
Abstract
Sinonasal inverted papilloma (SNIP) is less malignant and usually occur in the maxillary sinus. However, cases invading the pterygopalatine fossa are extremely rare. In this article, we describe a rare case of a man in his early 60s who presented with left nasal congestion, headache, epistaxis, and facial numbness. The patient underwent a comprehensive treatment primarily based on surgery. Nasal endoscopy showed that the mass had invaded the left infratemporal fossa laterally and was poorly separated from the internal maxillary artery, which increased the complexity and difficulty of the surgery. In addition, the patient had previously undergone nasal cavity surgery, which made the surgery more challenging. In order to reduce the risk of recurrence, we exposed the infratemporal fossa region under nasal endoscopic guidance with a combined labial and gingival incision, and completely removed the tumor base and tumor margins. There were no postoperative complications and no recurrence was observed during the 2-year follow-up period.
Introduction
Sinonasal inverted papilloma (SNIP) is a benign tumor that is less likely to be malignant, with lesions typically occurring in the maxillary sinus and rarely invading the pterygopalatine fossa. The mechanism of malignancy is not clear, and the diagnosis is mainly based on histopathology. 1 A thorough preoperative general examination is required to accurately assess the extent of surgery. The main treatment is complete intraoperative removal of the diseased tissue, which is the most important factor affecting the prognosis. Due to the deep anatomical location of the pterygopalatine fossa and its proximity to important structures such as the orbit and the internal maxillary artery, it is difficult to perform a complete resection of the tumor in this region. In this article, we report a rare case of malignant lesion of SNIP invading the pterygopalatine fossa, and we also review the literature on the mechanism and treatment of malignant lesions of SNIP.
Case report
The patient, a man in his early 60s, was admitted to the hospital with left nasal congestion, and epistaxis for more than 3 months, slight decrease in sense of smell, occasional headache with no clear temporal regularity, and occasional numbness on the left side of the face. The above symptoms persisted and worsened. For further treatment, the patient came to Guangzhou Twelfth People's Hospital and was admitted for detailed examination on July 2022. There was a history of removal of nasal polyps 17 years ago, however, the patient could not specifically describe the situation and lacked pathological information. Physical examination and nasal endoscopy showed a mass protruding from the left middle nasal tract, about 2*2*1.5 cm3 in size, brittle, with a poorly smooth surface, unclear borders, movable, and no signs of redness, swelling, oozing, tenderness, or increased skin temperature, with an S-shaped deviation of the nasal septum (Figure 1(a)). Sinus computed tomography (CT) showed: left maxillary soft tissue mass and sinus wall bone destruction, bilateral inflammation of maxillary sinus, ethmoid sinus, and left frontal sinus (Figure 1(b)). Biopsy pathology showed: malignant transformation of SNIP in the right nasal cavity. To be exact, it's cellular squamous cell carcinoma (SCC) (Figure 2(a)). Magnetic resonance imaging (MRI) with contrast enhancement demonstrated a mass involving the left nasopharyngeal lateral wall, pterygopalatine fossa and maxillary sinus cavity, with destruction of the left skull base bone. The findings suggested a high likelihood of a malignant tumor, and nasopharyngeal cancer cannot be ruled out (Figure 1(c)). Given the large size of the nasal mass and its primary location in the pterygopalatine fossa, the surgery was extremely difficult. There was a significant risk of injury to critical structures such as the pterygopalatine ganglion, infraorbital nerves, and the maxillary artery, which could lead to severe complications including hemorrhage, blindness, and shock. Therefore, we developed a comprehensive treatment plan for the patient and obtained the patient's consent. The patient underwent two cycles of preoperative chemotherapy (paclitaxel and cisplatin). The specific chemotherapy protocol consisted of docetaxel (120 mg) for 1 day, followed by cisplatin administered over three consecutive days at doses of 40 mg each. The patient reported no significant discomfort. Enhanced CT of the sinuses showed that the swelling was smaller than before on 26 July 2022 (Figure 1(d)). Subsequently, the patient underwent resection of the malignant SNIP involving the left nasal cavity, pterygopalatine fossa, and maxillary sinus cavity via combined nasal endoscopy and Corlu approach under general anesthesia. Postoperative pathology report: (left pterygopalatine fossa, medial wall of the left maxillary sinus) SNIP malignancy (Figure 2(b)). Immunohistochemistry: p-S6K positive. To minimize postoperative recurrence, the patient received postoperative radiotherapy, which was GTV 70Gy/30f, CTV 60Gy/30f.

(a) Nasal endoscopy: a mass was seen protruding from the middle nasal passage of the left nasal cavity. (b) Sinus CT (coronal plane): mass in the left middle nasal passage-maxillary sinus cavity-pterygopalatine fossa area, with bony destruction of the maxillary sinus wall and left skull base. (c) Sinus MR: left lateral nasopharyngeal wall—pterygopalatine fossa—maxillary sinus cavity mass and maxillary sinus wall, left skull base bone destruction, consider malignant tumor lesion may be high. (d) Mass in the left middle nasal passage-maxillary sinus cavity-pterygopalatine fossa area and bony destruction of the sinus wall of the maxillary sinus and the left cranial base are consistent with malignant transformation of an inverted papilloma, and the lesion is slightly reduced in extent when compared to the anterior film. (e) Nasal endoscopy: nasal cavity shows postoperative changes, no recurrence of the mass. (f) Sinus MR: mass in the left middle nasal passage-maxillary sinus cavity-pterygopalatine fossa area and bony destruction of the maxillary sinus wall and left cranial base are consistent with malignant transformation of SNIP, and in comparison with the anterior film, the extent of the lesion is slightly reduced. CT: computed tomography; MR: magnetic resonance; SNIP: sinonasal inverted papilloma.
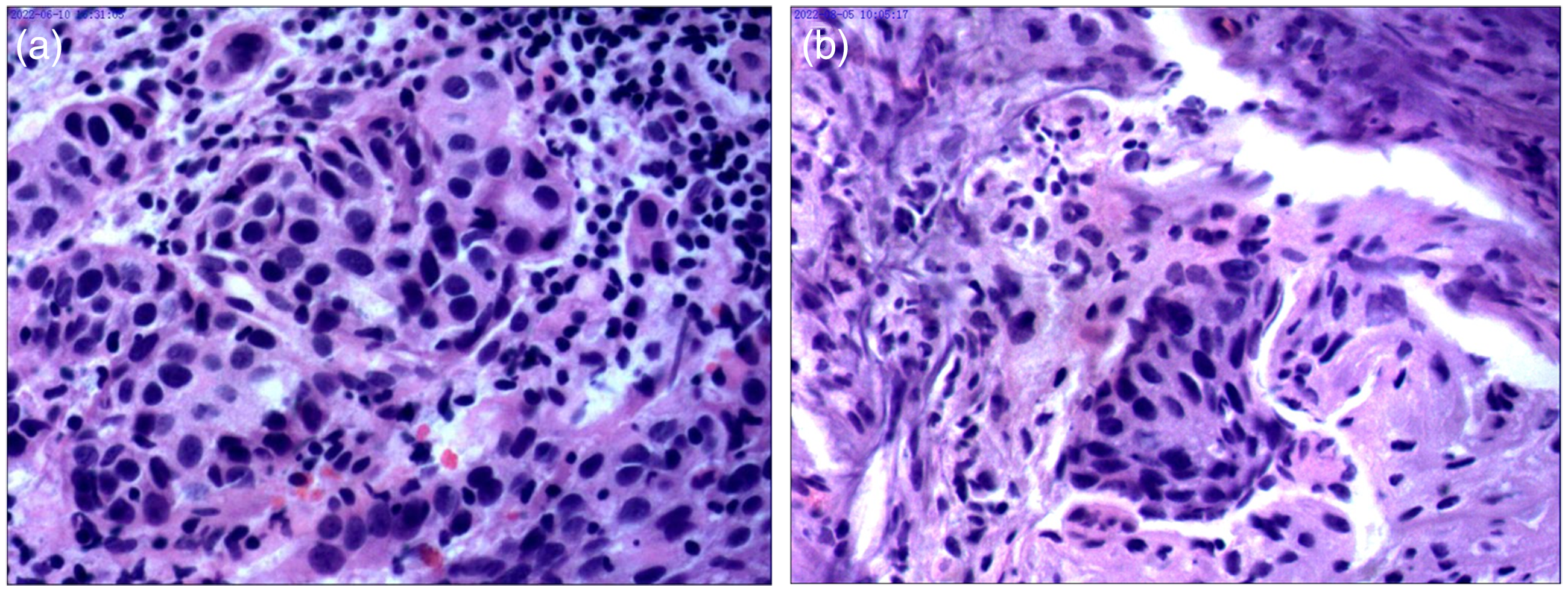
(a) 20×Microscopically, irregular nested cell clusters are seen, proliferating cells are heterogeneous, nuclei are large and deeply stained, pathological karyorrhexis is seen, and infiltrative lesions are seen locally. The lesion is considered: malignant transformation of (left nasal cavity) inverted papilloma. (b) 20× (Left pterygopalatine fossa) Localized cancer nests are seen with local invasion of nerve fibers.
At 2-year follow up, no recurrence was seen under nasal endoscopy and sinus MRI (Figure 1(e) and (f)). All patient details were de-identified. The reporting of this study conforms to CARE guidelines. 2
Discussion
Although SNIP is a benign tumor, it exhibits significant aggressive behavior, including invasiveness, recurrence, and malignant transformation. 3 Studies have shown that the likelihood of malignant transformation of SNIP ranges from 5% to 15% and occurs more frequently in the maxillary sinuses. 4 This report presents a rare case of SNIP malignancy with subsequent invasion of the pterygopalatine fossa, resulting in facial numbness that severely affected the patient's quality of life and necessitated reoperation, this case is significant for guiding the treatment of rare malignant sites of SNIP.
Previous statistics on the cancerous location of SNIP malignant cases, including maxillary sinus, ethmoid sinus, frontal sinus, etc. The location of the lesion did not significantly affect the prognosis of the patient, probably because of the low number of cases of malignancy. 5 In this case, the patient's left maxillary sinus, pterygopalatine fossa, and skull base were damaged by the invasion of cancer cells, leading to non-specific symptoms such as nasal congestion, epistaxis, headache, and facial numbness appeared, which made the diagnosis easily overlooked. The mechanism of SNIP malignancy is unclear, and studies have shown that SNIP malignancy may be associated with human papillomavirus infection. In a study of six cases of SNIP malignant to SCC, it was found that SNIP malignancy may be associated with CDKN2A, KMT2D, NF1, PDE4DIP, CYP2D6, FLT4, and MYH9. 6 SNIP progression and recurrence risk factors also include heavy metal exposure, inflammation, smoking, nasal septal deviation, recurrence cases, and choice of surgical approach for SNIP.7,8 In this case, the patient had a history of open sinus surgery, as well as risk factors including advanced age, a 35-year smoking history, and a deviated nasal septum. Therefore, postoperative follow up and observation should be emphasized.
It is currently believed that the disease should be treated in a comprehensive manner, with surgery being the mainstay. This patient underwent positron emission tomography/CT examination to assess his general condition before surgery, and no cervical lymph node metastasis was detected for the time being. Considering the wide range of tumor invasion in this case, more important functions such as patient's appearance and occlusion were preserved when ensuring adequate resection of the tumor week, and chemotherapy was taken to shrink the tumor before surgery. During the operation, the maxillary sinus was fully opened under nasal endoscopic guidance using the combined Corlu approach. After fully opening the maxillary sinus under nasal endoscopic guidance and exposing the left pterygopalatine fossa, the tumor was separated from the base and normal tissue. Hemostasis was achieved using plasma and bipolar electrocoagulation, and the soft tissue patch was used to repair the surgical cavity after the bone at the junction with the tumor was fully abraded with a grinder. The postoperative period was supplemented with local radiation therapy, which helped the patient's prognosis to some extent. 9 SNIP malignancy can be followed by distant metastases in the brain, lungs, bone, and liver, with lymphatic and systemic metastases rarely occurring. Tawee reviewed previous cases of SNIP malignancy and found that approximately 40% of patients will die from the disease within the first 3 years. 10 What's more, there is a high recurrence rate after surgery, and the 5-year recurrence rate is about 20.34%. 11 Postoperative review is recommended to compare the parameters of quantitative and semiquantitative-enhanced MRI. 12 In addition, serum SCC antigen levels can be used as a molecular marker for SIP recurrence. 13 At present, the patient in this case has no complaints of nasal congestion, runny nose, facial numbness, and other discomforts for 2 years after surgery. No signs of recurrence were seen under nasal endoscopy or enhanced MRI.
With the development of nasal endoscopic surgical techniques and the improvement of surgical instruments, nasal endoscopic surgery, or endoscopic-assisted combined extranasal pathway surgery has gradually become the main method of treatment. It has the advantages of clear intraoperative field of vision, small surgical injury, and reduced facial scarring. There is no significant difference in the postoperative recurrence rate between endoscopic resection of the tumor combined with postoperative radiotherapy and traditional open surgery. 14 Reviewing the case, we treated the case by performing nasal endoscopic surgery, and the high-definition endoscopic view greatly aided our surgical maneuvers in narrow anatomy and complex anatomy. The palatine bone, pterygoid canal, pterygoid nerve, round foramen, and maxillary branch of the trigeminal nerve were revealed along the periphery of the pterygopalatine fossa from top to bottom. The root of the pterygoid process and the inner and outer pterygoid plates were also exposed. Along the mass, sufficient separation was performed into the lateral infratemporal fossa and posteriorly. The cardiovascular anatomy within the mass was unclear. Fortunately, with the assistance of endoscopy, we precisely resected the lesion along the tumor margins, which had a positive impact on controlling the risk of recurrence of the malignant tumor. The patient had a good postoperative outcome, with a shorter hospital stay and significant improvement in quality of life after surgery. Therefore, we recommend a comprehensive treatment approach for cases of extensive malignant transformation of inverted papilloma, utilizing preoperative chemotherapy to reduce tumor size followed by endoscopic surgery.
Conclusion
This case report describes a rare case of malignant transformation of nasal SNIP into SCC with invasion into the pterygopalatine fossa. Given the complex anatomy of the pterygopalatine fossa and its surrounding critical neurovascular structures, a primarily surgical, multidisciplinary approach was adopted. The unique advantages of endoscopic techniques in difficult surgery in terms of demonstrating precise tumor resection, reducing surgical trauma, and improving surgical field of view are discussed. This case suggests that a combination of endoscopic surgery and adjuvant therapy in the management of intranasal papilloma with malignant transformation and invasion of complex anatomical sites may enhance the outcome and improve the patient's prognosis and quality of life. Further studies are needed to clarify the long-term efficacy of this comprehensive approach in similar cases of malignant transformation.
Footnotes
Authors’ contribution
LJ was involved in conceptualization and writing original draft; LW in supervision and writing review & editing; SG in conceptualization. YJ in supervision, funding acquisition, and writing review & editing; and HG in supervision, funding acquisition, and writing review & editing. The manuscript was written through the contributions of all authors. All authors approved the final version of the manuscript.
Ethical and consent statements
This article has not been published or submitted to any journal or meeting. Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Program of Guangzhou (#2024A03J0492); Medical Scientific Research Foundation of Guangdong Province of China(#B2024258); Municipal Schools (Institutes) and Enterprises Joint Funding Theme, Guangzhou Municipal Health Commission Basic and Applied Basic Research Project in 2023 (2023A03J0488); the Science and Technology Program of Guangzhou (# 2023A03J0973).