
Abstract
Objective:
To investigate the diagnosis and treatment procedure of synovial chondromatosis (SC) of the temporomandibular joint (TMJ).
Methods:
Clinical features, imaging features, surgical methods, and prognosis of 7 patients with SC of the TMJ were analyzed. We also reviewed and analyzed surgery-relevant literature included in the Pubmed database in the past decade using the search terms “synovial chondromatosis” and “temporomandibular joint”, and found 181 cases.
Results:
There was no specific difference in the symptoms of SC in the TMJ in different Milgram’s stages in our cases and the cases mentioned in the literature. The main symptoms of SC in the TMJ were pain (100%, 7/7; 64.64%, 117/181), limited mouth opening (57.14%, 4/7; 53.59%, 97/181), swelling (14.29%, 1/7; 28.18%, 51/181), crepitus (28.57%, 2/7; 19.34%, 35/181), and clicking (14.29%, 1/7; 9.94%, 18/181) in our cases and cases from literature separately. The imaging features of SC were occupying lesions (including loose bodies or masses) (71.42%, 5/7; 37.57%, 68/181), bone change in condyle or glenoid fossa (1/7, 14.29%; 34.81%, 63/181), effusion (42.86%, 3/7; 20.99%, 38/181), joint space changes (42.86%, 3/7; 11.05%, 20/181) in our cases and cases from literature separately. The surgical procedures seem to depend mainly on the involved structures and the extension of the lesion rather than the Milgram’s stage.
Conclusions:
The clinical features of SC in the TMJ are nonspecific and easy to be misdiagnosed. MRI is helpful in the diagnosis of SC in the TMJ. The surgical procedures mainly depend on the involved structures and the extension of the lesion.
Introduction
Synovial chondromatosis (SC) is a rare benign disease characterized by the formation of metaplastic cartilage in the synovial membrane of joints, resulting in cartilaginous nodules and loose bodies. 1 SC often occurs in large synovial joints such as the elbow, knee, wrist, and hip. 1 Only 3% of all SC cases occur in the temporomandibular joint (TMJ). 2
The common clinical signs and symptoms of SC in the TMJ are pain, limited mouth opening, preauricular swelling, malocclusion, crepitus, and clicking sound during mouth opening. 3 These nonspecific signs of SC can lead to a delay in the diagnosis or misdiagnosis as more common diseases such as temporomandibular disorders (TMD).3,4 However, the SC of the TMJ cannot spontaneously resolve and does not respond to conservative treatment. Surgery is the only effective treatment of SC in the TMJ. 5 Incomplete excision of the lesion may result in recurrence. 6 A 30% recurrence rate of SC has been reported after arthrotomy in large joints. 7
According to the pathological classification, Milgram divided SC into three stages.1,2,8 Stage I: chondrogenesis occurs in synovial mesenchymal stem cells, with no formation of loose bodies; Stage II: a transitional lesion with active chondrogenesis in synovium and cartilaginous nodules enlarge or are released into the articular cavity as loose bodies; Stage III: chondrogenesis in the synovial membrane disappears and loose bodies can be observed.
A proper understanding of clinical and pathological features of SC in the TMJ is crucial for the correct diagnosis and selection of the appropriate surgical intervention. This study introduces seven new cases of SC in the TMJ in different Milgram’s stages and reviews the literature related to SC in the TMJ and surgery treatment from 2011 to 2021.
Materials and methods
This study was approved by the Medical Research Ethics Committee of the Affiliated Stomatology Hospital of Guangzhou Medical University (No. LCYJ2022012), and adhered to the principles of the Declaration of Helsinki on medical protocol and ethics. Seven patients with SC of the TMJ diagnosed and treated in the Affiliated Stomatology Hospital of Guangzhou Medical University from July 2015 to March 2021 were retrospectively analyzed. The collected data included epidemiological characteristics, clinical symptoms, imaging findings, treatment, and outcomes (Table 1).
Information of 7 patients with synovial chondromatosis in the TMJ.
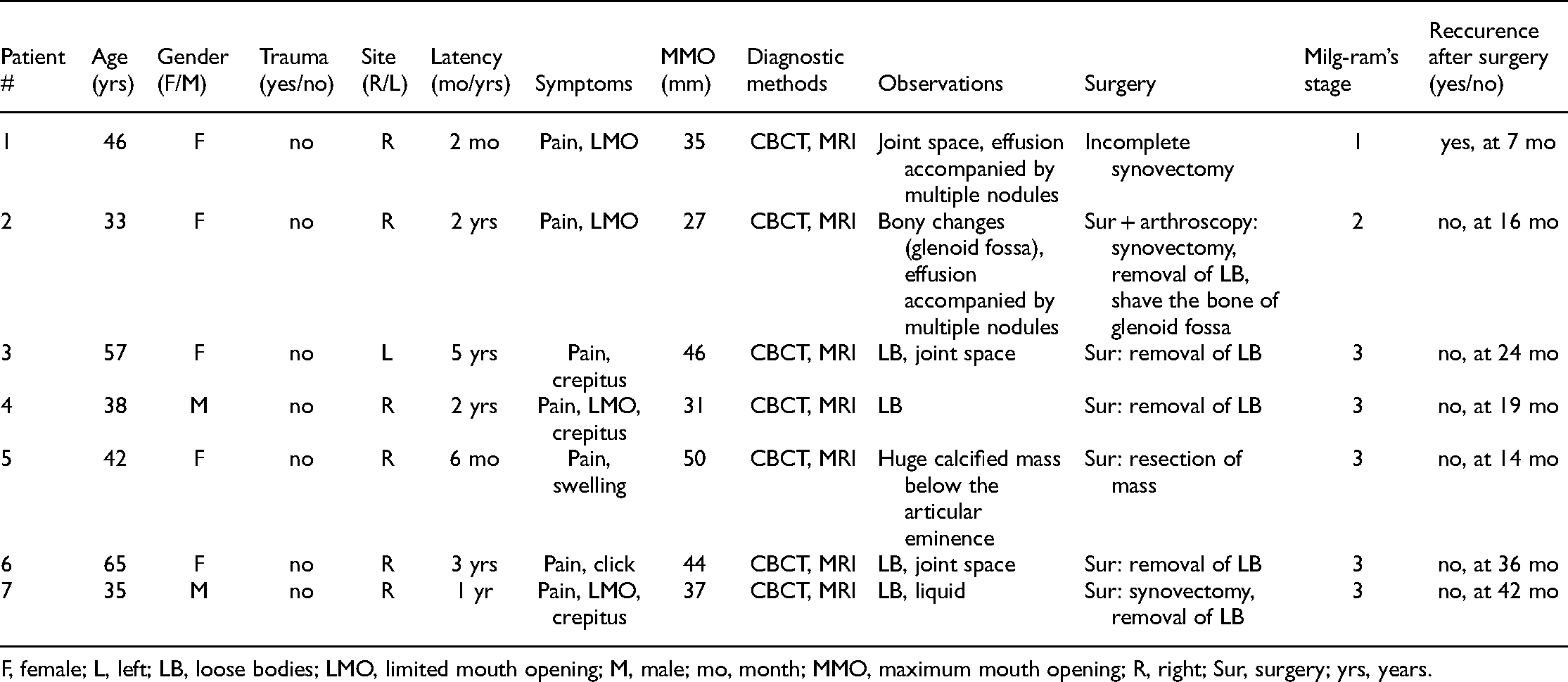
F, female; L, left; LB, loose bodies; LMO, limited mouth opening; M, male; mo, month; MMO, maximum mouth opening; R, right; Sur, surgery; yrs, years.
All reviewed articles and publications about SC were searched systematically in the National Library of Medicine’s PubMed database. The articles included were clinical studies published from 2011 to 2021, of which the treatment included at least one case of surgical intervention. For each study, the following data were recorded for discussion: name of first author, year of publication, patients age and gender, localization (right-left), clinical signs and symptoms, diagnostic imaging techniques used, imaging findings, type of surgical intervention used, Milgram’s stage, pathological results, follow-up time, and prognosis. Each case was recorded individually when multiple cases were reported in a single publication.
Results
Among the 7 patients (2 male, 5 female) with SC in the TMJ treated in our hospital, the average age of disease diagnosis was 45.14 ± 11.88 years. All results are listed in table 1.
All 7 patients underwent first cone-beam computed tomography (CBCT) examination, followed by magnetic resonance imaging (MRI) examination of the TMJ. At least one of the results showed imaging features of SC in the TMJ. Calcification of loose bodies or masses detected by CBCT was 71.43% (5 of 7). The bone destruction of the glenoid fossa was 14.28% (1 of 7), and the widening of the joint space on the affected side was 42.86% (3 of 7). Equal or low signal intensity scattering in the high signal image reflecting loose bodies scattering in joint fluid was found in MRI images in 3 out of 7 cases. Six patients were treated with open surgery, and one patient was treated with arthroscopy-assisted open surgery. One patient showed disease recurrence 8 months after surgery. The patients’ information is shown in Table 1. Typical cases are shown in Figures 1–2.
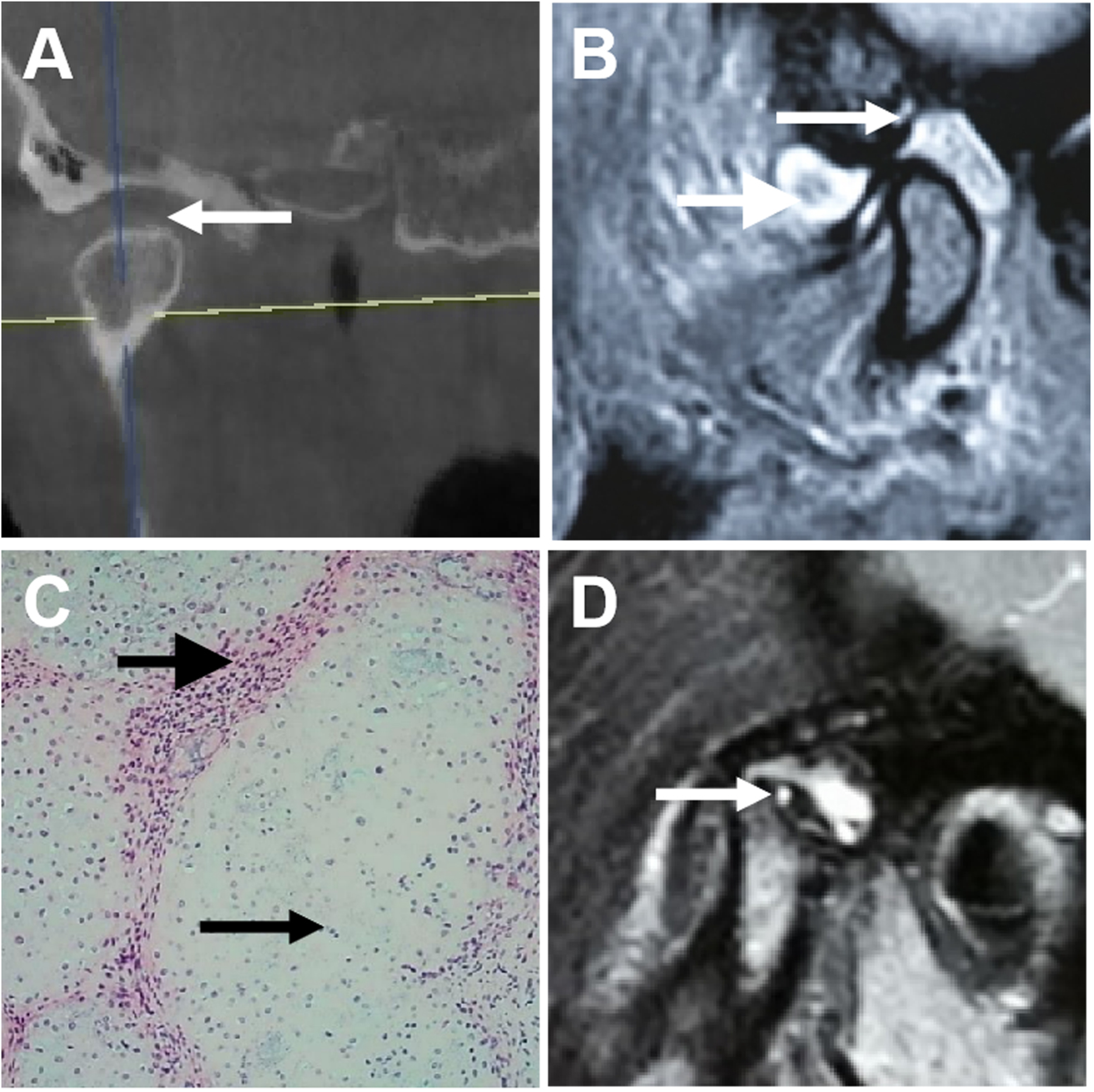
Patient 1 with temporomandibular joint synovial chondromatosis with recurrence after open surgery. A) CBCT image: Expanded articular cavity (arrow). B) MRI image: Before surgery, cartilage nodules (small arrow) and joint fluid (large arrow). C) Histology (HE): Multinodular TMJ synovial chondromatosis with epithelioid cells (small arrow) and spindle-shaped cells (large arrow). D) MRI image: 8 months after surgery, recurrence of temporomandibular joint synovial chondromatosis (arrow: Loose body).

Patient 2 with temporomandibular joint synovial chondromatosis did not reveal recurrence after arthroscopy-assisted open surgery. A) CBCT: Destructed glenoid fossa bone (arrow). B) MRI: Joint fluid (arrow) illustrating an enlarged joint capsule. C) Arthroscopy: Loose bodies (arrows). D) Histology (HE): Dense fibrous tissue (small arrow) at the surface with cartilage (large arrow) underneath.
The last search of cases in the literature was made on October 25, 2021, which resulted in 102 publications. Excluded were 43 publications, since they were unrelated to surgery or the full text could not be obtained. The remaining 59 publications were recorded in the annexed list Excluding 1 identical case reported by the same author in different papers, a summary of the general results of 181 patients in the literature, and all cases with SC in the TMJ (including 7 patients in our hospital) is shown in Table 2.
Epidemiologic characteristics, symptoms, imaging findings, treatments, milgram’s stage, and outcomes of all patients with synovial chondromatosis in the TMJ.

B, bilateral; LMO, limited mouth opening; F, female; L, left; M, male; R, right; Sur, surgery; A, arthroscopy; yrs, years.
The main symptoms of SC in the TMJ in our cases and cases from literature were as follows: pain (100%, 7/7; 64.64%, 117/181), limited mouth opening (57.14%, 4/7; 53.59%, 97/181), swelling (14.29%, 1/7; 28.18%, 51/181), crepitus (28.57%, 2/7; 19.34%, 35/181), and click (14.29%, 1/7; 9.94%, 18/181).
The imaging features of TMJ-SC occupying lesions were loose bodies or masses (71.42%, 5/7; 37.57%, 68/181), bone change in condyle or glenoid fossa (1/7, 14.29%; 34.81%, 63/181), effusion (42.86%, 3/7; 20.99%, 38/181), joint space changes (42.86%, 3/7; 11.05%, 20/181) in our cases and cases from the literature, respectively. The reviewed literature described 79 cases of open surgery, 55 cases of arthroscopic surgery, 38 cases of arthroscopy-assisted open surgery, and 1 case of arthroscopic lavatory treatment. The surgical methods were not mentioned in the remaining eight patients. The affected synovium and loose bodies were removed in most cases. Other surgical procedures such as condylar resection, disc resection, and costal cartilage transplantation were performed in some cases. Only one case of postoperative recurrence has been reported in the reviewed literature.
Discussion
The TMJ was thought to be rarely affected by SC. However, the reports about SC in the TMJ have increased in recent years, which may be related to an improved diagnosis rate using CT and MRI, and the improvement of doctors’ cognitive level.9,10 Our cases and literature review followed the epidemiological profile of SC in the TMJ. The mean onset age of our SC cases was 45.14 years, close to 44.62 years reported in the literature. SC in the TMJ occurred more often in women, but SC in the large joints occurred more often in men.11–13 This gender-specific prevalence of SC in TMJ was similar to that of TMD.14,15 This may be related to the effect of estrogen on TMJ, which needs further study. Most SC in the TMJ occurs on one side of the patients. 4 Bilateral diseases have rarely been reported, and only 2 bilateral cases have been reported so far in the literature.16,17 Most reports indicate that SC is usually limited to the upper compartment of the TMJ. We only found 7 cases in three publications from the literature that reported SC in the lower compartment of the TMJ.18,19 The low prevalence rate of SC in the lower compartment of the TMJ might be due to the more narrow joint compartment and smaller area of the synovial membrane.20,21
Preauricular swelling is a clinical symptom of tumor-like conditions such as diffuse tenosynovial giant cell tumor, synovial cysts, and SC.22,23 Other nonspecific symptoms make it difficult to distinguish SC from TMD or osteoarthritis. SC has local invasive behavior, which can lead to bone erosion, involving glenoid fossa, disc, condyle, and even intracranial extension in the later stage. 24 Therefore it is difficult but important to discriminate and treat SC in the early stages.
X-rays, CT, and MRI are important tools for the diagnosis of SC in the TMJ. Joint space change, bone destruction, sclerosis of the condyle and glenoid fossa, and numerous granular calcification shadows can be detected in X-rays and CT.25,26 The loose body is the most valuable diagnostic sign. However, the SC in Milgram’s stage 1 or 2 lacks calcified loose bodies, which provides difficulty in CT or X-ray-based diagnosis, wrong treatment, expansion of lesion, and delay of surgery.6,27–29 MRI images can display uncalcified loose bodies, joint capsules, disc position, effusion, and invasion of adjacent tissues.11,28 T2WI of MRI has an important reference value for the diagnosis of SC in the TMJ, which mainly manifests as a synovial thickening, joint capsule expansion, cartilage nodules, or calcified loose bodies showing low signal intensity scattered in the effusion that present high signal intensity.30,31 MRI could be a reliable diagnostic tool in the diagnosis of SC in the TMJ as its estimated diagnostic accuracy is nearly 96.06%. 32 In case 1 of this study, the CBCT image showed a widened joint cavity space, and one ineffective injection treatment made the clinician aware of the possibility of SC. Then MRI confirmed this as an SC case. Improving the clinician’s ability to meticulously observe the X-ray and CBCT images could help reduce the misdiagnosis of SC in the TMJ. In our patients, the detection rate of occupying lesions was 5/7, higher than 68/181 in the literature, and the probability of effusion was 3/7, higher than 38/181 reported in the literature. This may be related to the fact that all 7 patients got an MRI examination. The low number of patients in our study may also have affected the distribution of results.
The CT and X-ray imaging features of SC of the TMJ in Milgram’s stage 1 are normal or widened joint space. 33 MRI could reveal that the capsule is “dumbbell” dilated, and a moderate signal intensity region in the expanded joint space is present in T2WI. 34 Milgram’s stage 1 SC should be distinguished from synovitis, suppurative arthritis, and synovial cysts. 35 It is difficult to distinguish synovitis from effusion without contrast-enhanced MRI. It takes time from onset to detection of calcified loose bodies by CT. A patient, reported by Guijarro-Martínez R, showed joint cavity widening and effusion on CT and MRI during the first visit. Loose bodies appeared on CT after two years of follow-up. 14 The imaging features of SC of the TMJ without calcification or with poor calcification in Milgram’s stage 2 can be the same as that of stage 1. However, SC in stage 2 can also be accompanied by imaging manifestations such as bone changes of glenoid fossa and condyle. Calcified loose bodies can be detected by CT and X-ray in Milgram’s stage 3 and later Milgram’s stage 2. SC in the TMJ with calcified loose bodies should be distinguished from osteoarthropathy, exfoliative osteoarthritis, chondrosarcoma, and osteosarcoma.6,19,36
When an image is inconclusive, arthroscopic examination helps in the diagnosis by finding specific features of SC, 37 i.e. (1) villous or polypoid nodular protrusions on the hyperplastic synovial membrane; (2) the synovial membrane without metaplasia is a papillary protrusion-like aggregation, with a pink or bright red color as it is rich in capillaries; (3) many different sizes translucent or white color, round, oval, or strip-shaped loose bodies in the articular cavity. In X-ray, CBCT, MRI, and arthroscopy, the surgeon can select the examination methods according to their convenience of acquisition, the difficulty of diagnosis, the trauma caused by the examination, and the acceptance of the technique by the patient.
Surgery is the only effective treatment for TMJ-SC. Treatment options consist of arthroscopy, synovectomy, excision of loose bodies, discectomy, etcetera..36,38 Some scholars recommend arthroscopy in the treatment of SC because it has the advantage of small trauma. 39 Arthroscopy also has a wide field of vision and can detect lesions in the joint cavity that are not easy to find directly. 40 However, arthroscopy is only applicable to cases with loose bodies <3 mm limited to a single compartment.5,41 It has been reported that arthroscopy cannot completely remove the loose bodies and the abnormal synovial membrane, 7 while open surgery can efficiently remove the loose bodies and the abnormal synovial membrane. However, it is difficult to visualize the fossa directly in open surgery, especially the anteromedial part of the fossa. A condyle osteotomy and/or zygomatic arch amputation may be performed to achieve an excellent view of the fossa and complete removal of the lesion. 42 Open surgery combined with arthroscopy for SC in the TMJ has also been mentioned.36,43 The advantage of this technique is the complete elimination of lesions with minimal osteotomy and short surgical time. Since arthroscopy is a mature technique in our clinical setup, it was used in case 2, where it helped to remove the lesion clearly and saved the condylar from amputation.
Some literature recommends that surgical procedures should be selected according to Milgram’s stage of SC.18,24 The synovial tissue should be completely resected in Milgram’s stage 1 cases. The synovial tissue and loose bodies should be cleaned in stage 2. Only loose bodies or masses should be removed in stage 3. This rule was strictly followed in our cases. Synovectomy was performed in cases 1 and 2, only loose bodies or masses resection was performed in cases 3, 4, 5, 6, and 7.
Additional surgical procedures, such as discectomy, costochondral graft, and deep temporal fascial fat flap, are sometimes required, except for removing the loose bodies and abnormal synovium. We tried to correlate Milgram’s staging with procedures of surgical intervention, but the literature did not provide any useful information. It seems that the type of surgical procedure was determined according to the surgeon's experience and the structures of the SC involved.
Although the postoperative recurrence rate of SC is very low, long-term follow-up is necessary to rule out postoperative recurrence. Early recurrence is mostly related to incomplete synovectomy. The possible cause of long-term recurrence could be remaining tiny bone erosions on the condyle or glenoid fossa. The active metaplasia on the tiny bone erosion results in the recurrence of SC. 44 MRI should be performed before and after surgery since MRI is more sensitive to SC diagnosis, and early diagnosis is very important for selecting the appropriate treatment and providing a better prognosis.
Supplemental Material
sj-docx-1-sci-10.1177_00368504221115232 - Supplemental material for Temporomandibular joint synovial chondromatosis: An analysis of 7 cases and literature review
Supplemental material, sj-docx-1-sci-10.1177_00368504221115232 for Temporomandibular joint synovial chondromatosis: An analysis of 7 cases and literature review by Zhiqiang Song, Shanshan Yuan, Junjie Liu, Astrid D. Bakker, Jenneke Klein-Nulend, Janak L. Pathak and Qingbin Zhang in Science Progress
Footnotes
Acknowledgments
The authors thank Zhongcheng Gong for critically revising the manuscript for important intellectual content. This study was supported by 2019 Featured Clinical Technique of Guangzhou (No. 2019TS42) and Guangzhou Health Commission General Project (No. 20191A010067).
Data sharing and data accessibility
The shared data of this study can be obtained by emailing the corresponding authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangzhou Health Commission General Project, 2019 Featured Clinical Technique of Guangzhou, (grant number No. 20191A010067, No. 2019TS42).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.