
Abstract
Background
Schatzker IV-C tibial plateau fractures pose a significant challenge for adequate visualization and reduction of the lateral articular surface through a solitary posteromedial (PM) approach. This study aimed to evaluate the effectiveness of an adjunctive lateral patellar ligament (LPL) approach in enhancing articular exposure, assessed through cadaveric modeling and a clinical case series.
Methods
In a cadaveric study, eight preserved knee specimens were dissected using a combined PM and LPL approach. The exposed articular area was quantitatively measured using calibrated digital imaging and ImageJ software before and after the LPL approach was established. Clinically, a case series of 10 patients with Schatzker IV-C fractures underwent open reduction and internal fixation via the combined approach between October 2021 and December 2023. Outcome measures included intraoperative exposure, 12-month postoperative Knee Society Score (KSS), and complications.
Results
The addition of the LPL approach resulted in a 96% increase in the mean exposed articular area (from 8.4 cm² to 16.5 cm²; p < .001) in the cadaveric specimens. All clinical fractures achieved satisfactory reduction and healing. At the 12-month follow-up, the mean KSS was 85.3 (range: 78–88), with no cases of infection, wound complications, or delayed union observed.
Conclusions
The lateral patellar ligament approach significantly improves the surgical exposure of the lateral tibial plateau in Schatzker IV-C fractures when combined with the standard posteromedial approach. This technique facilitates anatomical reduction and meniscal management, contributing to favorable short-term functional outcomes with a low complication rate. It represents a valuable auxiliary option for these complex fractures, particularly in cases involving lateral meniscal impaction or plateau widening.
Keywords
Introduction
Tibial plateau fracture is a common intra-articular fracture in clinical practice, accounting for about 1% of total adult fractures. 1 According to the location and morphology of the fracture, it is divided into different subtypes, and Schatzker classification is commonly used in clinical practice. Among them, Schatzker IV is often caused by high-energy trauma, accounting for about 10%–30% of all tibial plateau fractures.2,3 It is often accompanied by meniscus and ligament injury, which is difficult to operate, and if not handled properly, it is easy to cause serious complications such as traumatic arthritis.
The injury mechanism of Schatzker IV tibial plateau fracture is axial violence combined with varus and valgus stress, leading to split, collapse, and condyle displacement of the medial plateau, even involving the lateral plateau. In order to predict which type IV tibial plateau fractures are susceptible to soft tissue injury, Wahlquist et al. proposed a classification method for type IV tibial plateau fractures. According to the relationship between the fracture line and the condyle, they were divided into three types: A, B, and C. Type A: the fracture line is located medial to the intercondylar spine; Type B: the fracture line passes through the intercondylar spine; Type C: the fracture line is lateral to the intercondylar spine. 4
At present, the posteromedial approach of the knee joint is often used for the treatment of Schatzker IV tibial plateau fractures, but the exposure range of the simple posteromedial approach is limited. 5 For fractures involving the lateral plateau (Schatzker IV-C), especially those with lateral meniscus impaction, the reduction is often poor due to the limitation of the visual field. It seriously affects the prognosis of patients. The posteromedial and anterolateral approaches are commonly used in the clinical treatment of Schatzker IV-C tibial plateau fractures. However, they cause significant damage to the skin's blood supply, thereby increasing the risk of wound edge necrosis, poor healing, and deep infection. 6 In order to increase the surgical field of view, we designed a lateral patellar ligament approach as an auxiliary window, which can be used to solve the problem of lateral meniscus incarceration and observe the reduction of the lateral plateau under direct vision. The increased field of view of this approach was evaluated by cadaveric studies, and the advantages of this approach were verified by clinical case studies.
Materials and methods
Cadaver dissection
We dissected eight knee joint specimens treated with Thiel solution, which unlike formalin fixation, maintains near-physiological flexibility and structural integrity in all specimens, 7 and the dissection study was conducted at the Department of Anatomy, Anhui Medical University. According to the local ethics committee, ethical approval was not required for anonymous human cadaver studies
Posteromedial approach (PM)
The skin and subcutaneous tissue were incised along the posteromedial arc of the tibia. The proximal end of the incision starts from the level of the posteromedial articular surface, and the distal end of the incision generally extends 8 cm below the line of the anteromedial tibial joint. This can be further extended to the distal end based on the position of the fracture line. Subsequently, blunt dissection is performed between the semitendinosus and the medial head of the gastrocnemius muscle, while ensuring the protection of the medial collateral ligament. The medial articular surface of the tibia is exposed, and the joint capsule is retracted bilaterally using a vascular clamp. Valgus stress is applied, sufficiently large to maximize the visual range of the medial plateau, and the edge of the visual field is marked with a marker (Figure 1(a)).

A posteromedial approach and a lateral patellar ligament approach were established on the knee specimen. (a) Posteromedial approach surgeon's view. (b) Lateral patellar ligament approach surgeon's view.
Lateral patellar ligament approach (LPL)
A longitudinal minimally invasive incision was made parallel to the lateral side of the patellar ligament, with the proximal end starting at the level of the lower pole of the patella and the distal end ending at the level of the tibial tubercle. The skin, subcutaneous tissue and the anterior joint capsule were cut in turn. The distance between the incision and the posteromedial approach incision was more than 7 cm and about 0.5 cm from the lateral side of the patellar ligament. 8 Instead, the tip of the blade was used to carefully incise the anterior joint capsule to prevent the lateral meniscus from being injured by mistake. The patella and patellar ligament were pulled medial with a retractor to expose the articular surface of the lateral tibial plateau to the maximum extent, and the edge of the visual field was marked with a marker (Figure 1(b)).
Data collection
After the exposure field was marked through the posteromedial and lateral patellar ligament approaches, the soft tissue around the proximal tibia was completely dissected, and a steel ruler was placed next to the specimen for digital image calibration. Calibrated digital images of each articular surface of the tibial plateau were taken, and ImageJ software was used to analyze these images to calculate the exposed joint surface area. Then the two-dimensional surface area was calculated from pixels converted to square centimeters by the software using the photographed ruler as the reference standard (Figure 2).

Calibrated digital images were taken of the marked articular surface of the tibial plateau. The blue area indicates the visual field exposed through the posteromedial approach. The red area indicates the visual field exposed through the lateral patellar ligament approach.
Clinical study
General data
From October 2021 to December 2023, a total of 10 patients with Schatzker IV-C tibial plateau in our hospital were enrolled in the study. Inclusion criteria: (1) fracture type was Schatzker IV-C tibial plateau fracture; (2) the knee joint function of the affected limb was normal before injury; (3) patients aged between 18 and 65 years; (4) closed tibial plateau fracture. Exclusion criteria: (1) open fracture; (2) poor lower limb function such as cerebral infarction or hemiplegia; (3) there is serious vascular or nerve damage; (4) there is a history of surgery before the knee. The patients ranged in age from 18 to 65 years old, with an average age of 40.6 years old, including six males and four females, five left knees and five right knees, seven traffic accidents and three fall injuries. Intraoperative exploration revealed lateral meniscus incarceration in the fracture line of the lateral plateau in four patients, among whom two had tears in the posterior angle of the lateral meniscus. Three patients had a simple tear in the posterior angle of the lateral meniscus, one patient presented with an avulsion fracture at the tibial attachment point of the anterior cruciate ligament, and two patients had lateral collateral ligament injury (grade II). More details listed in Table 1. The study was approved by the Ethics Committee of the Third Affiliated Hospital of Anhui Medical University; the ethics approval number for this study is 2021(55), and all patients signed informed consent.
Patient characteristics.
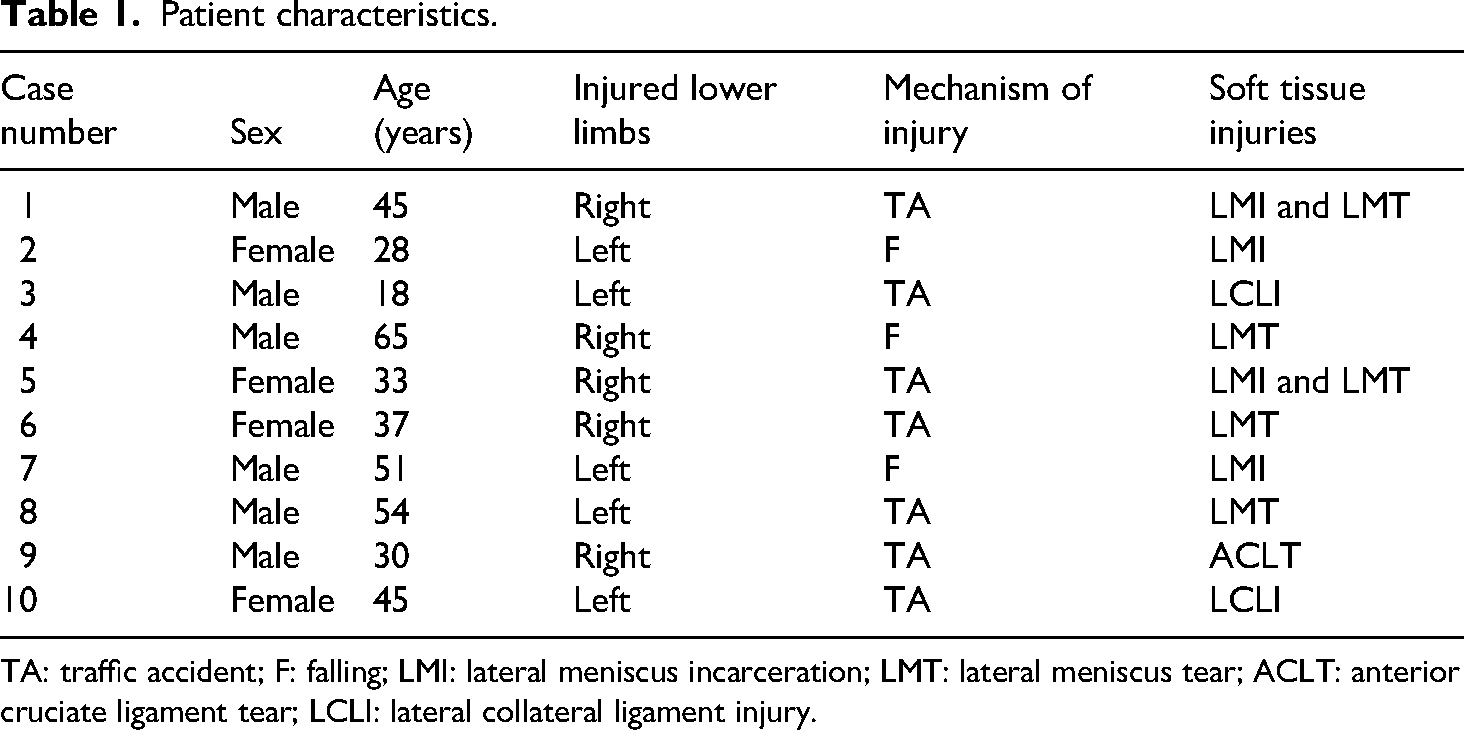
TA: traffic accident; F: falling; LMI: lateral meniscus incarceration; LMT: lateral meniscus tear; ACLT: anterior cruciate ligament tear; LCLI: lateral collateral ligament injury.
Surgical technique
Surgical procedures were typically performed approximately one week after injury, once limb swelling had subsided and the “wrinkle sign” was present on the skin. All operations were performed by surgeons with substantial clinical experience in complex knee trauma, all of whom hold the title of Associate Chief Physician or Chief Physician. After ensuring satisfactory anesthesia, the patient was positioned in the supine posture, and an inflated tourniquet was applied at the root of the thigh on the affected limb. Standard disinfection procedures were performed. A posterior medial arc incision, approximately 8 cm in length, was sequentially made through the skin, subcutaneous tissue, and deep fascia. The incision entered between the semitendinosus and the medial head of the gastrocnemius muscle, exposing the tendon of the pes anserinus. Care was taken to protect the medial collateral ligament, and a trial reduction of the fracture was conducted through the medial approach. In cases where intraoperative fluoroscopy revealed inadequate reduction in the width and height of the tibial plateau, a lateral patellar ligament auxiliary incision, approximately 3 cm in length, was made. The distance between the two incisions should be greater than 7 cm. The length of the incision could be extended upward or downward based on the complexity of the fracture. The lateral patellar ligament auxiliary approach could be adopted, which allowed for clear observation of the conditions of the articular surface of the lateral plateau. If meniscal impaction was found within the fracture line, the incarcerated meniscus could be released through the auxiliary approach. In cases of a tear in the lateral meniscus or an avulsion fracture of the anterior cruciate ligament, repair could be performed through the auxiliary approach. The avulsion fracture of the anterior cruciate ligament was fixed under direct vision, and the reduction of the fracture line of the lateral plateau was observed under direct vision. Upon verification through intraoperative fluoroscopy that the height and width of the tibial plateau were satisfactorily reduced, the fracture block was finally fixed with a medial anatomic locking plate. The fracture end was reinforced with hollow lag screws when necessary (Figure 3).

The figure showed a 45-year-old woman with a Schatzker IV-C tibial plateau fracture caused by a traffic accident (case 10). (a) The radiograph of the patient before the operation. (b) The magnetic resonance image of the patient before the operation. (c) Surface markers of the surgical approach. (d) Intraoperative fluoroscopic images of the patient; it showed that the collapsed lateral plateau fracture fragment cannot be effectively reduced through a simple posteromedial approach. (e) The collapsed lateral plateau fracture fragment was reduced under direct vision by establishing a lateral parapatellar ligament approach. (f) The radiograph of the patient after the operation. P, patella; AL, articular line; LPL, lateral patellar ligament approach; PM, posteromedial approach; TT, tubercle of Tibia; CFF, collapsed fracture fragment.
Postoperative care
The incision dressing was changed on the first day after surgery, and the postoperative anterior-lateral X-rays of the knee joint were reviewed, and the incision drainage tube was pulled out 48–72 hours later. Pay close attention to the healing of the incision within 1 week to prevent the occurrence of adverse complications such as infection and incision cutaneous necrosis, and observe the swelling of the lower extremity within 48 hours to prevent the occurrence of osteofascial compartment syndrome. If the patient has a ligament injury, the knee plaster brace should be fixed after surgery. Passive flexion and extension of the knee joint began on the first day after surgery, rehabilitation of the knee joint flexion and extension function was completed 4–6 weeks after surgery, and weight-bearing activities began to be practiced 10–12 weeks after surgery.
Observation index
The operation time, blood loss, complications, bone healing time, and KSS score at 1 year after the operation were recorded. The KSS score is categorized as follows: 85–100 points as excellent, 70–84 points as good, 60–69 points as medium, and below 60 as poor.9,10 The KSS assessment was not performed in a blinded manner.
Statistical analysis
To ensure objectivity, all statistical analyses were performed by an independent researcher who was blinded to the experimental groups. All statistical analyses were performed using SPSS software (version 25.0). For comparisons between two independent groups or paired samples, parametric Student's t-tests or paired t-tests were applied, respectively, following confirmation of assumptions for normality (Shapiro–Wilk test) and homogeneity of variances (Levene's test). If these assumptions were not met, the non-parametric Mann–Whitney U-test (for independent samples) or the Wilcoxon signed-rank test (for paired samples) was used instead.
Results
Cadaveric study
A total of eight knee specimens were available for study, all of which showed that the surgical field of view of the articular surface of the tibial plateau could be significantly increased by increasing the lateral patellar ligament approach, with an average increase of 96% in the exposed area. The surgical field of view exposed through the simple posteromedial approach was about 8.4 cm2, and that exposed through the combined posteromedial and lateral patellar ligament approach was about 16.5 cm2, and the difference between the two was statistically significant (Table 2). The anterior cruciate ligament, lateral intercondylar spine, and lateral meniscus can be clearly displayed through the lateral patellar ligament approach.
Exposed articular surface area.

PM: posteromedial approach; LPL: lateral parapatellar ligament.
Case series study
The mean operation time was 2.4 hours, the amount of blood loss was 129.5 ml, and the bone healing time was 12.8 weeks. There were no complications such as incision infection and incision necrosis in all patients. Two patients developed temporary saphenous nerve paralysis and recovered completely at 8 and 12 weeks, respectively. All patients were followed up for at least 1 year after surgery, and the average KSS score at 1 year after surgery was 85.3, among which seven patients were evaluated as excellent and three patients as good (Table 3).
General data.

Discussion
We have treated 10 patients with Schatzker IV-C tibial plateau fractures through a posteromedial approach combined with an auxiliary lateral patellar ligament approach with satisfactory clinical results. No incision infection, incision necrosis, delayed fracture healing, or other adverse complications occurred in all patients, and the KSS score was excellent or good at 1 year after operation. This is the first cadaveric study to verify that adding a lateral patellar auxiliary approach can significantly increase the exposed area of the tibial plateau by an average of 96%.
In clinical practice, the posteromedial approach is commonly used to treat Schatzker IV-A and Schatzker IV-B tibial plateau fractures. 5 However, the reduction of Schatzker IV-C fractures by this surgical method often leads to poor reduction or even difficult reduction due to limited exposure space and poor vision.11,12 Schatzker IV-C tibial plateau fractures often involve the posterolateral column of the tibial plateau. 4 Due to its special fracture location and the complex anatomical relationship of the surrounding local area, how to safely achieve the reduction and fixation of the posterolateral region fractures in a limited space has always been a problem faced by trauma orthopedic surgeons.13–15 At present, the common surgical approaches for the treatment of posterolateral column fractures include: anterolateral approach, posterolateral approach, posteromedial approach, proximal fibular osteotomy approach, lateral femoral condyle osteotomy, and Gerdy's tubercle osteotomy approach.16,17
For lateral tibial plateau fractures, the anterolateral approach is the main approach, but the standard anterolateral approach can only expose 1/3 of the articular surface of the lateral plateau, which has great difficulty in exposing the posterolateral fracture fragment, but it can be selected as a combined approach or an auxiliary approach.18,19 The posterolateral approach is the mainstream approach for the treatment of posterolateral tibial plateau fractures. 5 Carlson 20 reported in 2005 that the posterolateral and posteromedial double S-shaped incisions were used for the treatment of posterior column fractures of the tibial plateau, and the posterolateral incision has been followed and modified by later scholars. The advantage is that the exposure of the posterolateral corner is sufficient and direct, which can roughly expose the posterolateral area between the superior tibiofibular joint and the insertion of the posterior cruciate ligament and the space between the small head of the fibula. The disadvantages are as follows: (1) The classic posterolateral approach and the inverted “L” approach require a prone position, which is not easy to achieve for patients with craniocerebral injury, thoracic and abdominal trauma, etc. It increases the risk of infection for patients who need to change position during an operation, and it is difficult to treat the fractures in other quadrants, especially the anterolateral quadrant. (2) The dissection of the posterolateral corner is large, and sometimes it is necessary to dissect part of the popliteal muscle and part of the posterolateral complex. How to maintain the stability of the posterolateral region is a challenge. With the development of sports medicine, the stability of the posterolateral region has been paid more and more attention by scholars, and it is also a hotspot of current research. (3) The shape of posterolateral vessels and nerves is complex and variable, so there is a risk of injury to adjacent vessels and nerves by the posterolateral approach. Moreover, according to years of local anatomy and clinical experience, the scope of distal dissection should be controlled within 5 cm below the articular surface. For the treatment of posterolateral column fractures, in addition to the posterolateral approach, posteromedial approaches can also be used for posterolateral region exposure and fixation, which can expose the posteromedial and posterolateral columns of the knee joint relatively fully and directly. 21 Due to the complex posterior anatomy of the knee joint, there are many branches of blood vessels and nerves, and the risk of injury to blood vessels and nerves and branches is high, which requires high requirements for surgeons. At the same time, different degrees of flexion contracture of the knee joint are also the shortcomings of the posterior median approach. Therefore, the posterior median approach is relatively rare in clinical practice, which is mainly suitable for the exploration of popliteal vessels and nerves. Due to the special anatomical position of the posterolateral region and the congenital occlusion of the proximal fibula, the operation space is narrow and limited, and it is sometimes difficult to achieve effective reduction and fixation of the posterolateral bone fragment by the above non-osteotomy approach. Therefore, in recent years, scholars at home and abroad have proposed to use a variety of osteotomy approaches to treat posterolateral tibial plateau fractures.22–25 At present, the proximal fibular osteotomy approach, lateral femoral condyle osteotomy approach and Gerdy's tubercle osteotomy approach are mainly reported, which aim to increase the exposure of the posterolateral region, but also bring problems of bone healing at the osteotomy site and stability of the posterolateral region.26,27
Combined with the morphological characteristics of Schatzker IV-C tibial plateau fracture and the advantages and disadvantages of common surgical approaches, this study added an auxiliary small incision near the patellar ligament approach on the basis of a simple posteromedial approach, and a small incision near the lateral patellar ligament was used as an observation window for auxiliary reduction and direct articular surface reduction. Schatzker IV tibial plateau fractures involve a large range of articular surface, especially in patients with posterolateral column involvement. It is difficult to directly observe the reduction of the articular surface of the fracture site through a simple posteromedial approach. Previous authors have advocated for combined lateral peripatellar and posteromedial approaches to address the limitations of single approaches, which often provide restricted visualization and inadequate reduction of posteromedial fragments and associated meniscal injuries. 28 Our study extends this existing work by focusing specifically on the Schatzker IV-C subtype , which involves distinct posterolateral column impaction, and by introducing a modified lateral patellar ligament approach. In contrast to the previously described lateral peripatellar route, our approach offers enhanced and direct access to the posterolateral tibial plateau, enabling more effective decompression of the impacted lateral meniscus and facilitating the restoration of plateau width. Furthermore, a key methodological advancement of our study is the incorporation of a cadaveric dissection study, which provides novel anatomical evidence regarding exposure adequacy, safety margins, and technical feasibility that was not available in prior clinical studies alone. The lateral patellar ligament approach can detect and remove the soft tissue of the meniscus in the incarcerated fracture in time, and directly view the articular surface and fracture line, which is beneficial to the reduction of the proximal tibial articular surface, and reduce intraoperative fluoroscopy. For articular surface fractures, the degree of joint function recovery is usually proportional to the accuracy of fracture reduction.29–31 Intra-articular fractures require anatomical reduction, and this approach creates a good condition for the reduction of the articular surface of the fracture. In addition, this approach has less trauma, does not involve important vascular and nerve bundles, and is relatively simple and safe to operate. Through a clinical case series study, we found that increasing the approach did not increase the risk of postoperative incision infection or necrosis, but was conducive to the anatomical reconstruction of the articular surface of the tibial plateau and the recovery of knee joint function after operation.
In the present study, all patients were successfully followed for a minimum of 1 year, demonstrating a mean KSS of 85.3. This outcome is particularly encouraging, with 70% of patients (7/10) achieving an excellent rating and the remaining 30% (3/10) a good rating, according to the KSS criteria. These favorable short-term results indicate that our surgical protocol effectively restores knee function and stability in the initial postoperative period. When contextualized within recent literature, our findings align with the expected trajectory of recovery but also highlight areas for long-term vigilance. The excellent and good outcomes at one year are comparable to those reported in studies utilizing modern internal fixation techniques, suggesting that achieving stable anatomical reduction is a critical factor for early success. 32 However, the work by Biz C et al. serves as a crucial reminder that even with satisfactory initial functional results, the risk of posttraumatic knee osteoarthritis (KOA) development remains a significant long-term concern. 33 Their research underscores that the initial joint injury itself is a primary predictor for KOA, independent of the quality of surgical reduction. Therefore, while our high 1-year KSS scores are promising, they represent only the first chapter in the patient's journey. Consequently, the functional status at one year, as captured in our study and others, should not be misinterpreted as a final endpoint. As emphasized by Belluzzi et al., long-term follow-up is essential to monitor the potential decline in function and the radiographic progression of osteoarthritis over time. 34 Our future research directions will include extending the follow-up period to evaluate these critical long-term outcomes, specifically assessing the incidence of KOA and the durability of the functional results we observed at one year.
In our cadaveric study, we found that there was a great limitation in the field of view of the tibial plateau revealed by using only the posteromedial approach. This approach can only clearly show the structure of the medial platform, but can not effectively show the details of the lateral platform. However, once the lateral patellar approach was introduced, the situation changed markedly. With this assisted approach, we were not only able to clearly visualize the insertion of the anterior cruciate ligament, but also to observe the clear structure of the lateral intercondylar spine and lateral meniscus. This increases our visual field area by a full 96%. This new approach not only provides a wider anatomical view but also makes the surgical operation more precise and controllable. By expanding the surgical field, we can understand the anatomical structure more comprehensively, which provides strong support for surgeons to make more accurate judgments and operate during surgery. In clinical studies, the lateral patellar approach allows surgeons to pry and reduce the collapsed fracture fragment of the lateral plateau under direct vision, thereby restoring the anatomical structure of the articular surface. At the same time, this approach also provides favorable conditions for the surgeon to repair the damage to the soft tissue within the joint. In our case study, tears of the posterior horn of the lateral meniscus were found in five patients. Among them, four cases were successfully repaired by suture via lateral patellar approach, while in the other older patient, the meniscoplasty was performed directly. In addition, we encountered a patient with an avulsion fracture of the tibial insertion of the anterior cruciate ligament, which was successfully reduced under surveillance through a lateral patellar ligament approach and fixed with cannulated screws. This approach provides an effective way for the repair of fractures and intra-articular soft tissue injuries, and greatly improves the success rate of surgery.
However, our study has some potential limitations. First, we did not set a control group and did not conduct comparative analyses with the posteromedial approach alone to assess whether there were statistically significant differences in operative time, intraoperative blood loss, surgical complications, and postoperative knee function. This will be the focus of our future studies to more fully understand the superiority of the new approach. Second, in the cadaver study, the exposed area is obtained by artificial marking, and there are certain measurement errors. We need to further improve the experimental method to reduce these errors and ensure the reliability of the research results. In addition, the clinical sample is relatively small, which may lead to a certain bias in the study results. Therefore, we plan to expand the sample size to verify the validity and scientific validity of the method. Another key limitation is the sole reliance on the Knee Society Score (KSS) for functional assessment. Although the KSS is a widely used and validated tool, it prioritizes clinician-reported metrics and may not fully reflect patients’ subjective experiences—such as quality of life, emotional well-being, or specific daily functional challenges. The incorporation of patient-reported outcome measures (PROMs), such as the Oxford Knee Score (OKS), WOMAC, or SF-36, would allow for a more comprehensive and multidimensional evaluation. We recommend that future studies integrate diverse PROMs to better capture the full spectrum of patient outcomes.
Conclusions
The lateral patellar ligament auxiliary approach appears to be a useful technical adjunct for improving articular surface exposure during the surgical management of Schatzker IV-C tibial plateau fractures. Our preliminary experience suggests that this approach may facilitate reduction and visualization, particularly in cases involving lateral meniscal impaction and restoration of plateau width. While our initial results are promising, further comparative studies with larger sample sizes are needed to definitively establish the advantages of this technique over existing approaches.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank all staff members in the participating departments.
Ethical approval
This study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki and its later amendments or comparable ethical standards. According to the local ethics committee, ethical approval was not required for anonymous human cadaver studies. All procedures involving human participants were approved by the Ethics Committee of The Third Affiliated Hospital of Anhui Medical University.
Consent to participate
In this clinical study, written informed consent was obtained from all patients included.
Consent for publication
Not applicable.
Authors’ contribution
RF and RDN designed and conducted the study and wrote the manuscript. KHW and CNZ collected and analyzed the data. BZT and YLL reviewed and edited the manuscript. All authors read and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant from the Basic and Clinical Collaborative Research Promotion Initiative of the Third Affiliated Hospital of Anhui Medical University (2023sfy017).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions regarding patient data and anonymity, but may be available from the corresponding author upon reasonable request.