discharge, low-molecular-weight heparin anticoagulation was discontinued, and the patients were prescribed enteric-coated aspirin tablets (100 g every 12 h orally) until they could walk. Lower limb deep vein ultrasounds were conducted, and the medication was stopped if there was no thrombus. Patients typically began walking with crutches 2–3 months after surgery.
Efficacy evaluation indicators
According to the Matta scoring criteria, 15 the quality of fracture reduction was evaluated as follows: displacement of <1 mm was considered excellent, 1–3 mm was considered good, and >3 mm was considered poor. This indicator can be evaluated in the postoperative 3D CT examination.
Based on the X-ray images of the patient during follow-up, which showed blurry fractures and callus formation, fracture clinical healing was concluded. If the fracture site is not clearly displayed on the X-ray and it is impossible to determine whether the fracture has healed, a 3D CT scan should be performed.
Using Matta's modified Merle d'Aubigné & Bone scoring system, 16 hip joint function was evaluated as follows: (1) pain—2 points for severe pain and inability to walk; 3 points for moderate-to-severe pain and the ability to walk; 4 points for pain after walking, relieved with rest; 5 points for mild or intermittent pain; and 6 points for no pain; and (2) walking—1 point for inability to walk; 2 points for very limited walking; 3 points for limited walking with a walking aid; 4 points for the need for a cane or crutch for long-distance walking; 5 points for mild limping, not requiring a cane; and 6 points for normal walking.
Activity range scores were assigned based on the percentage of postoperative activity to normal activity, with a score of 1 being <50%, a score of 2 being 50%–60%, a score of 3 being 60%–70%, a score of 4 being 70%–80%, a score of 5 being 80%–95%, and a score of 6 being 95%–100%. The total score was the sum of all three categories above, with an excellent score being 18 points, a good score being 15–17 points, an average score being 13–14 points, and a poor score being <13 points. 17
Results
General results
A total of 17 patients completed follow-up. The mean ± standard deviation surgical incision length, operation time, and intraoperative blood loss was 9.7 ± 0.6 cm, 48.7 ± 9.1 min, and 235.3 ± 65.6 mL, respectively. The average hospitalization for these patients is 13.6 days. One patient experienced incision fat liquefaction after surgery, but the incision healed well after 25 days. All other patients exhibited good incision healing. All patients were followed up for a mean of 16.6 ± 4.1 months. We measured the Acetabular Fracture Index in CT, which is the percentage of remaining to the complete arc length in the posterior wall of the acetabulum. And we found that there were three patients with residual posterior wall between 0% and 25%, 10 patients between 25% and 50%, three patients between 50% % 75%, and one patient between 75% and 1%.
Quality of fracture reduction
All patients in this study underwent X-ray imaging (pelvic plain radiography, iliac oblique radiography, and sacroiliac joint obturator oblique radiography) and hip joint three-dimensional CT examinations after surgery. Based on the Matta score, 11 patients had excellent reduction quality, 6 had good reduction quality, and 0 had poor reduction quality. The combined excellent or good rate was 100%. The determination of the quality of the reduction was performed by a physician blinded to the surgical team.
Fracture healing
All patients in this study had good fracture healing with a mean healing time of 9.7 ± 1.6 weeks. There were no cases of internal fixation failure or fracture displacement. The determination of the fracture healing and displacement was performed by a physician blinded to the surgical team. The surgical team did not participate in the evaluation of fracture healing and displacement.
Hip joint function assessment
Approximately 1 year after surgery, the mean modified Merle d'Aubigné & Bone score was 17.0 ± 1.6, with 11 patients rated as excellent, 4 as good, 2 as average, and 0 as poor. The combined excellent or good rate was 88.2%.
Postoperative complications
None of the patients in this study experienced sciatic nerve injury, superior gluteal nerve vascular bundle injury, incision infection, or any other complications, such as femoral head necrosis or traumatic arthritis, during follow-up. One patient experienced fat liquefaction after surgery, but the incision healed after 25 days. Two patients developed deep vein thrombosis in the lower limbs after surgery. Their anticoagulant treatment was changed from aspirin to oral rivaroxaban, and the thrombi resolved by the 3-month follow-up. The overall incidence of postoperative complications was 17.6%.
Discussion
The most typical injury mechanism of a posterior wall acetabular fracture is direct violence transmitted through the knee joint and femur to the proximal femur in the state of hip and knee flexion, causing bone destruction of the acetabular posterior wall due to the impact of the femoral head on the acetabular posterior wall. In recent decades, the treatment approach for posterior acetabular fractures has shifted from non-surgical to surgical interventions. However, due to the complex anatomical structure, and intersecting nerves and blood vessels of the acetabulum, surgery for posterior acetabular fractures is very challenging.18,19 The traditional K–L approach requires considerable surgical exposure, often resulting in numerous severe complications. 20 Manzoor reported that the recovery rate of patients after K–L surgery was 71.4%, with a 7% incidence of ectopic ossification and a 4.7% incidence of femoral head necrosis.
As mentioned earlier, Professor Shi Cai Fan 7 initially proposed a minimally invasive DPA that involved making a straight incision along the midpoint between the posterior superior iliac spine and the posterior edge of the greater trochanter of the femur. In their report, Huang et al. 7 stated that compared with the K–L approach, the DPA had the following advantages: (1) smaller surgical incision and trauma, less intraoperative bleeding, and shorter surgery time; (2) lower incidence of postoperative ectopic ossification; (3) reduced incidence of ischemic necrosis of the femoral head; (4) no exposure or direct contact with the sciatic nerve, minimizing the incidence of iatrogenic sciatic nerve injury; and (5) preservation of the joint capsule and labrum connected to the posterior wall bone block to protect the stability of the hip joint posterior. After anatomical research and clinical certification of the posterior part of the acetabulum, Huang et al. 7 concluded that DPA is suitable for simple posterior wall acetabular fractures, posterior column fractures, posterior wall fractures combined with posterior column fractures, posterior wall fractures combined with hip dislocation, posterior wall fractures combined with sciatic nerve injury, and fractures around the sciatic foramen involving the superior gluteal nerve and blood vessels.
Despite its benefits, the DPA also has certain shortcomings, such as increased surgical difficulty and potential damage to blood vessels and nerve bundles above the buttocks when the apex of the greater sciatic notch is exposed. In addition, when it is necessary to reduce the fracture of the upper edge of the acetabulum, DPA cannot be well exposed, and surgical dissection and operation may be outside the safe range, which can easily damage the superior gluteal nerve and vascular bundle. Therefore, it is not recommended to use DPA for this type of fracture. Nevertheless, we consider the DPA to be a safe, effective, and minimally invasive option for treating posterior acetabular fractures.
Due to the irregular curved shape of the posterior wall of the acetabulum, the reconstruction of the steel plate requires repeated pre-bending during surgery to achieve good bone surface adhesion, which increases surgical time, blood loss, and patient trauma. If the pre-bending of the reconstructed steel plate is insufficient or excessive, it can easily lead to loss of fracture reduction. The seagull-shaped plate has a unique screw-fixing design, enhancing its fixing strength and plasticity. Li Zhaowei et al. found that the strength and plasticity of the seagull-shaped plate were particularly suited for acetabular fractures requiring both softness and hardness. By modifying the seagull-shaped plate, a steel plate suitable for posterior wall acetabular fractures was obtained in this study (Figure 1). Zhao Bin reported that using the seagull-shaped plate effectively reduced the degree of residual pain after ankle fusion surgery. Yu Aiyu et al. also noted that the titanium alloy promotes bone healing by providing benign stimulation during weight-bearing. We believe that the excellent characteristics of the seagull-shaped plate make it ideal for posterior wall acetabular fractures. Nonetheless, current clinical and biomechanical research on the use of seagull-shaped plates for posterior wall acetabular fractures is limited; the cases included in this study are also limited. Moreover, additional studies are needed to compare the efficacy of different plate types, such as seagull-shaped plates versus reconstruction plates.
This study had certain limitations, including insufficient cases, a short follow-up period, and a lack of biomechanical, three-dimensional finite element research, VAS, satisfaction, work, and sports return. In the future, we will continue to conduct follow-up studies to observe complications and long-term efficacy.
One of the cases in this study is shown in Figure 2.

Photographs and X-ray images from a representative case in which the direct posterior approach with seagull-shaped plate fixation was used to treat a left posterior wall acetabular fracture. (a) Preoperative incision planning for the patient. (b) Intraoperative placement of the seagull-shaped plate. (c) Before closing the incision during surgery, tissues such as the gluteus medius muscle were not cut off. (d) The patient was at the one-year follow-up after surgery. (e–g) Preoperative pelvic plain film, iliac oblique position, and obturator oblique position X-ray images of the patient. (h–j) Postoperative pelvic plain film, iliac oblique position, and obturator oblique position X-ray images of the patient.
Conclusions
The present study showed that surgical reduction for posterior wall acetabular fractures using the DPA and seagull-shaped plate fixation resulted in a 100% excellent or good reduction rate, with 88.2% of patients achieving excellent or good hip joint function, with an incidence of postoperative complications of 17.6%. These results demonstrate that this approach may substantially improve clinical results, especially the living ability and quality of life of patients, and be an effective treatment for posterior wall acetabular fractures.
Footnotes
Abbreviations
Acknowledgements
Thank you for the help provided by Editage in language polishing.
ORCID iDs
Author contributions
Shuaixian Tao, Yurong Zhao, and Jidong Wang are responsible for writing the article, with equal contributions as co-first authors. Shaofeng Xu, Jifa Hou, Baoxin Li, and Qiang Wang are responsible for collecting and analyzing cases, while Rong Ren, Zhonglin Lu, and Zhaowei Li are responsible for reviewing and revising the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.