
Abstract
The SARS-CoV-2 (COVID-19) pandemic called for the restructuring of National Health Service (NHS) surgical departments across the country. Initial guidance advised that patients undergoing elective surgery isolate for 14 days prior to their operation. As we learnt more about COVID-19 and its incubation period, at the Princess Royal University Hospital this guidance has been decreased to 72 h. We collected retrospective data for two patient cohorts that underwent elective surgery in June and September 2020, isolating for 14 days and 72 h, respectively. We followed-up these patients with several questions allowing us to categorise the cohorts into three groups based on their compliance with isolation measures and also to assess their satisfaction with the isolation process. Our data shows that only 16% of the June cohort and 53% of the September cohort isolated in accordance with the guidelines whilst patient satisfaction was 16% and 64% respectively. These results highlight a suboptimal compliance to pre-operative guidelines as well as an adverse effect on patient mental health and raise the issue of both patient and NHS staff safety. With the possibility of a COVID-19 second wave and for future pandemics, a clear evidence-based plan for pre-operative isolation is vital. Furthermore, consideration of patient adherence and satisfaction is key in deciding which guideline will be most effective.
Introduction
The 27th of December 2019 saw the first reported case of the COVID-19 pandemic. 1 Almost a year later, COVID-19 continues to impact hospital policy on a nationwide scale. Several urgent changes were introduced to aid the NHS in dealing with the strain of COVID-19. 2 Departmental infrastructure was adapted in anticipation of the ‘peak’ and healthcare professionals across the country were redeployed.
Surgery was one of the main departments to undergo major restructuring. As many of the surgical team were redeployed all over the hospital, new systems were put in place to allow critical elective operations to continue. 3 Simultaneously, other non-urgent elective cases were postponed.
Patients undergoing surgery are known to have an increased susceptibility to infection. 4 A recent study of 1128 patients investigating 30-day mortality post-operatively showed a significantly increased risk of death in patients with COVID-19. 4
Surgery can create aerosol generation from intubation, abdominal deflation in laparoscopic surgery, pre- and post-operative patient contact and many other sources.5,6 In order to protect healthcare staff and minimise the risk of infection, surgical departments adopted guidance for patients to isolate for 14 days in order to minimise risk of virus transmission. By educating patients about isolation and implementing strict methods to prevent transmission, it is possible to significantly reduce perioperative COVID-19 infection. 7
Since then, The Princess Royal University Hospital has adopted new practice where patients are only required to isolate for 72 h prior to elective surgery. This followed King’s College Hospital Trust guidance for emergency planned surgery. 8 We predict that patients isolating for a longer period of time may struggle to follow these guidelines. This raises the question of how well 14-day isolation guidance is followed and whether adherence is better with a shorter isolation.
Method
As pre-operative isolation is not usually required for elective cases, we anticipated that the implementation of this guidance would be challenging, especially for our cohort isolating for 14 days. We collected retrospective data for two patient cohorts who underwent elective surgery at the Princess Royal University Hospital. The first cohort of 25 patient isolated for 14 days prior to their surgery. The second cohort of 36 patients isolated for 72 h prior to their surgery. We asked our cohorts a series of questions regarding their isolation pre-operatively, including:
1. Did the patient isolate pre-operatively and for how long?
2. What daily activities patients carried out during their isolation period?
3. Who patients self-isolated with and what activities they did together?
4. What activities household members took part in during the isolation period?
5. How patients travelled to and from the hospital for their operation?
For our guidance on pre-surgery isolation during the COVID-19 pandemic, we used Guy’s and St Thomas’ (GSTT) guidelines. 9 The questions in our study were formulated by consensus of the authors considering the GSTT guidelines and based on this, we stratified our two cohorts into three groups:
Green included patients who isolated with their household bubble or away from household members taking part in other activities. A person from their isolating bubble or hospital transport was used on their operation day.
Amber included patients who isolated at home but left the house for exercise alone or with someone from their house.
Red included patients who did not adequately isolate pre-operatively or travelled to hospital by taxi, public transport or with someone outside of their bubble. Patients interacting with others who went shopping or received visitors were included in this category.
In order to assess the adverse impact on patient well-being in each of the cohorts, we asked the following question:
6. Overall, did you find it difficult to isolate?
Here, again, responses were categorised into red, amber and green according to their response. Below, the table highlights which words or phrases were used by the patients and how we decided to categorise them. Patients in the green category were not dissatisfied whilst patients in the red category portrayed a strong dissatisfaction. Those in the amber category lay somewhere in-between.

Patients in both cohorts were called again 7 days post-surgery and asked whether they have developed shortness of breath, a fever or cough. This aim of this was to assess development of COVID-19 symptoms in the study group.
Results
In the 14-day isolation cohort, 1 out of the 25 patients admitted to not following the isolation protocol. This compared to zero in the 72-h cohort. However, when the more detailed questions were analysed, a far higher proportion of participants were found to have broken their isolation.
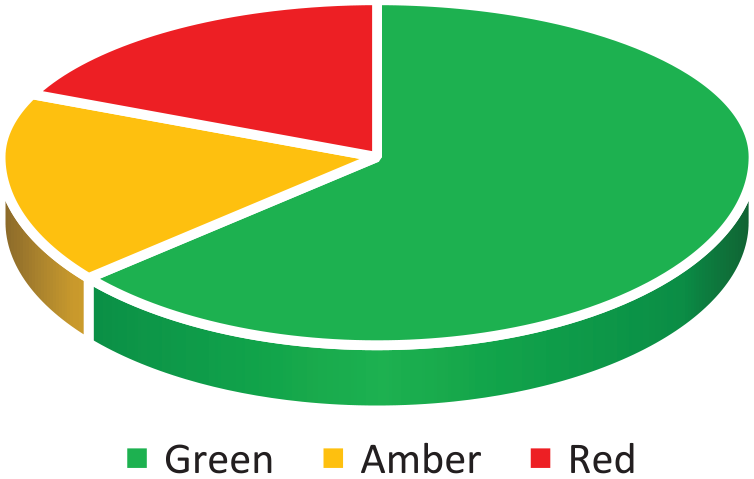
In the 14-day cohort, 48% of patients fell into the red category, 36% into the amber category and 16% in the green category (Figure 1). This contrasts to the 72-h cohort where 53% of patients fell into the green category, 17% into amber and 30% into the red category (Figure 2). A breakdown of responses to the questions asked, provides further insight into which isolation activities were usually adhered to (Figures 3 and 4).

Fourteen-day isolation cohort by category.

Seventy-two-hour isolation cohort by category.

% of 14-day cohort adhering to isolation guidelines by category.

% of 72-h cohort adhering to isolation guidelines by category.
When looking at overall patient satisfaction with the isolation process, this was greatly increased in the 72-h cohort when compared to the 14-day cohort.
In the 14-day cohort, 40% fell into the red category with regards to patient satisfaction, 44% into the amber category and 16% into the green category (Figure 5). All four of the patients who fell into the green category for satisfaction also fell into this category with regards to isolation compliance.

Patient satisfaction with 14-day isolation period.
In the 72-h isolation cohort, 64% of patients fell into the green category, 17% into the amber category and 19% into the red category (Figure 6).
Patient satisfaction with 72-h isolation period.
In order to investigate whether there was a significant difference in isolation compliance between the two cohorts, a Chi Squared analysis of our data was performed. Due to a low n for some categories, we also carried out a Yates correction in order to obtain the final p-value.
Chi squared analysis with Yates correction yielded a p-value of 0.036, showing a statistically significant difference between the two cohorts. Our data showed a decrease in the number of patients who isolated sub-optimally (amber and red) between the 14-day and 72-h groups. Simultaneously, an increase in the number of patients isolating correctly (green) between the two cohorts was noted.
Our calculated p-value and the trend of categories between the two cohorts shows us that there was a statistically significant better adherence to isolation guidelines in the 72-h cohort.
Seven days post-surgery, none of the patients from either cohort had developed shortness of breath, a cough or fever. Unfortunately, it was not possible to re-swab the cohorts for a more accurate measurement of post-surgery COVID-19 infection.
Discussion
From our study data, there is clearly a suboptimal level of patient isolation prior to surgery reflected in both cohorts. 84% and 47% of the 14-day and 72-h cohorts respectively did not isolate as required pre-surgery (Figures 1 and 2).
There was a large difference in successful isolation between the 14-day and 72-h cohorts. The 14-day isolation period was introduced to minimise the risk of patients having surgery whilst incubating COVID-19. Compliance, however, has not been fully considered and if 84% of a patient cohort failed to isolate correctly, we should consider whether that guidance is an effective policy. This is further supported by our second cohort of patients. When asked to isolate for 72 h, there was a much higher compliance to the pre-surgery instructions.
For the 14-day cohort, a large percentage (64%) our study group failed to distance from household members who were not isolating (Figure 3). Patients often limited their own daily activities, however, they would continue to interact with others who went shopping or had visitors. There is a clear infection risk between the household member in contact with others and the isolating person.
We hypothesise that a significant number of the population was unable to shop online as the demand for e-commerce greatly increased. Figure 7 shows a dramatic increase in overall internet retail sales in the UK during the March–June 2020 period. We theorise that a general avoidance of physical grocery shopping and the increase of ‘stockpiling’ prevented a number of our cohort from accessing online shopping services. This would force household members to break isolation during the pre-surgery 14-day period in order to buy essentials.

Value of internet retail sales monthly in the United Kingdom (UK) from January 2016 to June 2020. 10 .
For the 72-h cohort, the largest factor leading to a failure to follow the isolation guidance was the transport to the hospital (Figure 4). All of these patients were living alone and had to resort to public transport, taxi services or friends/family outside of their household bubble to drive them to and from the hospital.
This raises the issue of whether patients going for surgery have access to hospital transport and highlights the need to consider arranging transport for these specific patients in order to allow them to comply with isolation guidance.
Patient satisfaction is greatly increased in the 72-h cohort when compared to the 14-day isolation cohort (Figures 5 and 6). This must be considered when producing future isolation policies. If a patient is dissatisfied, then they are less likely to conform to isolation guidelines. It is also vital to consider patients’ mental health and by comparing the two cohorts (Figures 5 and 6) it is likely that this is impacted by the duration of self-isolation. A longer isolation period was associated with decreased patient satisfaction and, we hypothesise, negative impact on mental health.
Interestingly however, the four patients who were not dissatisfied with the isolation protocol, were also completely compliant. This may relate to the patient’s perceived importance of their operation, encouraging them to tolerate the isolation. If a 72-h isolation is bearable and strictly observed, then is this better for patient and staff safety than a longer period with poor compliance?
Conclusion
It is clear from our data that initial guidance on isolating for 14 days pre-operatively was not adhered to by the majority of patients. Isolation guidance for the 72-h cohort, however, was better followed. Compliance to isolation guidelines would theoretically decrease risk of COVID-19 transmission. Therefore, we propose that consideration of a shorter pre-operative isolation period may improve adherence and benefit both patients and NHS staff. It is also worth considering emergency surgery where patients are not able to isolate pre-operatively at all. In these cases, patients have a COVID-19 swab either the day before or on the day of surgery.
Predictably, patient satisfaction with the isolation process is increased with a shorter isolation period. However, this needs to be balanced against the safety of patients and staff.
For the 14-day isolation cohort, accessibility to shopping services may play a large part in their isolation. A solution to this problem would be an online service providing patients in isolation with priority online shopping. Availability of hospital transport for patients living alone was relevant for both cohorts. Transport services for patients living alone would provide an alternative means that would not infringe upon isolation guidance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.