
Abstract
This report presents a unique finding of an incidental right internal carotid artery dissection in an asymptomatic 69-year-old man. The report highlights the possible trigger and long-term outcomes of this condition. The patient had participated in Japanese archery competitions for many years. His medical history included hypertension and a prior ischemic stroke in the left lateral medulla, resulting in Wallenberg syndrome. During a routine visit, head magnetic resonance angiography revealed right internal carotid artery dissection. He was managed conservatively with antiplatelet therapy and close monitoring. Follow-up imaging after 10 years showed no changes, and the patient remained asymptomatic. Therefore, routine screening for incidental findings is important even in asymptomatic patients. Archery competitions may be a possible trigger for internal carotid artery dissection. The presence of re-entry in the lesion at the time of onset can be a predictor of a good long-term prognosis.
Keywords
Introduction
Internal carotid artery dissection (ICAD) is a relatively common cause of cerebrovascular disease, particularly among young people.1–3 The etiology of ICAD can be classified as traumatic or spontaneous based on specific clinical presentations and underlying etiological factors such as connective tissue or vascular disorders. Some idiopathic cases were caused by sport-induced neck hyperextension or flexion. 4 Conservative treatment with medical therapy is given priority; since cases with worsening symptoms have been reported, diagnosis and treatment are important in the acute phase. 4 Here, we describe a case of ICAD in an older man who remained asymptomatic and showed no change on imaging 10 years after disease onset.
Patient information and clinical findings
The patient provided written informed consent for the publication of their case.
Patient
A 69-year-old man.
Current medical history
He attended the neurology clinic for regular check-ups in January 2013. Annual magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) scans were conducted as a standard procedure because of the frequent association between Wallenberg syndrome and vertebral artery dissection in Japanese patients (Figure 1(a)). MRI conducted in 2013 indicated stability, whereas MRA revealed dissection in the right internal carotid artery (ICA) spanning from the cervical to the petrous level.

MRA are shown 1 year before onset (A), at onset (B), 2 months after onset (C), and 120 months after onset (D). A dissociated lesion with reentry is seen in the right internal carotid artery (arrow); no progression is seen at the site of dissociation after 120 months.
The old infarction displayed T2 hyperintensity, diffusion-weighted hypointensity, and high signal intensity on the apparent diffusion coefficient map spanning from the left cerebellum to the dorsolateral left medulla oblongata. Cerebral atrophy remained unchanged from that in the previous year.
Cranial MRA revealed a dissection in the right ICA, extending from the cervical to the petrous region (Figure 1(b)).
Additionally, given the rarity of carotid artery dissection in Japanese patients, we suspected the potential for artifacts and conducted head angiography using computed tomography (3D-CTA). This investigation confirmed the presence of right ICAD, which started immediately before entering the carotid canal and extended within the canal (Figure 2(a)–‒(c)).

CT-Angio at onset, showing right internal carotid dissection with re-entry (yellow arrow). True(blue arrow) and false (red arrow) lumens.
Medical history
Hypertension, ischemic stroke in left lateral medulla with Wallenberg syndrome (diagnosed in 2001).
Patient background
No alcohol consumption or smoking. He had been involved in Japanese archery competitions for 37 years.
Findings on arrival (2013)
Blood pressure: 131/86 mmHg, pulse rate: 55/resting.
No cognitive impairments, such as apraxia, agnosia, aphasia, or dysmnesia, were evident. There was no apparent acroparalysis. Additionally, there were no signs of deep tendon hyperreflexia or pathological reflexes, and there was no ataxia in the upper and lower limbs and trunk. Notably, there was dissociated sensory loss in the left frontal region, specifically hyposensitivity to warmth and pain, which has remained unchanged over the past few years.
He had a National Institutes of Health Stroke Scale score 5 of 0. Eyelid conjunctival anemia was not detected. Eye movements were normal bilaterally. The Barre's sign was negative for both upper extremities. Additionally, the Romberg's sign was negative.
Follow up and outcomes
Important follow-up diagnostic and other test results
The patient underwent conservative management with antiplatelet therapy and close monitoring. Cranial MRI + MRA was conducted every 2 to 3 months in the first year, biannually for the next 1 to 3 years, and annually thereafter. Ultrasound was omitted because of the location of the dissection site. Imaging showed no changes after a decade (Figure 1(c) and (d)) and the patient remained symptom-free with no unexpected events.
Discussion
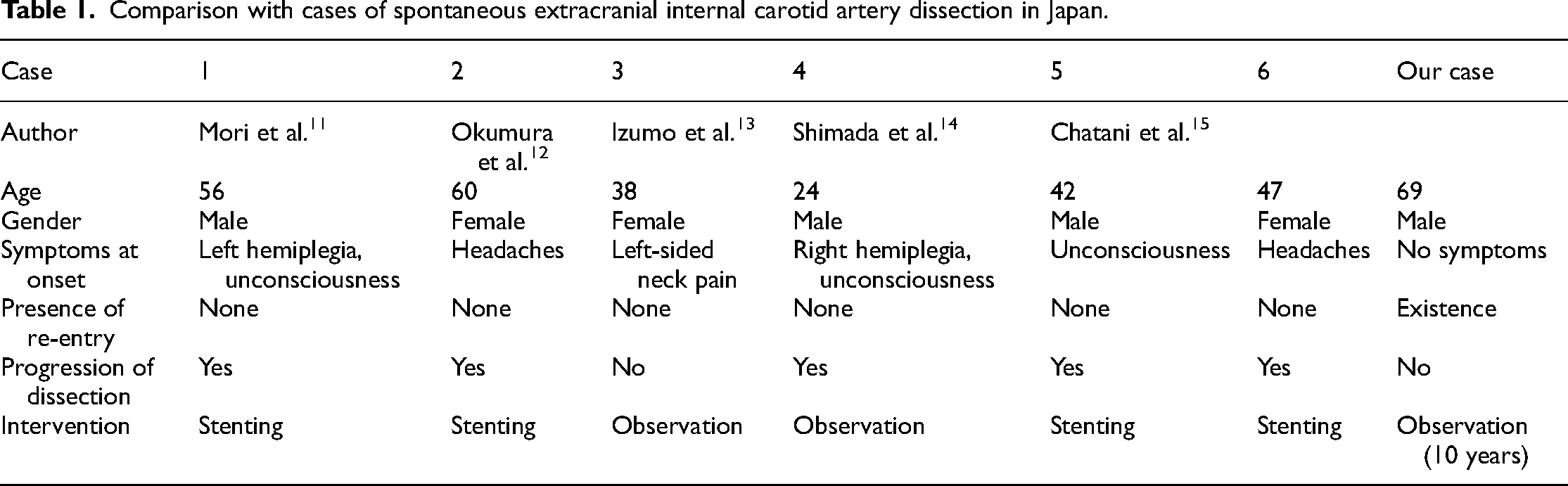
Carotid artery dissection typically occurs distal to the carotid at the C2-C3 level. 6 It is caused by cervical rotation with hyperextension of the ICA due to neck flexion opposite the lesion at the C2-C3 level. 7 Four mechanisms exist for blunt carotid artery injuries 8 : prevalent type II results from neck hyperextension and opposite rotational movements. 9 The upper cervical vertebrae (C1-C3) extend more forward than the lower (C4-C7), which can stretch the cervical ICA over lateral processes during hyperextension. This is worsened by rotation at the atlantoaxial joint due to potential anterior movement of the opposite C1 transverse process. In our case, the patient's 37-year archery history until 2013 prompted us to consider a type II carotid artery injury due to frequent right neck hyperextension. Imaging revealed dissection up to the C1 level, possibly from contact with the transverse process of the right C1 vertebra during cervical hyperextension, as reported previously.6,7 In patients without trauma or medical complications, obtaining a medical history of the mode of onset is important. 4 While ICAD treatment strategies remain controversial, conservative or antithrombotic therapy is suggested because of the generally favorable outcomes. In 10% of the cases that worsen rapidly, bypass surgery or stenting may be required. Adverse outcome predictors include an ICA diastolic diameter of >10 mm and no re-entry. 10 None of the aforementioned conditions were observed in this patient, and he remained in good health over the 10 years of follow up. The patient's stability over this extended period suggests that conservative management and meticulous monitoring are effective strategies for asymptomatic patients with ICAD, and achieving re-entry may be considered a favorable outcome. In this case, cranial MRI + MRA was conducted every 2 to 3 months in the first year, biannually for years 1 to 3, and annually thereafter. For asymptomatic patients, we recommend MRI + MRA at 3 months, 6 months, 1 year, and annually thereafter. Archery may have triggered ICAD, highlighting the need to assess lifestyle factors. Table 1 lists cases of spontaneous extracranial ICAD cases in Japan. A PubMed search was conducted using the query “spontaneous extracranial internal carotid artery dissection Japanese.” Patients with connective tissue disorders were excluded from this study. Our study, when compared to previous reports, revealed that cases lacking re-entry typically exhibited lesion progression, suggesting that it is a potential adverse prognostic indicator.
Comparison with cases of spontaneous extracranial internal carotid artery dissection in Japan.
Conclusion
This case offers valuable long-term insight into the right ICAD in an asymptomatic 69-year-old man. His archery history, which is a potential trigger, has not been reported in the medical literature. The case's progression indicates that conservative management with vigilant monitoring effectively prevents complications, and the initial re-entry might predict a positive outcome.
Footnotes
Abbreviations
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Tokuharu Tanaka, he is a Assistant Professor of Family Medicine. He holds a PhD in Medicine. His research area is Sarcopenia and Health Promotion.
Osamu Yamamura, he is a Professor of Community Medicine. He holds a PhD in medicine. His research area is Sarcopenia, Neurology and Health Promotion.
Hidenori Onishi, he is a Assistant Professor of Community Medicine. He holds a PhD in Medicine. His research area is Community Medicine and medical laboratory science and Public Health and Geriatrics.
Masamichi Ikawa, he is a professor of Community Health Science. He holds a PhD in medicine. His research area is community health, neurology and medical genetics.
Hiroyuki Hayashi, he is a Professor of Family and Emergency Medicine. His research area is medical education.
Tadanori Hamano, he is a Professor of Neurology Medicine. His research area is Clinical Neurology and Biochemistry and Cell biology of Alzheimer’s disease.