
Abstract
Introduction:
Eltrombopag, a kind of thrombopoietin (TPO) receptor agonist, plays the role on the megakaryocyte to activate the platelet production and rapidly increase the number of circulating platelets in patients with primary immune thrombocytopenia (ITP). Eltrombopag provides an opportunity for rapid tapering and/or cessation of corticosteroid therapy. However, it is not clear about the platelet response to Eltrombopag in ITP associated with Sjögren's Syndrome(SS).
Methods:
A retrospective research was conducted on the clinical course of three patients, each with ITP secondary to SS, and initially received therapy of corticosteroids or other immunomodulatory. They took this drug for bleeding diseases. Referring to the description, Eltrombopag was prescribed and adjusted with an initial dose of 25 mg daily, then weekly, then monthly according to the monitoring of platelet counts.
Results:
All patients maintained a satisfactory level of platelet counts (>100,000/mm3 for >2 years) following corticosteroid withdrawal. Meanwhile, Eltrombopag was well-tolerated, and there were no adverse effects, such as thrombotic events.
Conclusions:
Eltrombopag is effective and safe for patients with ITP associated with SS during corticosteroid withdrawal. Thus it may be a crucial therapeutic strategy for reducing corticosteroid-related side effects in SS patients with ITP.
Introduction
Sjögren syndrome (SS) is a systemic autoimmune disease characterized by a wide spectrum of clinical manifestations and autoantibodies. Immune thrombocytopenia (ITP) is a common clinical manifestation of SS that raises the risk of hemorrhagic events. 1 The mechanism of ITP in SS is due to auto-antibody-mediated peripheral platelet destruction and splenic sequestration, as well as declining platelet production due to autoantibodies targeted against megakaryocytes. 2
Corticosteroids supplemented with immunoglobulin are the first-line treatments for SS-related ITP, 3 but long-term remission is rare, and the relapse rates are as high as 70–80%. 4 Moreover, the most recurrent patients were insufficiently sensitive to high doses of glucocorticoids. 4 Second-line therapies contain danazol, Cyclosporin A, azathioprine, and rituximab, ultimately splenectomy. 5 Despite multimodality therapy, about 12–15% of patients still do not respond to therapy. 6 Eltrombopag is non-peptide thrombopoietin (TPO) receptor agonist, which is suggested for the second-line treatment of ITP.5,6 Eltrombopag selectively unites to the transmembrane region of the TPO receptor and triggers megakaryocytopoiesis through the Janus kinase/signal transducer and activator of transcription (JAK/STAT) signaling pathway. 7
While no clinical trials focus on the efficacy or safety of these drugs in patients with secondary ITP relevant to SS, limited case reports and case series have displayed promising results in patients with SLE or APS secondary ITP,8–10 which occurred via similar pathogenesis. Hence, more data are required to inform clinicians whether patients with SS benefit from Eltrombopag. Here we present three cases of Eltrombopag used in patients with SS at the first affiliated hospital of Zhejiang Chinese Medical University from 2017 to 2021.
Case reports
Case 1
A 48-year-old female presented to our clinic with dryness of mouth and eyes for two weeks. She was diagnosed with thrombocytopenia (platelet count was less than 10,000/mm3) without bleeding in a regular physical check-up in July 2017. At that moment, the bone marrow examination was tested, and the result met ITP criteria. 2 She received the standardized treatment(Dexamethasone and IVIg) referred to the ITP guideline. After discharge, her platelet count was stable with prednisone 60 mg every day, and the dose was gradually reduced until withdrawal in September 2017. In December 2017, her thrombocytopenia recurred after catching a cold, and the platelet count was 5000/mm3. But this time, she was no longer sensitive to the same treatment, and her platelet count never exceeded 30,000/mm3. Three weeks before this visit, she developed dry mouth and eyes, and the serum tests revealed positive Antinuclear and anti-SSA antibodies, but negative anti-platelet antibodies. Biopsy of the low labial gland indicated focal lymphocytic sialadenitis, which fulfilled ACR SS criteria. 11 The current bone marrow tests showed obvious active proliferation of nucleated cells and decreased megakaryocytes. Treatment with Methylprednisolone (MP) 500 mg/day for three days and IVIg 0.4 g/kg/day for five days was initiated, then MP was decreased to 80 mg/day and Cyclosporin A (CsA) 5 mg/kg/day followed. However, her thrombocytopenia did not improve, and the platelet count climbed hardly from 27,000/mm3 to 43,000/mm3. After discharge, she continued the therapy with MP 40 mg/day and CsA 150 mg/day for three months, and the platelet count fluctuated around 30,000/mm3. On 18th April 2018, the patient began taking eltrombopag 25 mg daily, and two weeks later, the platelet count was 168,000/mm3. On 10th May 2018, with the cessation of MP and CsA, the platelet count was kept at 220,000/mm3 another two weeks later. Then the platelet count was maintained at about 200,000/mm3 for six months. Finally, eltrombopag was discontinued in January 2019, but the platelet count kept normal until now.
Case 2
A 57-year-old female with a four-year history of SS-related interstitial pneumonia (SS-ILD) presented with severe thrombocytopenia and purpura for four days. She was first diagnosed with SS-ILD in 2017 when she developed a dry mouth and eyes with short breath after activities. CT revealed interstitial changes in both lungs. Antinuclear and anti-SSA antibodies were both positive, and the labial salivary gland biopsy met focal lymphocytic sialadenitis, which fulfilled ACR SS criteria. 11 She received MP, with a considerable response of the sicca symptoms and interstitial pneumonia. Three months later, she discontinued the treatment due to obesity that was related to the glucocorticoids. Fortunately, she kept healthy for the second year. In 2018, She caught a cold, and the blood routine examination conducted in the community hospital indicated the platelet count was 22,000/mm3. At that moment, there was no skin petechiae, ecchymosis, gingival bleeding, etc., so she paid no attention to it. But one month later, a repeated examination of the blood routine showed thrombocytopenia as before, about 20,000/mm3. Without sicca manifestations of SS, but the CT scanning still revealed interstitial pneumonia similar to 2017, her antiplatelet antibodies test was negative, and the bone marrow test showed the proliferation of nucleated cells was active, and megakaryocyte proliferation increased obviously (Figure 1). She received the therapy of dexamethasone 40 mg/day and IVIg 0.4 g/kg/day for five days, her platelet count increased to 143,000/mm3, and she received prednisone 50 mg daily for maintenance. Subsequently, the dose of prednisone was reduced at a rate of 10% per week to 5 mg daily. One month later, the patient's platelets redescended to 12,000/mm3. Since her bone mineral density examination suggested osteoporosis related to corticosteroids during the period, she rejected the therapy of glucocorticoids. Therefore, she was prescribed eltrombopag 25 mg oral daily in December 2018, and a half month later, her platelet count climbed to 148,000/mm3 rapidly. Then, Eltrombopag was gradually reduced to 25 mg every other day, then twice a week, then once a week, then once every other week, and was withheld in June 2019. Her platelet count on 15th May 2021 was 221,000/mm3.
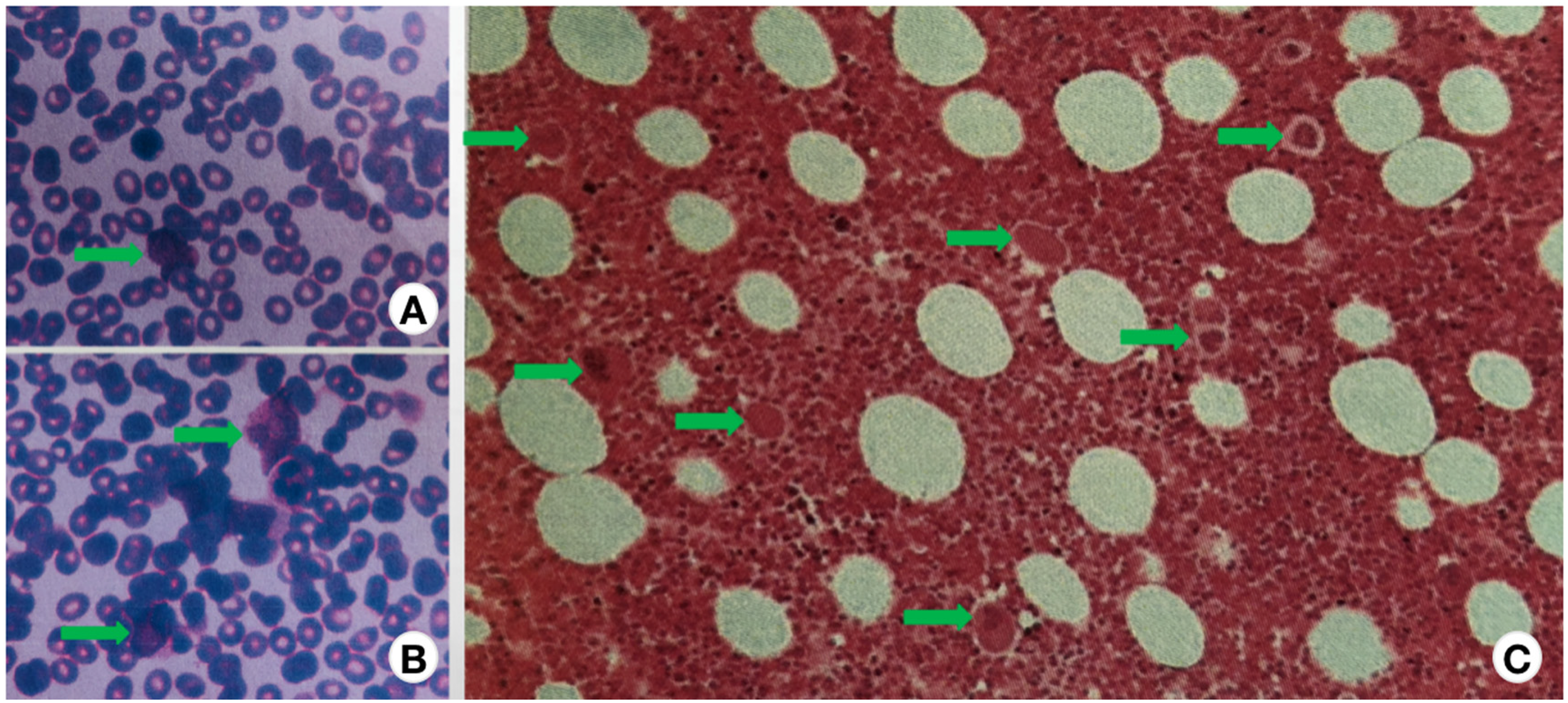
Bone marrow revealing that the proliferation of nucleated cells was active, and megakaryocyte proliferation increased obviously (A, B: bone marrow morphology. C: Bone marrow biopsy histopathology. The green arrows point to megakaryocytes.).
Case 3
A 50-year-old female with a history of SS complained about severe thrombocytopenia and purpura. She was first diagnosed with SS in 2014 when she developed mouth and eye dryness. Antinuclear and anti-SSA antibodies were both positive, and the labial salivary gland biopsy showed the number of mononuclear-cell infiltrates containing more than 50 inflammatory cells per 4 mm2, which fulfilled ACR SS criteria. 11 She received hydroxychloroquine, with a favorable response to the sicca symptoms. In 2018, she presented with thrombocytopenia (a platelet count of 4000/mm3), at the moment, she has no other symptoms of SS, her serum antiplatelet antibodies were negative, her bone marrow test showed disorders of megakaryocyte maturation, and the number of platelet-producing megakaryocytes was significantly reduced (Figure 2), which met ITP criteria. 2 Her condition improved with IVIg 0.4 g/kg/day for 5 days, MP 40 mg/day and CsA 5 mg/kg/day. From the end of 2018 to the beginning of 2019, the platelet count remained about 34,000/mm3. In March 2019, her ITP recurred with a platelet count of 12,000/mm3, and she received methylprednisolone, IVIg, and cyclophosphamide 0.8 g/month repeatedly. After three months the platelet count ascended to 50,000/mm3. During the reduction of methylprednisolone, her platelet count declined again. Considering the side effects of MP, such as hypertension, diabetes, osteoporosis, and Cushing's syndrome, she rejected the therapy with a high dose of corticosteroids. Then, she was started on eltrombopag 25 mg PO daily in April 2019, and three weeks later, her platelet count climbed to 67,000/mm3, then Eltrombopag was withheld, but two weeks later, her platelet count descended to 26,000/mm3. Eltrombopag was restarted at 25 mg daily, and a week later, her platelet count rose to 74,000/mm3. Then, the eltrombopag was gradually reduced to 25 mg every other day, then twice a week, then once a week, then once every other week, and was finally omitted altogether in March 2020. Her platelet count on 23rd July 2021 was 102,000/mm3.

Bone marrow biopsy histopathology revealing that the number of platelet-producing megakaryocytes was significantly reduced (A: The black arrows point to megakaryocytes. B: The red arrow point to megakaryocytes.).
Results
Three female patients with refractory SS-ITP were enrolled in our study. Severe thrombocytopenia was the presenting manifestation of the protopathy. They all had poor responses to a high dose of corticosteroids and immunosuppressive treatment. The patients’ platelet levels gradually increased to the normal range with eltrombopag, which was gradually reduced and finally omitted. Here we present the results of platelet counts at particular and critical time points during ITP therapy (Figure 3). All three patients maintained a satisfactory result of platelet counts (>100,000/mm3 for >2 years) following corticosteroid withdrawal or other immunosuppressants. Eltrombopag was well-tolerated, and there were no adverse effects, such as thrombotic events.

Schematic diagram of platelet counts measured at particular, critical time points during ITP therapy: time point 1: baseline value; time point 2: Maximum value while on 1st-line therapy; time point 3: Maximum value while on repeated 1st-line treatment after relapse (case 3 showed insensitivity); time point 4: Minimum value before treatment of eltrombopag; time point 5: Maximum value after 25 mg of eltrombopag once-daily initiation; time point 6: value on eltrombopag withdrawal.
Discussion
In this retrospective study, eltrombopag manifested a satisfactory therapeutic outcome in pretreated refractory adult ITP patients related to SS. Despite the poor quality of evidence, our research results support the use of low dosage eltrombopag as an excellent choice after first-line treatment failed. It seems a very ideal strategy for the effective maintenance of response, improving health-related quality of life, and lowering both costs and side effects of the drugs. Meanwhile, it possibly enhances the safety of the therapy of ITP. A retrospective multicenter study conducted in 17 centers affiliated with the Italian Association of Pediatric Hematology and Oncology (AIEOP) also highlighted the crucial role of eltrombopag in children with chronic ITP. 12
Despite the excessive therapeutic strategies in ITP, there is no sufficient evidence to guide a principle of treatment for refractory ITP cases. Those platelet counts do not respond to ≥2 treatments. 13 Recently, eltrombopag was established as an effective second-line therapy for chronic ITP 5 and used in primary ITP and thrombocytopenia secondary to connective tissue diseases (CTD), such as lupus, APS, Wiskott-Aldrich syndrome, and SS. However, limited data appear, especially SS.
In the present case series, we present three SS secondary refractory ITP patients with different bone marrow manifestations who achieved long-term clinical remission while taking eltrombopag at a low dose of 25 mg daily initiated, then reduced gradually and withdrawn. No extra corticosteroids or immunosuppressive were required. Our study results revealed that decreasing eltrombopag dosage is effective for retaining the normal range of platelet counts.
Another interesting finding is that eltrombopag was effective regardless of whether the results of bone marrow examination suggested an increase or decrease in megakaryocytes. In cases 1 and 3, the patients’ bone marrow showed the number of megakaryocytes with platelet production was significantly reduced, and the other patient's bone marrow indicated the megakaryocyte proliferation increased obviously. Indeed, the commonality among the three cases is that they all had a poor response to a high dose of corticosteroids and immunosuppressive treatment, and positive anti-SSA Ab and negative anti-PA Ab. Theoretically, as a TPO receptor agonist, eltrombopag should be more effective for the patients by reducing platelet-producing megakaryocytes in the bone marrow biopsy. However, it is also effective in patients with active megakaryocyte proliferation. The possible mechanism is that eltrombopag can bind to the transmembrane domain of the TPO surface receptor on the megakaryocyte, which triggers intracellular MAP kinase and JAK-STAT signaling pathways contributing to maturation and differentiation of megakaryocyte, and ultimately to an improvement in platelet production. 7 Consequently, circulating platelet counts in patients with ITP increase, allowing for speedy corticosteroid withdrawal.
As for the phenomenon that patients' platelets still maintained an ideal level after drug withdrawal, we speculated that the mechanism of SS secondary ITP is a transient platelet production dysfunction of bone marrow megakaryocytes caused by the low function of TPO receptors. With the treatment of eltrombopag, TPO receptors were activated and not suppressed again for a period. The specific mechanism needs us to research in the future.
Footnotes
Author contribution
The cases were diagnosed and followed up by XLP, ZY, and LN. SXW and DQD conceived and planned the case reports. Article collection was performed by XLP. Data collection and analysis were performed by ZY and LN. XLP and ZY wrote the initial manuscript with help from SXW and DQD. The final version was read, corrected, and approved by all the authors.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Traditional Chinese Medical Science and Technology Project of Zhejiang Province (Grant No. 2022ZB130), and the National Famous Old Chinese Medicine Experts SONG Xinwei Inheritance Studio Project (G.TCM.R.J.H.[2018]134).
Ethics approval
The case report was approved and supervised by the ethics committee of The First Affiliated Hospital of Zhejiang Chinese Medical University.
Author biographies
Liping Xu, MD of TCM, is an attending physician of Rheumatology and Immunology Department in the First Affiliated Hospital of Zhejiang Chinese Medical University.
Yan Zhang, MD, is an attending physician of Rheumatology and Immunology Department in the First Affiliated Hospital of Zhejiang Chinese Medical University.
Na Lin, MM, is an attending physician of Rheumatology and Immunology Department in the First Affiliated Hospital of Zhejiang Chinese Medical University.
Xinwei Song is a professor of TCM, the National Famous Old Chinese Medicine Expert, and the chief physician of Rheumatology and Immunology Department in the First Affiliated Hospital of Zhejiang Chinese Medical University.
Qiaoding Dai, MD, is a deputy professor and the associate chief physician of Rheumatology and Immunology Department in the First Affiliated Hospital of Zhejiang Chinese Medical University.