
Abstract
Objective:
Two walking tests including the six-minute walk test (6MWT) and the incremental shuttle walk test (ISWT) are widely used to evaluate functional ability in individuals with disease conditions. However, it remains unclear whether these walking tests effectively manifest clinical impairment in individuals with asymptomatic peripheral artery disease (PAD). We aimed (i) to compare the walking performance of individuals with and without asymptomatic PAD using the 6MWT and ISWT, and (ii) to investigate the correlation between ankle-brachial index and toe-brachial index (ABI-TBI) and the walking distance.
Methods:
A cross-sectional, crossover, matched pairs design was employed in this study. Asymptomatic PAD was diagnosed using ABI-TBI measurements. Seventy-six participants (38 with asymptomatic PAD and 38 without PAD) were randomly ordered to perform the walking tests. During the 6MWT, participants walked along the 30-meter corridor at their self-selected pace for six minutes, and the six-minute walk distance (6MWD) covered was recorded. In the ISWT, participants walked at a 12 prescribed speed level, and the incremental shuttle walk distance (ISWD) covered was recorded.
Results:
Result revealed no difference in 6MWD between individuals with asymptomatic PAD and without PAD (mean distance: 501.6 m vs 516.8 m, p = 0.24). Asymptomatic PAD individuals exhibited a significantly shorter ISWD than those without PAD (median distance: 270 m vs 340 m, p = 0.003). No participants reported any leg pain symptoms during the 6MWT and ISWT. A statistically significant positive correlation was observed between the right leg TBI and ISWD in all participants (r = 0.23, p = 0.04).
Conclusions:
Individuals with asymptomatic PAD demonstrated poorer walking performance than those without PAD when assessed using ISWT but not the 6MWT. Asymptomatic PAD is also associated with diminished walking performance during the ISWT. Thus, ISWT may show the clinical impairment in this population.
Keywords
Introduction
Peripheral arterial disease (PAD) is characterized by the narrowing of peripheral artery system, typically results in a reduction of blood flow to limbs. 1 Major risk factors for developing PAD include advancing age, diabetes, smoking, dyslipidemia, hypertension, and physical inactivity. PAD links to increased heart disease and stroke, which are the leading cause of death. 2 PAD extends to affect physical illnesses, including intermittent claudication (IC), rest pain, ischemic ulcer, and even gangrene in distal tissue lesions, which can result in limb loss. Consequently, this leads to a reduced quality of life. 3
Functional ability represents the capability to perform aerobic tasks that require an integration of the following components: cardiovascular, pulmonary, and skeletal muscle systems. Regarding PAD characteristics presenting a reduced blood flow to working muscles during activity, several studies have employed the treadmill test as a standard tool to evaluate the changes in functional ability in individuals with symptomatic PAD.4–7 However, the graded walking test using a treadmill is limited in the community; thus, field walking test is likely to be an alternative measure.
Six-minute walk test (6MWT) and incremental shuttle walk test (ISWT) are the two most widely used to evaluate functional performance in people with disease conditions. Existing studies investigating functional ability using 6MWT with PAD have found that individuals with symptomatic PAD had shorter six-minute walk distance (6MWD) than those without PAD.8,9 In addition, 6MWD positively correlated with ABI in individuals with symptomatic PAD. 10 On the other hand, a previous study has suggested using ISWT as a superior measure to 6MWT in assessing functional impairment in people with symptomatic PAD. 11 While most studies have focused on individuals with symptomatic PAD, asymptomatic PAD is neglected, as many individuals with PAD have latent disease or are asymptomatic. 12 In addition, a suitable walking test that would be able to manifest clinical impairment for those with asymptomatic PAD is also unknown. Thus, this study aims to (i) compare the maximum walking distance and leg pain by 6MWT and ISWT between individuals with asymptomatic PAD and without PAD, (ii) to explore the correlation between ABI-TBI and the maximum walking distances. Identifying a proper walking test would provide clinical impairment information for PAD patients with asymptomatic severity.
Materials and methods
Ethics approval
This study was conducted following the Declaration of Helsinki and approved by the Research Ethics Committee at the Research Institute for Health Sciences, Chiang Mai University (approval number: 01/2023, approval date: 19 January 2023). All eligible participants provided a written-consent form before participation.
Study design and participants
This study is a cross-sectional, crossover, matched pairs design, investigating participants with asymptomatic PAD and without PAD living in Chiang Mai, Thailand. Participants were recruited from 21 January 2023 to 25 September 2023, through public announcement at the Endocrine Outpatient Department, Maharaj Nakhon Chiang Mai Hospital and online media. Participants were selected consecutively based on inclusion and exclusion criteria of the study. Inclusion criteria were: (i) PAD (defined if ABI score ≤0.9 or TBI score ≤0.7; presence asymptomatic PAD using San Diego claudication questionnaire (SDCQ) 13 ) or non-PAD (defined if ABI score > 0.9 and TBI score >0.7),14,15 (ii) aged ≥20 years or above, (iii) both sexes, (iv) able to communicate and follow the study instruction. Participants were excluded if they had the following conditions: (i) presence of musculoskeletal conditions such as severe arthritis, (ii) presence of neurological disorders such as hemiplegia, (iii) presence of unstable/ untreated heart diseases, (iv) presence of respiratory diseases such as chronic obstructive pulmonary disease and asthma, (v) unable to walk independently or use walking aids.
Sample size was estimated from primary outcomes (i.e. 6MWD and ISWD) based on our pilot study. Mean and standard deviation of ISWD (PAD vs non-PAD: 238 ± 42.1 m vs 286 ± 55.9 m, respectively), with an effect size of 0.9 was considered to calculate due to maximum sample size identified. To ensure that we obtain sufficient statistical power to provide a statistical significance for all outcomes, the effect size was adjusted to the lower border (effect size = 0.8) of the large effect size. With 90% power, 5% type I error, a sample size of 68 was required. To allow 10% dropout rate, a total sample size of 76 was needed.
Measurements
Ankle-brachial index (ABI) and toe-brachial index (TBI)
ABI and TBI were evaluated by a well-trained assessor using automated ABI-TBI meters (Automated ABI-TBI, VaSera VS-1500 N device, Fukuda Denshi, Japan). The automated ABI measure has a moderate inter-rater reliability, expressed as ICC = 0.7.
16
The automated TBI also has moderate reliability (ICC = 0.7),
17
high sensitivity and specificity (82.35% and 92%, respectively) for PAD detection.
18
Participants were asked to rest in a supine position for 10 min in a room with a constant temperature of 22 degrees celsius. Blood pressure cuffs were placed on each limb. This automatic device simultaneously measured blood pressure in both arms and one ankle, both arms and the other ankle side, and both arms and both great toes, respectively. Arteries were assessed by an automated sphygmomanometer and standard oscillometric algorithms. Blood pressure measurements were performed twice each, with systolic blood pressure not exceeding 10 mmHg. ABI was calculated by the following formula;


TBI was computed based on the following equation.


Six-minute walk test (6MWT)
Participants were instructed to walk on a 30-meter corridor, round-trip trail for six minutes. The participants must walk as far as possible at their self-selected speed. At the end of each minute during the test, the participants were provided a standardized encouragement using standard phrases and neutral tones (e.g. you are doing well, you have 5-min left). All participants were tested twice with a minimum of 30-min rest interval between the tests. The farthest distance covered of the two trials was used to analysed. 19 During the test, vital signs (i.e. heart rate, respiratory rate, blood pressure, oxygen saturation), fatigue levels, and other adverse events (e.g. dizziness, fainting, and pale face) were monitored. The test was terminated if participants experienced some of the termination criteria following the exercise testing guidelines. 20 6MWT was measured by a well-trained assessor.
Incremental shuttle walk test (ISWT)
The ISWT consists of 12 levels, with the time signals continuing for 12 min. 21 Participants were asked to walk on a 10-m-long corridor following a given bleep sound. A walking speed increment of 0.17 meters per second was adjusted every minute, with an initial speed of 0.5 meters per second (level 1) and last speed of 2.37 meters per second (level 12). The test was terminated when participants could not maintain the determined speed or meet the termination criteria following the exercise testing guidelines. 20 The maximum walking distance covered was analysed. ISWT was evaluated by a well-trained assessor.
Leg pain scale
Leg pain was measured using a visual analogue scale for peripheral artery disease. 22 The pain scale ranges from 1 to 5, in which a higher score indicates more severe pain.
Physical activity level
Physical activity was assessed using a short version of the International Physical Activity Questionnaire (IPAQ). 23 The short version of IPAQ is valid and reliable.23,24 This questionnaire encompasses eight items which focus on time spent vigorous activity, moderate activity, walking, and sitting. Metabolic equivalent in a minute (MET-minute) was computed for each activity. Physical activity level is interpreted as inactive, minimally active, or high active based on a MET-minute achieved.
Procedure
On a screening day, general information, health status, and PAD diagnosis were evaluated. On the same day, participants were asked to perform a walking test based on a random order either 6MWT or ISWT obtained. A 2-day washout period was considered between different walking tests in order to prevent a carry-over effect. All participants were instructed to refrain from vigorous exercise, caffeine consumption, and smoking at least 24 h before testing. The details of each participant were de-identified using codes that were not linked to the participants’ personal information.
Statistical analyses
Data were analysed using IBM SPSS statistics, version 22.0 for Windows. Demographic data were presented by descriptive statistics. The Shapiro-Wilk test was used to identify the data distribution. For baseline characteristics, the Chi-square test was used for dichotomous variables (i.e. sex, smoking history, underlying diseases, SDCQ, and physical activity level) while independent t-test (i.e. age, BMI, ABI for asymptomatic PAD and non-PAD groups, and TBI for asymptomatic PAD group) and Mann-Whitney U test (i.e. TBI for non-PAD group) were used for continuous variables. An independent t-test was used to determine the between-group differences in 6MWD during 6MWT while Mann-Whitney U test was used to detect for ISWD during ISWT. Pearson correlation was utilized to calculate a correlation between the worst ABI and 6MWD, while Spearman's correlation was used for the worst ABI and 6MWD correlation, the worst TBI and 6MWD and ISWD correlations. Correlation coefficient is interpreted as very weak (0.0–0.19), weak (0.2–0.39), moderate (0.4–0.59), strong (0.6–0.79), and very strong (0.8–1.0). A significant difference was set at p < 0.05. The reporting of this study conforms to STROBE guidelines. 25
Results
Eighty-three participants were screened. Seven participants were excluded due to symptomatic PAD, asthma, and refusal to participate. A total of 76 eligible participants completed the study procedure (Figure 1).

Flow diagram.
Baseline characteristics between asymptomatic PAD and non-PAD groups are shown in Table 1. No differences in age, sex, BMI, smoking history, underlying diseases, ABI, and physical activity level between PAD and non-PAD groups. The asymptomatic PAD group had significantly lower TBI than the non-PAD group (p < 0.001). The asymptomatic PAD group had significantly higher PAD symptoms than those with non-PAD (p < 0.001).
Baseline characteristics.

ABI, ankle-brachial index; BMI, body mass index; kg/m2, kilogram per square meter; M, male; n, number; non-PAD, without peripheral artery disease; PAD, peripheral artery disease; SDCQ, San Deigo claudication questionnaire; TBI, toe-brachial index; %, percentage
After completing 6MWT, the asymptomatic PAD group had a 3.1% shorter 6MWD than the non-PAD group (PAD vs non-PAD: 501.6 ± 62.2 m vs 516.8 ± 50.0 m), but the difference was not significant (p = 0.24) (Figure 2). The asymptomatic PAD had a 20.6% significantly shorter ISWD than those with non-PAD (PAD vs non-PAD: 270 (220–340) m vs 340 (287.5–370) m) (Figure 3). No participants reported any leg pain during the 6MWT and ISWT.

Six-minute walk distance between asymptomatic PAD and non-PAD. PAD, peripheral artery disease.

Incremental shuttle walk distance between asymptomatic PAD and non-PAD. PAD, peripheral artery disease.
For correlation analyses, no correlations between the worst ABI and 6MWD and ISWD were observed (the worst ABI-6MWD: r = -0.13, p = 0.26; the worst ABI-ISWD: ρ = -0.006, p = 0.95). The result of correlation between the worst TBI and walking distance showed that the worse TBI positively correlated with ISWD (Figure 4), but not with 6MWD (Figure 5).
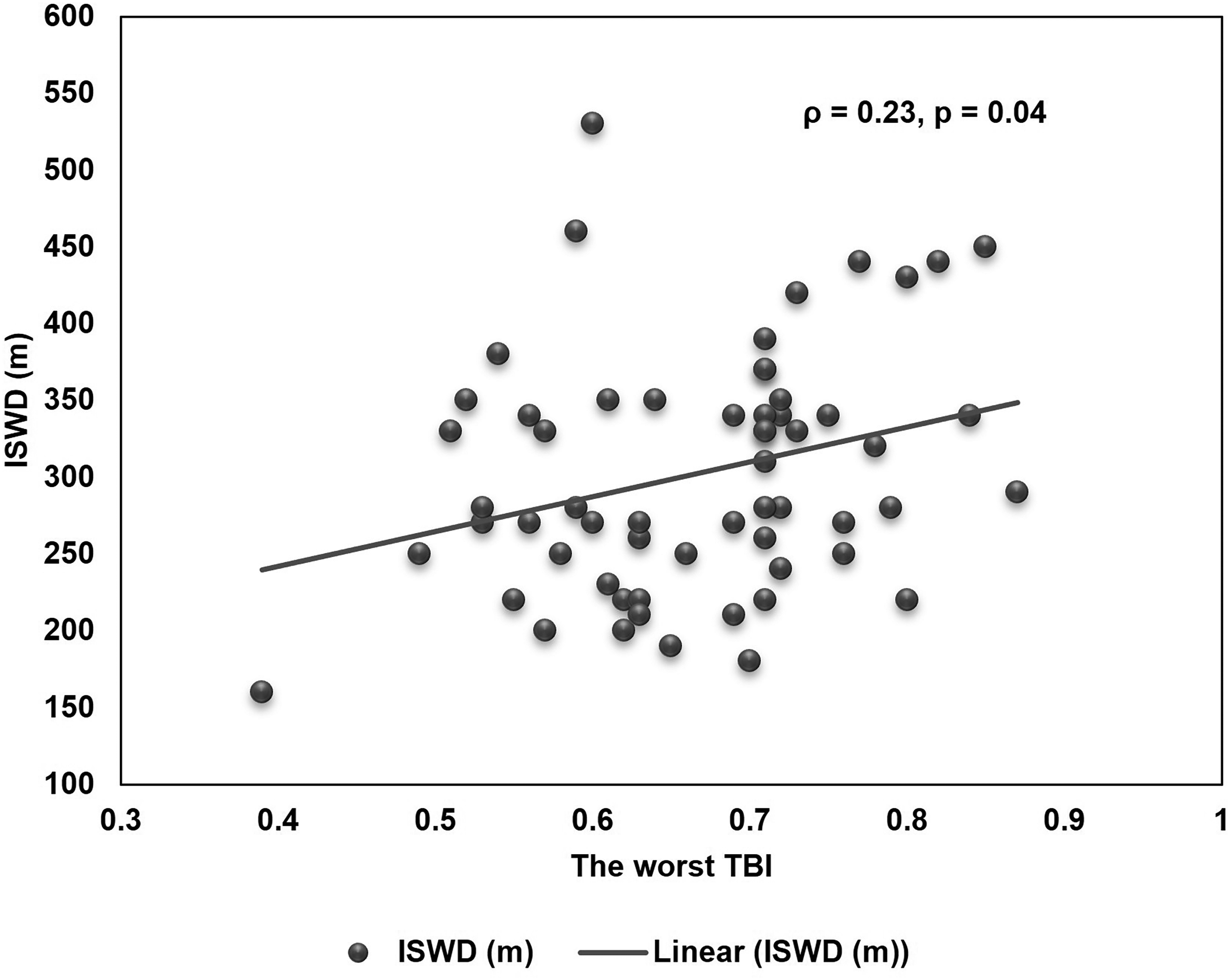
Correlation between TBI and ISWD. TBI, toe-brachial index; ISWD, incremental shuttle walk distance.
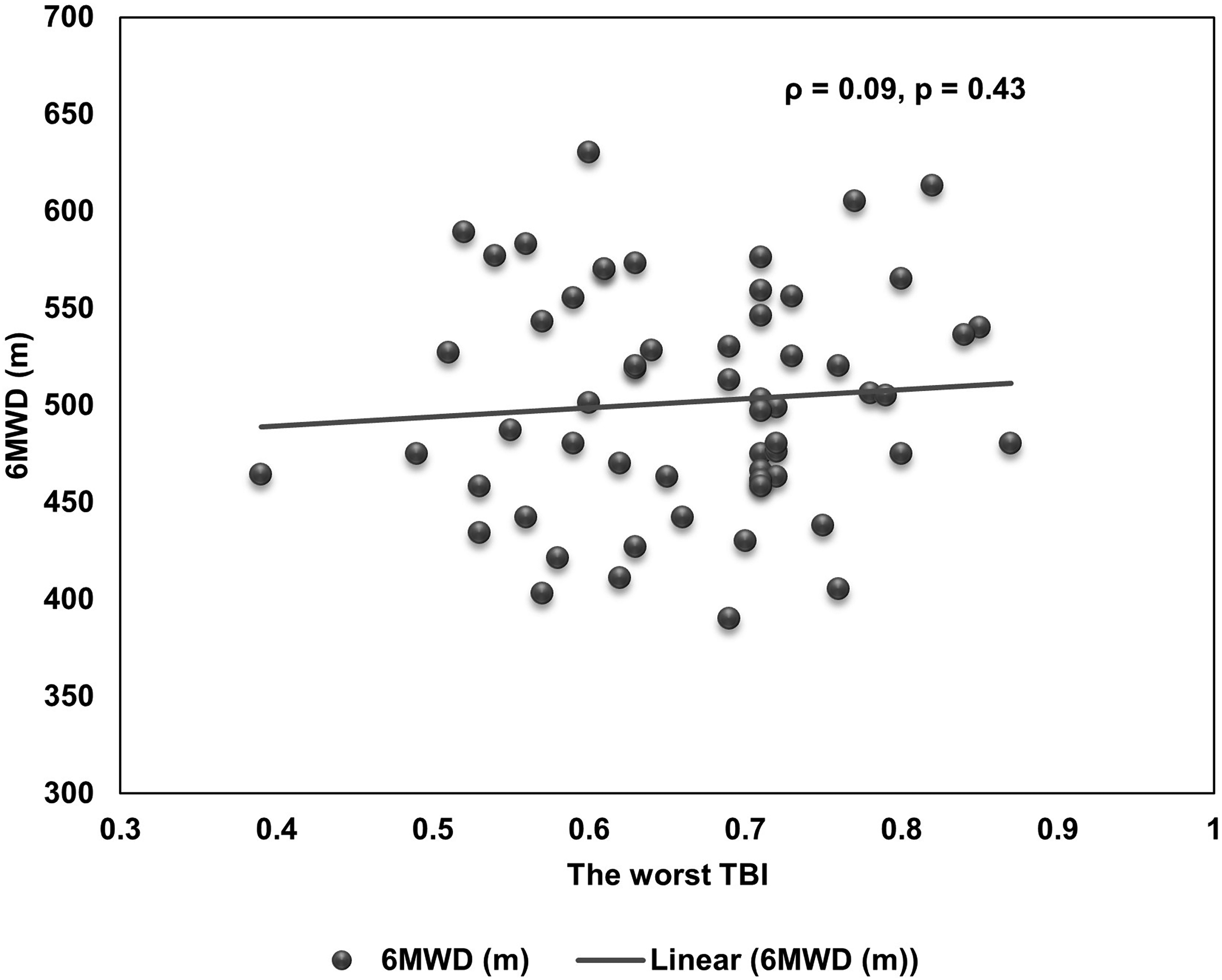
Correlation between TBI and 6MWD. TBI, toe-brachial index; 6MWD, six-minute walk distance.
Discussion
Findings of this study provide evidence that individuals with PAD had poorer walking performance, as indicated by a shorter walking distance when assessed using the incremental shuttle walk test. In addition, the incremental shuttle walk distance positively correlated with toe brachial index. Taken together, the evidence suggests a promising performance of ISWT as a potential walking test to manifest a clinical impairment for individuals with asymptomatic PAD.
Since PAD is characterized by poor blood perfusion resulting from narrowing of the artery conduit, 1 functional ability (i.e. walking test) has been recognized. Two most field walking tests widely used are 6MWT and ISWT. Our data found a comparable walking distance between asymptomatic PAD and non-PAD individuals when assessed using 6MWT. This finding is inconsistent with previous evidence, revealing a shorter 6MWD in individuals with symptomatic PAD than non-PAD participants.8,9 On the other hand, our finding supports the use of ISWT, as indicated by a 20.6% significantly shorter walking distance in individuals with asymptomatic PAD than those without PAD. The finding is in agreement with a previous study suggesting a superior measure in ISWT to 6MWT in assessing functional impairment in people with symptomatic PAD. 11 Poorer walking performance in individuals with asymptomatic PAD, when assessed using ISWT but not the 6MWT, is attributed by the characteristics of the ISWT and asymptomatic PAD. ISWT is characterized as a progressive exercise test, which increases an energy demand and induces muscle activation, resulting in enhanced blood supply. 26 In individuals suffering from PAD, blood perfusion to active muscle tissue may be limited by progressive exercise activation, resulting in lower walking performance. Furthermore, the participants had predominantly less symptomatic PAD, indicating that individuals with PAD, particularly those with asymptomatic PAD, may require progressive speed as measured by ISWT to reveal disease manifestations rather than self-selected speed as measured by 6MWT. Poorer walking performance in the current study is consistent with a previous observational study reporting an impaired lower extremity functioning in individuals with asymptomatic PAD. 12
In this study, the lack of a correlation between walking distance and ABI may be explained by the lower sensitivity of ABI in individuals suffering from medial arterial calcification. Medial arterial calcification typically begins to develop in individuals aged 40. 27 Physiologically, calcification occurs in the Tunica media (a middle layer of artery), 28 resulting in poor compression and underestimation of PAD by ABI. Our study participants, with a mean age of 46 years, may have falsely normal ABIs. Consequently, these participants, who have false negatives for PAD, may exhibit shorter walking distance. In contrast, TBI is generally less influenced by medial arterial calcification since collateral vessels of the toe are less prone to calcification. 29 Our study reveals a significant correlation between walking distance and TBI. The finding that the incremental shuttle walk distance positively correlated with TBI provides a complementary support for the use of the ISWT to exhibit clinical impairment in individuals with asymptomatic PAD. It should be noted that such a correlation was of small magnitude (r = 0.23), which should be interpreted with caution.
This study has some limitations that should be considered. First, most participants in this study had less severity based on TBI measurement, asymptomatic PAD, and majority of female. These factors may limit generalizability. Second, the correlation between ISWT and TBI was small. Future study with a comprehensive severity and more sample size are needed.
Conclusions
This study concludes that individuals with asymptomatic PAD had poorer walking performance when assessed using ISWT but not the 6MWT. Asymptomatic PAD was associated with a diminished walking performance during ISWT. Thus, ISWT may show the clinical impairment in individuals with asymptomatic PAD.
Footnotes
Acknowledgements
This study was partially supported by Chiang Mai University.
Author contributions
Conceptualization, S.N., B.C., K.R., S.B. S.Ka., N.P., and J.K.; Data curation, C.S. and S.Ko.; Formal analysis, S.N.; Investigation, S.Ka., N.P., and J.K.; Methodology, S.N. and B.C.; Supervision, B.C.; Writing—original draft preparation, S.N.; Writing—review and editing, all authors.
Data availability statement
All data for this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted following the Declaration of Helsinki and was approved by the Research Ethics Committee at the Research Institute for Health Sciences, Chiang Mai University (approval number: 01/2023, approval date: 19 January 2023).
Informed consent
All participants were provided a written informed consent before participating in the study.