
Abstract
Objectives:
Patients with drug-related problems are at high risk for perioperative complications. The study aimed to determine the prevalence, number, characteristics, clinical significance and the involved drugs of drug-related problems in inpatients, who were admitted to elective surgery, as well as their burden of comorbidity.
Methods:
The study design was a retrospective, observational study across nine different surgical sites. Patients at admission for elective surgery with ≥ 1 drug-related problem, a hospital stay of ≥ 24 h and at age ≥ 18 years were included. The outcomes of interest were the prevalence and nature of drug-related problems, assessed by pharmacists at hospital admission. The Pharmaceutical Network Europe classification V9.1, the Hatoum scale of clinical significance, the Anatomical-Therapeutic-Chemical classification scheme of the World Health Organization were engaged to categorize drug-related problems and their clinical significance. The Charlson Comorbidity Index was applied to assess the comorbidity of participants.
Results:
The final data set included 11,176 elective surgical inpatients. Of these, a sample of 284 (2.54%) patients was analysed. It was found that 9.89% of the patients showed at least one drug-related problem (average 1.43, SD 0.7). Major causes were drug-drug interactions (30.3%) and supra-therapeutic doses (18.0%). Most drug-related problems were referred to a prescriber for intervention (61.3%). Eighty-two percent of drug-related problems were rated as clinically significant. Cardiovascular drugs were of major concern. Participants’ most common comorbidities were tumour diagnosis (34%), diabetes mellitus with end organ damage (26%) and peripheral vascular diseases (19%).
Conclusions:
Although the prevalence of drug-related problems in this diverse study population was low, drug-related problems were of great importance in terms of their cause and clinical significance. Patients with drug-related problems showed a moderate burden of physiological illness. Study results suggest a need to identify exposed patients with drug-related problems.
Short conclusion
This retrospective, observational study examined drug-related problems in 284 patients admitted to the hospital for elective surgery. It was found that 9.89% of patients had at least one drug-related problem. The most common causes were drug-drug interactions (30.3%) and supra-therapeutic doses (18.0%). The majority of drug-related problems were considered clinically significant (82%). Cardiovascular medications were of greatest concern. The most common comorbidities among participants were tumour diagnosis (34%), diabetes mellitus with end-organ damage (26%), and peripheral vascular disease (19%).
Although the prevalence of drug-related problems was low in this diverse study population, they were important in terms of their cause and clinical significance. Patients with drug-related problems had a moderate burden of physiological disease. The study results suggest a need to identify exposed patients with drug-related problems.
Introduction
A drug-related problem (DRP) is defined by the Pharmaceutical Care Network Europe (PCNE) as ‘an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes’. 1 As such, DRP include adverse drug events, adverse drug reactions and medication errors. 2 DRP can have a considerable impact on individual health and represent a high burden to all health-care systems. As the dose makes the poison, some DRP are challenging to identify and avoid. Preventable DRP contribute to approximately 15% of all emergency department admissions, particularly among the elderly and individuals with multiple medications and underlying health conditions.3–5 In a previous study it was shown that more than half of the patients in ambulatory care were exposed to drugs, which were unknown to their general practitioner despite carrying a high risk for hospitalization. 6 Depending on the setting and the report, more than 15% of all hospital admissions can be linked to DRP. 3 The main issues are insufficient implementation of pharmaceutical services, lack of evidence in their effectiveness, diverse settings and difficulties in identifying high-risk patients for DRP, who are assumed to benefit most from pharmaceutical services.7–11 Little is known regarding DRP in hospital patients and their burden of comorbidity, especially those undergoing elective surgery. This is of particular interest, as the population differs from collectives in most ambulatory care medication management studies in regards of age, type of surgery/surgery ward and medication use.12,13
The overall aim of the study was to analyse the value of an implemented pharmaceutical care service conducted in a pre-anaesthesia clinic, and to assess the burden of comorbidity in those patients. Occurring DRP should be characterized regarding their prevalence, number of DRP per patient, nature of DRP (i.e.: types, causes and resulting pharmaceutical interventions), clinical significance of the DRP and major drugs involved. In addition, participants’ comorbidity was analysed by the Charlson Comorbidity Index (CCI).
Methods
The study explored DRP and categorized them according to the German version of the PCNE classification system V9.1 in a hospital setting. 14 The reporting of this study conforms to the strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15
Ethics
The study was conducted in line with the ethical principles of the Declaration of Helsinki and current Good Clinical Practice. The study protocol was approved by the local ethics committee of Salzburg County, Austria (ID: 1158/2021) which waived the need for written informed consent because of the retrospective nature of the study. The study protocol was registered at the German Register of Clinical Trials (DRKS, DRKS00028763). All data were fully pseudonymized and access was restricted to authorized personnel. Patients could not be identified by others at any point of time.
Study setting and period
The study was conducted at the PAC of the university hospital of Salzburg (SALK), Austria between 1 January and 31 December 2021. According to routine care, patients visiting the PAC were sent from nine different surgical sites:
cardiac surgery, vascular surgery and endovascular surgery (GF) dermatology/allergology (DE) ear, nose and throat diseases (LA) general surgery (CH) gynaecology and obstetrics (GY) oral and maxillofacial surgery (KG) orthopaedics and traumatology (OT) special gynaecology (SF) urology and andrology (UR)
Within the PAC, all patients underwent pharmaceutical face-to-face consultation comprising of medication reconciliation and a comprehensive medication review upon admission, with exception of those who came for day surgery and who were under the age of 18 years. The medication plan and notifications on potential DRP were entered into the digital hospital information system ORBIS (Dedalus HealthCare, Bonn, Germany) and made available for the medical team. Pharmacists’ evaluation on DRP included their individual perspective. However, the team of nine pharmacists at PAC were all clinical trained experts and continuously discussed cases to ensure a high degree of consistency. All DRP were double-checked by a second pharmacist. In a second step, patients encountered an anaesthetist for consultation and medical assessments. Anaesthetists needed to approve the medication plan and the notifications, provided by the pharmacists. Patients met the anaesthetists immediately after the pharmacists. Anaesthetists were free to contact the pharmacists in case of remaining questions. Regarding the overall medical conditions, patient approval for surgery relied on the anaesthetists’ appraisal. The setting is based on inter-professional collaboration with the overall aim of increasing patients’ perioperative safety and quality of care by managing surgical, anaesthesia, pharmaceutical and laboratory concerns in a best possible way.
Study design and participants
The study design was a hospital-based retrospective, observational study. All patients fulfilling the eligibility criteria were included in the study. Considering a confidence level of 95% (and 10% prevalence of DRP in elective surgical patients), it was shown that for a number of 300 patients with DRP, a precision of ±5% was given. Hence, the power of the study was set at three hundred patients, who met the inclusion criteria and who were randomly drawn out of the study collective.
Inclusion criteria of the study were
visit of the PAC in the year 2021 due to elective surgery at one of the remaining surgical wards
age ≥ 18 years
hospital stay of more than 24 h and
at least one documented DRP by pharmacists addressed in pharmaceutical interventions
Patients undergoing day care surgery and at age of <18 years were excluded from the study.
Statistical analysis
Data on medication review were extracted from the patients’ medical charts using the digital hospital information system ORBIS. Patient data was entered in a clean Excel file. Data management (coding and cleaning) was done by a trained researcher (SC). To avoid risk of classification bias, DRP were detected (out of written pharmaceutical interventions) and classified by two independent researchers (one clinical pharmacist (KK) and one master class student (CS)). For process validation, classification results of assessments were discussed among each patient case in regular peer meetings (CS, KK, SC) from July until December 2022. Inconsistencies induced further research on patient history and were resolved through discussion. During this process, a Standard Operating Procedure was developed aiming a consistent classification process of DRP. Frequencies, percentages, means, standard deviations and ranges were calculated using Excel® Software version 1912 (Microsoft, Redmond, Washington, USA). Data was presented using figures, graphs and PCNE codes.
Outcomes
The primary outcome of the study was the proportion of the study participants meeting the inclusion criteria with at least one DRP at hospital admission, documented by pharmacists of the PAC (prevalence of DRP).
Secondary outcomes were the assessed nature of DRP, the clinical significance, major involved drugs and the burden of comorbidity. Furthermore patient characteristics according to socio-demographic aspects (sex, age), medication (number of drugs at admission), hospital ward, lengths of hospital stay, pre-operative risk classes 1–4 (via classification of American Society of Anesthesiologists, ASA) rated by anaesthetists, and approval of operation by anaesthetists were investigated as tertiary outcomes. 16
DRP were categorized by three different standardized classification systems:
PCNE classification system V9.1
14
:
DRP were classified among their type, cause and intervention. Manifest DRP were defined as causing an impact on the patient and the therapy, whereas potential DRP might have led to manifest real problems in the future. Hatoum scale
17
:
DRP were categorized regarding five levels of clinical significance: 1 (adverse significance – leading to an adverse outcome), 2 (no significance), 3 (somewhat significant), 4 (significant) and 5 (very significant). Level 6 (extremely significant) was excluded as life-threatening situations were immediately managed by the hospitals’ emergency teams. WHO Anatomical-Therapeutic-Chemical (ATC) classification
18
:
The system was used to classify the most commonly implicated medication groups.
The burden of participants comorbidity was assessed by the CCI.
19
Missing data
Only complete cases of medication review data were included in the study. Missing values for patient characteristics (e.g.: approval of operation) were documented and assumed to be low.
Results
Prevalence of DRP
At PAC, 11,176 patients were recorded in 2021. This collective included day care surgery patients and patients under the age of 18 years. Of the whole collective, 31.85% (n = 3560) were 18 years or older with an inpatient surgery (hospital stay >24 h). Of the total 3560 patients, 9.89% (n = 352) had at least one DRP identified by one of nine different pharmacists (via two-eye principle) of the PAC at time of hospital admission. Out of this study population, three hundred patients were randomly drawn and were included in this study. After screening the included patients for data completeness, 16 patients were excluded due to documentation issues. Consequently, 284 patients remained in the study. A patient flow diagram is shown in Figure 1.

Patient flow diagram.
The mean age of participants was 72.41 years (SD 10.78), ranging from 23 years of the youngest patient to 93 years of the oldest participant. The majority of patients were of male sex (63.03%) and was admitted for elective surgery at the urological and andrological hospital site. Characteristics of the study population are displayed in Table 1.
Patient characteristics (N = 284).

Frequencies, proportions, means, SDs and ranges are presented.
CCI: Charlson Comorbidity Index; ASA: American Society of Anesthesiologists; SD: standard deviation; NA: not applicable. NA was documented in cases of missing data, which consisted low (<5%) per variable and occurred due to documentation issues. GF: cardiac surgery, vascular surgery and endovascular surgery; DE: dermatology/allergology; LA: ear, nose and throat diseases; CH: general surgery; GY: gynaecology and obstetrics; KG: oral and maxillofacial surgery; OT: orthopaedics and traumatology; SF: special gynaecology; UR: urology and andrology.
Most common comorbidities according to the CCI of patients were tumour diseases (34%), diabetes mellitus with end organ damage (26%) and peripheral vascular diseases (19%). A list of all comorbidities is shown in Table 2.
Comorbidities of the study population (N = 284).

Calculations according to the Charlson Comorbidity Index of elective surgical patients. 19
AIDS: acquired immunodeficiency syndrome; CCI: Charlson Comorbidity Index.
About 284 patients were found to have 405 detected DRP (1.43 DRP per patient, SD 0.7). In more detail, 196 patients showed one single DRP (69%), 64 patients showed two DRP (22.5%) and 17 patients three DRP (6%). The maximum number of DRP per patient in this sample was six. A comparison between participants’ major problems, causes, interventions and significance levels of DRP are displayed in Figure 2. The full data on the DRP classification is available at supplement 1.
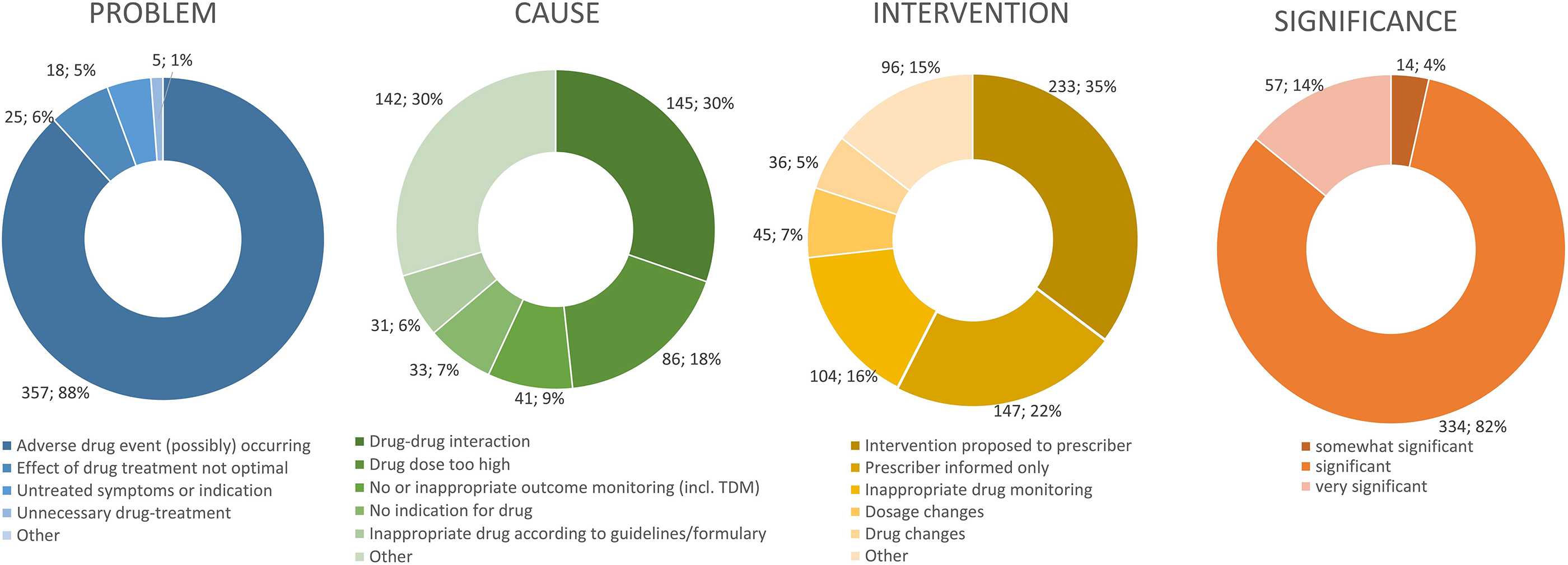
Problem, cause, intervention and significance of DRP found in patients (N = 284) undergoing elective surgery, represented in absolute (n) and relative (%) frequencies.
Type of DRP
DRP were mainly on medication safety, regarding potential adverse effects (88.1%), and less frequently on effectiveness (10.6%). The vast majority of DRP were potential problems (92.3%).
Cause and planned intervention of DRP
Drug-drug interactions were a leading concern (30.3%), supra-therapeutic doses led to 18.0% of the DRP. Medication reconciliation was a rare problem with 3.6% of the DRP causes. Most DRP were referred to the prescriber for interventions (61.3%).
Clinical significance of DRP
The DRP were rated for their clinical significance according to the six-level Hatoum scale, with level one representing the lowest, and level six the utmost significance. 17 Most interventions were rated as significant (82%). There was no negative significance and no intervention at the lowest two and on the highest level.
Involved drugs
In addition to the DRP classification and the significance level, drugs, which caused the DRP were analysed and stratified according to the ATC groups. In total, 671 drugs were involved in DRP, most of them multiple times. Cardiovascular drugs as a group, and simvastatin, pantoprazole and acetylsalicylic acid as specific drugs were of major concern. Details on drugs, the frequency of involvement into DRP and the ATC groups are displayed in Figure 3. These 15 drugs comprised of 42% of all DRP.

Most common ATC-groups, agents: involved drugs in DRP, displayed in relative (%) and absolute (n) frequencies.
To get a better picture, typical statements were taken from medication review records (Table 3).
Frequent and typical examples of DRP, how they were managed and their classification into the PCNE system.

Discussion
This study differs from most other medication review studies by the considerably different patient population on elective surgical wards. With the focus on patients at admission, the study gained interesting insights into this particular setting, at the initial point of the hospital stay.
In contrast to other projects in this field, a high number of adult patients of any age and at any state of (co)morbidity were included. Whereas the number of DRP in other studies was around seven (elderly patients with polymedication), it was much lower in this ‘general population’, with just 1.4 DRP per patient. 13 A potential explanation for the relatively few DRP is the young age of several patients, included in this study. Pharmacists of the PAC also mentioned an agreement with the anaesthetists on which DRP should be reported, and which ones should not be mentioned. The focus of the medication review hence was rather on medication safety than on an optimization of the long-time medication therapy plan. However, this low number is in line with recent studies in surgery by Albayrak et al. and by Mohammed et al..20,21 Male patients were exposed to DRP to a higher extent. Urology and andrology contributed one quarter of the cases, the largest group of patients with DRP in this study. As urological patients benefit from interaction checks and dosage adjustments, this high number seems reasonable. 22 At admission and in expectation of an elective surgery, the focus of the medication review was rather on medication safety and on avoiding risks during the intervention, than on a comprehensive optimization of the long-term medication therapy. This might explain the emphasis on drug safety issues. Approaches to increase medication safety in surgery are in line with the ASA Task Force on Paranesthesia Evaluation, which highlights the safety of perioperative care, improved outcomes, and patient satisfaction when assessing anaesthetic risks. 23 Cardiovascular and psychotropic drugs play an important role upon the DRP. With drug selection as the major single cause for DRP, and almost all interventions rated at clinical significance in the Hatoum scale, the detected few DRP still seem to be extremely meaningful. These results differ from a recent study by Oki et al., who found untreated indications, sub-therapeutic dosages and inappropriate administration as the most frequent DRP, and anti-infective drugs as the most relevant ATC class for DRP in surgery. 24 The difference in findings to our study can be explained by the later timing of the medication review during hospital stay. While the medication review was conducted in the perioperative period during the study of Oki et al., medication reviews were conducted at hospital admission in our study, and thus much earlier in the surgery course. Later medication reviews hence tend to find different patterns of DRP. 25 Major morbidities of participants in the study were related to oncologic diagnosis and diabetes with end organ damages. Specifically cancer patients are related to several risks for DRP and patients with type 2 diabetes mellitus require intensive disease management.26,27
Implications for policy, practice and research
It is of special notice that many DRP at admission for elective surgery were caused by a few similar drugs. In a previous study, it was shown that patient selection for medication review should depend on the mere number of prescribed drugs. 10 This might be true for patients with polymedication but not for the surgery setting, where only few drugs are taken in many cases. One potential focus for patient selection in this setting hence can be the prescription of the mentioned 15 drugs, which frequently led to DRP. Despite the low number of DRP, clinical significance is definitely given and the quotations from the hospital records underlined this impression. At the same time, it is obvious that patient selection cannot be restricted to the patients taking these 15 drugs, nor be limited to a few indications, as the other half of patients would have been missed.
The identified DRP have implications for surgery, particularly in managing statin medications commonly prescribed for cardiovascular risk reduction. According to ASA Surgical guidelines, patients should continue cholesterol medications to reduce mortality risk. Perioperative statin use, like Simvastatin, has shown benefits such as faster bone regeneration and improved early postoperative outcomes.28–30 However, appropriate preoperative assessment of statin use is crucial to manage dosage limits, adverse effects and monitoring parameters. Failure to address these DRP could impact surgery, potentially leading to delayed or cancelled cases. Therefore, proactive management of statin-related DRP is essential for optimizing surgical outcomes and holds relevance for other practice sites. 31
Strengths and limitations of this study
The study included a very large patient sample over 12 months at admission for elective surgery and was based on the latest PCNE classification of DRP (9.1). Data were analysed only retrospective. Patients varied widely regarding their inclusion criteria, which can be regarded as a strength and a limitation at the same time. The study was conducted at a single hospital only. Medication reviews were done by several pharmacists with different levels of experience, but were checked by dual control principle. The pharmaceutical care service was conducted during the COVID-19 pandemic, which may have influenced processes of the PAC and the service itself.
Conclusions
The study has analysed the nature of DRP upon admission on elective surgery. Patient safety has likely increased from handling DRP in a multi-professional team. It was shown that DRP are less frequent at this specific moment at admission in the surgery course, while they still can cause significant problems. In the shade of other studies, a conclusion of this project is that the number and kind of DRP varies with the setting, but also with the point of time, when the medication review is conducted. While a medication review with a focus on medication reconciliation and drug safety seems to be meaningful upon admission, untreated indications, inappropriate application and sub-therapeutic dosages seem to be predominant after the surgical intervention, in the perioperative situation. In an outpatient setting, patients with obvious problems or higher numbers of prescribed drugs seem to be eligible for a comprehensive medication management with a focus on long-term medication.10,32 That means that a medication review and its focus need to be tailored, according to the setting and the moment, when it is conducted. Appropriate aspects need to be selected from the inventory of potential medication review activities. 33 Consequently, medication review at hospital admission to elective surgery would likely benefit from a selection process on patients with high-risk of showing DRP. This study identified 15 drugs or indications, which seem to be closely related to DRP in this setting. While special attention can be paid on these 15 drugs, they cannot be regarded as an exclusive selection criterion. Further research should address additional risk factors.
Supplemental Material
sj-docx-1-sci-10.1177_00368504241263534 - Supplemental material for Drug-related problems in elective surgical inpatients: A retrospective study
Supplemental material, sj-docx-1-sci-10.1177_00368504241263534 for Drug-related problems in elective surgical inpatients: A retrospective study by Clara Simon, Olaf Rose, Karin Kanduth, Johanna Pachmayr and Stephanie Clemens in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504241263534 - Supplemental material for Drug-related problems in elective surgical inpatients: A retrospective study
Supplemental material, sj-docx-2-sci-10.1177_00368504241263534 for Drug-related problems in elective surgical inpatients: A retrospective study by Clara Simon, Olaf Rose, Karin Kanduth, Johanna Pachmayr and Stephanie Clemens in Science Progress
Footnotes
Acknowledgements
The authors would like to thank the study participants for taking part in the study and the pharmaceutical team of Dr Ulrike Porsche and Dr Martin Wolkersdorfer at patient admissions of the university hospital Salzburg for provision of the medication review dataset.
Author contributions
SC, KK, CS, and OR conceived and designed the analysis. SC, KK, CS collected and analysed the data. SC and CS performed the analysis. SC and OR supervised the study. OR and CS wrote the paper. SC, KK, CS, and OR interpreted the data, corrected and approved the manuscript.
Data availability statement
The original dataset analysed during the current study is available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.