
Abstract
Objective
The COVID-19 pandemic has impacted various health conditions. Emerging evidence suggests that COVID-19 may trigger or exacerbate oral and maxillofacial conditions, yet data from Iraq and the broader Middle East remain limited. This retrospective cohort study, conducted at the Laboratory of Oral Pathology, College of Dentistry, University of Baghdad, explores potential links between COVID-19 infection and maxillofacial disorders.
Methods
This was a retrospective cohort study using data from the Laboratory of Oral Pathology, College of Dentistry, University of Baghdad. Cases were divided into pre-COVID-19 and post-COVID-19 periods. Chi-square tests assessed differences in oral pathologies incidence, while logistic regression analyzed associations with COVID-19 status and corticosteroid use.
Results
Mucormycosis cases demonstrated a significant increase from 3 (pre-COVID-19) to 23 (post-COVID-19), with 65.22% of post-COVID-19 patients testing COVID-19-positive. A significant increase in mucormycosis severity was observed after COVID-19 (χ² = 14.24, p = 0.0026). Logistic regression identified age (coefficient 0.8738) as having a significant association with severe mucormycosis, while COVID-19 status (coefficient 0.1272) exerted a lesser effect. Sjögren's syndrome increased from 15 to 25 cases, with a model area under the curve of 0.8, indicating substantial ability to distinguish symptom changes pre- vs. post-COVID-19.
Conclusion
The findings suggest that the pandemic has considerably impacted the incidence and severity of mucormycosis and Sjögren's syndrome. Older age and COVID-19 positivity may be key drivers of severe mucormycosis, whereas COVID-19 infection appeared to exacerbate Sjögren's syndrome symptoms. These results underscore the importance of vigilant monitoring and targeted therapeutic strategies for managing oral and maxillofacial conditions during and after viral pandemics.
Introduction
Several viruses are widely recognized as key contributing factors for human diseases. Viruses like Hepatitis B and C, Epstein-Barr Virus (EBV), and Human Herpes Virus 8 are known for their oncogenic potential 1 while EBV, for instance, is linked to autoimmune disorders like rheumatoid arthritis, systemic lupus erythematosus, and Sjogren's syndrome. 2
With the advent of COVID-19, studies proliferated on its long-term complications. Previous SARS-CoV-2 infections have been linked to increased risks of conditions such as type 1 diabetes mellitus, systemic sclerosis, Sjogren's syndrome, Behcet's disease, immune dysfunction, and systemic lupus erythematosus.3,4
Several hypotheses regarding the role of COVID-19 in immune system dysregulation have been proposed, including molecular mimicry, organ involvement through widespread receptor expression, bystander lymphocyte activation, superantigen effects, epitope spreading, and the release of autoantigens from injured tissues. 5 Additionally, Post-vaccination complications also emerged, encompassing thrombotic events, autoimmune conditions, Guillain-Barre syndrome, IgA nephropathy, and inflammatory arthritis. 6
Oral complications related to COVID-19, such as petechiae, ulcers, geographic tongue, plaque-like lesions, gustatory dysfunction, and herpes simplex reactivation have been reported.7,8 Among the oral complications reported after SARS-CoV-2, mucormycosis has gained recognition as a serious and potentially life-threatening condition. Studies have shown that the combination of SARS-CoV-2 infection, underlying comorbidities such as diabetes mellitus, and corticosteroid treatment create a favorable environment for the development of this opportunistic fungal infection.9–11 While mucormycosis has been mostly reported as a systemic disease involving the rhino-orbital and pulmonary areas, the involvement of the maxillofacial area is also common. Despite the decline in acute COVID-19 cases, long-COVID and post-infection sequelae, including potential immunological consequences, remain highly relevant in global healthcare. Further investigation into the long-term impact of SARS-CoV-2 on the incidence and presentation of various conditions is still necessary.
Despite the global recognition of the importance of mucormycosis as a complication of SARS-CoV-2, there is a lack of specific epidemiological data from Iraq and the broader Middle East. Furthermore, the study is novel due to the comparison of data from pre- and post-pandemic periods, providing a clearer understanding of the changes in incidence of mucormycosis, Sjogren's syndrome, and tuberculous lymphadenitis in the setting of an oral pathology referral clinic. Previous studies have often presented individual cases or series. Our study, however, seeks to quantify the impact of the pandemic on the incidence of maxillofacial mucormycosis in this specific geographic location and within an oral pathology setting.
Materials and methods
Study design and Setting
This retrospective cohort study was conducted at the Laboratory of Oral Pathology, College of Dentistry, University of Baghdad. Data were collected from patient records referred from two major maxillofacial centers in Iraq, selected to represent a comprehensive demographic cross-section and mitigate statistical biases. The study period extended from January 2018 to December 2023, segmented into pre-COVID-19 (January 2018 to 23 February 2020) and post-COVID-19 (January 2021 to December 2023) phases to examine the impact of the pandemic on the incidence of oral and maxillofacial lesions. Based on the first documented case of COVID-19 in Iraq, reported in Najaf on 24 February. 12 The pre-COVID period for this study was January 2018 to 23 February 2020. While the first reported case may have been earlier, this was the first documented case that was accurately recorded and confirmed. The period from March 2020 to December 2020 was excluded due to disruptions caused by the initial COVID-19 outbreak and subsequent healthcare limitations, including lockdowns and the peak of the first infection wave. The post-COVID-19 period was defined as January 2021 to December 2023 to allow sufficient time for the potential manifestation of post-COVID complications, including those related to immune system dysregulation and inflammatory processes, which may emerge after the initial peak of infections.
Inclusion and exclusion criteria
This retrospective cohort study included all patients referred to the Laboratory of Oral Pathology at the College of Dentistry, University of Baghdad, between January 2018 and December 2023 who presented with suspected oral and maxillofacial lesions requiring histopathological examination. Only individuals with a confirmed histopathological diagnosis and complete medical records were eligible. Participants were excluded if they lacked sufficient clinical or pathological data to confirm a final diagnosis. All patients meeting these criteria were entered into the study without further selection, ensuring that the sample accurately reflected the types of lesions encountered in routine practice. This is considered a consecutive sampling method.
Range of lesions studied
The cases documented during this period included a range of benign and malignant lesions across epithelial, odontogenic, salivary gland, connective tissue, and bone origins, related to inflammatory, infectious, developmental, physical or chemical injuries, and autoimmune diseases.
Study outcomes
The primary outcomes of this study were the changes in incidence of mucormycosis, Sjogren's syndrome, and tuberculous lymphadenitis in the pre- and post-COVID periods. The secondary outcomes were severity of mucormycosis, exacerbation of Sjogren's syndrome symptoms, and their association with age and COVID-19 status. Participants were assigned to the pre-COVID-19 group if their histopathological diagnosis was before 23 February 2020, and to the post-COVID-19 group if their histopathological diagnosis was after 1 January 2021. Cases in the post-COVID-19 group were further classified as COVID-19 positive or negative based on their test results (PCR and/or serology).
Variables and definitions
The primary exposures in this study were confirmed COVID-19 infection (positive/negative PCR or serology test) and corticosteroid use (yes/no; and if related to COVID-19 treatment). The primary outcomes were changes in the incidence of mucormycosis, Sjogren's syndrome (defined by new-onset or exacerbation of symptoms), and tuberculous lymphadenitis. The secondary outcomes included the severity of mucormycosis and the exacerbation of Sjogren's syndrome symptoms, both of which were analyzed in association with age and COVID-19 status. Potential confounders included age, gender, and the presence of comorbidities (such as diabetes). The main effect modifiers explored were age and COVID-19 status. The primary source of data was the pathology records, which included clinical and histopathological data. Telephone interviews were conducted to fill in any missing information. The questionnaire used in the telephone interviews is available from the authors upon request. Diagnoses of mucormycosis, Sjogren's syndrome, and tuberculous lymphadenitis were based on established clinicopathological criteria following analysis of histopathology. Detailed clinicopathological criteria for the diagnosis of mucormycosis are provided in
Data collection
To study any significant differences in the incidence of oral pathologies pre- and post-COVID-19, patient records were used as the primary source of data. These records encompassed comprehensive clinical documentation, including COVID-19 infection status, hospitalization records, and treatments, with a focus on immunomodulatory drugs such as corticosteroids. These records were supplemented by structured telephone interviews to confirm and elaborate on clinical data, especially in cases where documentation in medical records was unclear or incomplete. Data extraction from medical records was performed by BH and OM, and the telephone interviews were conducted by NA and FI. The Data collection form is provided in
Data verification and validation
To ensure the accuracy of the data:
Handling missing data
Recognizing the potential impact of missing data on the study's outcomes:
Statistical analysis
The statistical approach included:
Ethical considerations
The study protocol was approved by the Institutional Review Board at the University of Baghdad, Baghdad, Iraq (reference number 936724) on 29/8/2024. All procedures adhered to the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975 as revised in 2013. All patient identifying information was removed, and only de-identified data were used for analysis. Given that this study was a retrospective analysis of existing patient records, obtaining signed consent was not required by the Institutional Review Board. Measures were implemented to ensure patient anonymity and data confidentiality in compliance with data protection laws. Data access was restricted to authorized personnel involved in the study. This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cohort studies. 13
Results
The study analyzed 812 cases prior to the COVID-19 pandemic and 694 cases following its onset. The majority of oral and maxillofacial disorders did not show any significant changes in diagnosis rates before and after the emergence of COVID-19. However, there was a notable increase in the incidence of mucormycosis, Sjogren's syndrome, and a drop in the cases of tuberculous lymphadenitis.
Mucormycosis
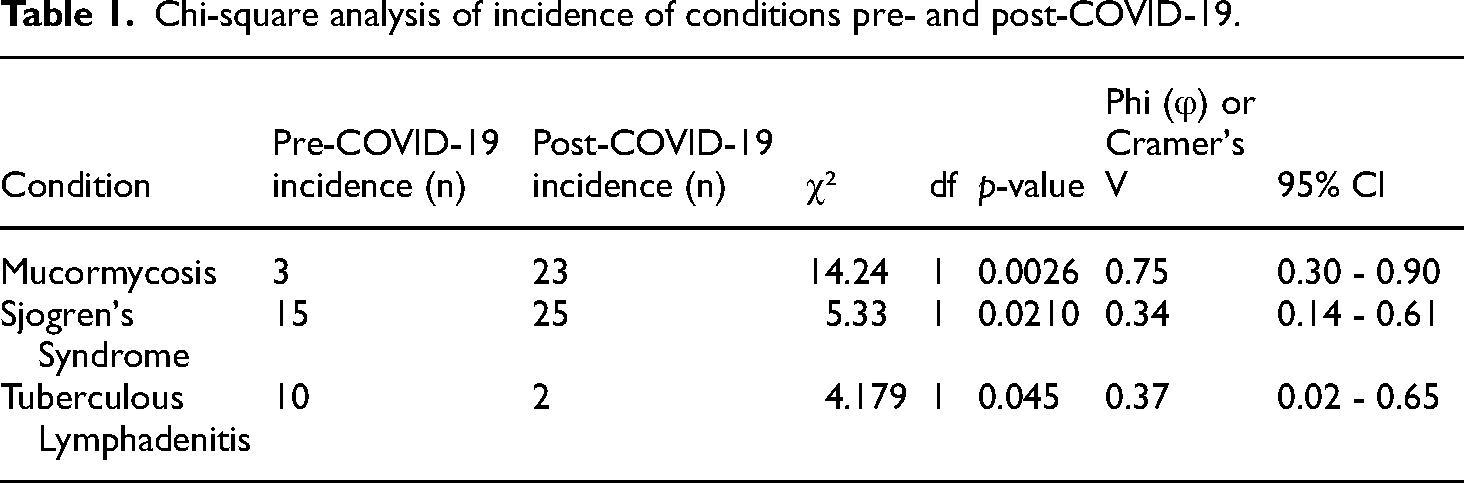
The cohort included 26 cases with an age range from 33 to 80 years (mean age 57.1 years). Three cases before COVID-19 and 23 post-COVID-19, the majority of post-COVID-19 mucormycosis cases were associated with COVID-19 infections, with 21 cases testing positive (Figure 1). A Chi-square test showed a significant increase in mucormycosis cases post-COVID-19 (χ² = 14.24, df = 1, p = 0.0026, φ = 0.75, 95% CI 0.30 - 0.90) (Table 1). The prevalence of diabetes was high, with 18 out of 26 patients (69%) reporting this comorbidity. A significant correlation was found between cortisone use and severity of mucormycosis (r = 0.77, p < 0.05). Age was positively correlated with severity, where older patients tended to present with more severe forms of infection.

Incidence of mucormycosis and Sjogren's syndrome pre- and post-COVID-19.
Chi-square analysis of incidence of conditions pre- and post-COVID-19.
A Chi-square test was performed to detect significant differences in the severity of mucormycosis between pre- and post-COVID-19 periods. The results indicated a statistically significant difference in the severity distribution (Chi-square = 14.24, p = 0.0026), suggesting that the emergence of COVID-19 has impacted the severity of mucormycosis cases (Figure 2).

Distribution of mucormycosis severity relative to COVID-19 history.
A logistic regression analysis with L1 regularization (Lasso) was conducted to determine the association between COVID-19 status and mucormycosis severity after controlling for age. The model coefficients were as follows: Age 0.8738, COVID result positive 0.1272.
The intercept was −0.7435. These results indicate that an increase in age is significantly associated with a higher likelihood of severe mucormycosis. While COVID-19 status shows a positive association with mucormycosis severity, the strength of this association is less pronounced than that of age (Figure 3).

Logistic regression coefficients for severe mucormycosis.
Sjogren's syndrome
The Chi-square results for Sjogren's syndrome showed a significant increase in the incidence of the condition post-COVID-19 (χ² = 5.33, df = 1, p = 0.0210, φ = 0.34, 95% CI 0.14 - 0.61) (Table 1). The incidence of Sjogren's syndrome increased from 15 cases pre-COVID-19 to 25 cases post-COVID-19 (Figure 1) with an age range from 23 to 73 years, with a median age of 45.5 years, manifesting predominantly among middle-aged individuals. The cohort was largely composed of females, accounting for 91.67% of the total. Regarding COVID-19 impact, 61.1% of participants tested positive for the virus. Notably, there were no hospitalizations reported among the participants. Steroid treatment for Covid-19 was administered to 13.8% of the patients; 47.2% did not receive steroids, and for 38.8% of the cases, the steroid treatment data was unavailable or unchanged.
The study closely monitored changes in Sjogren's syndrome symptoms post-COVID-19 infection. A total of 25% of the patients experienced new-onset symptoms, 16.6% reported an exacerbation of existing symptoms, and an additional 8.3% noted varied changes in symptom severity.
A logistic regression model was employed to examine the relationship between COVID-19 infection and the exacerbation of Sjogren's syndrome symptoms, adjusting for potential confounders such as age and sex. The model's effectiveness was evaluated using a receiver operating characteristic curve, achieving an area under the curve (AUC) of 0.8, demonstrating substantial discriminative ability to differentiate between symptom changes pre- and post-COVID-19 infection.
The model exhibited a precision of 78% and a recall of 88% in identifying post-COVID-19 cases. However, it faced challenges in accurately classifying pre-COVID-19 cases, particularly those with less pronounced symptom changes. Cross-validation techniques were utilized to confirm the model's consistency and robustness, consistently achieving an average AUC of 0.8 across various folds. The optimized model incorporated an L2 penalty with a regularization strength (C) of 1, effectively minimizing overfitting and enhancing the generalizability of the model's findings (Figure 4).

ROC curve for Sjogren's syndrome model. ROC: receiver operating characteristic.
The analysis highlights a significant increase in the severity of mucormycosis post-COVID-19, with age being a key predictor of severe outcomes. Additionally, there was a notable increase in Sjogren's syndrome cases, with logistic regression indicating substantial discriminative ability in identifying post-COVID-19 symptom changes.
Tuberculous lymphadenitis
In contrast to what was observed with Mucormycosis and Sjogren syndrome, the Chi-square test showed a significant decrease in the incidence of tuberculous lymphadenitis post-COVID-19 (χ² = 4.179, df = 1, p = 0.045, φ = 0.37, 95% CI 0.02 - 0.65) (Table 1); suggesting that the lockdown, masking, and other hygiene precautions contributed to a drop in the transmission of tuberculous infections.
Discussion
The COVID-19 pandemic that originated from Wuhan, China has had far-reaching effects on various aspects of human health. This study aimed to assess the impact of COVID-19 on the incidence and severity of oral and maxillofacial disorders and to investigate potential causal links with COVID-19 infection.
Our findings revealed a significant increase in the incidence of mucormycosis and Sjogren's syndrome post-COVID-19. The Chi-square test indicated a statistically significant difference in the severity distribution of mucormycosis between pre- and post-COVID-19 periods (Chi-square = 14.24, p = 0.0026). One case series from Iraq reported 16 cases of maxillofacial mucormycosis infections over a period of 10 years (Museedi et al. 2022). Notably, this number is smaller than the 23 cases that emerged over the relatively shorter period following the COVID-19 outbreak. This aligns with previous studies that have reported a surge in oral and jaw mucormycosis cases associated with COVID-19, particularly in patients with comorbidities such as diabetes and those treated with corticosteroids.10,14–16
The logistic regression analysis with L1 regularization identified age as a significant predictor of mucormycosis severity, with a coefficient of 0.8738. Although COVID-19 status showed a positive association with mucormycosis severity, its coefficient (0.1272) suggests a less pronounced effect compared to age. This may indicate that while COVID-19 infection is associated with an increased risk of mucormycosis, other factors such as age and comorbidities play a more critical role in determining the severity of the disease.
The increase in Sjogren's syndrome cases post-COVID-19 is also noteworthy. The logistic regression model achieved an AUC of 0.8, demonstrating substantial discriminative ability in differentiating between symptom changes pre- and post-COVID-19 infection. This finding is consistent with reports of autoimmune and inflammatory conditions being triggered or exacerbated by COVID-19.17–19 The precise mechanisms underlying these associations remain unclear, but it is hypothesized that viral infections can trigger autoimmunity through molecular mimicry, bystander activation, and other immune-mediated processes. 20 These findings underscore the critical need for targeted monitoring and therapeutic strategies during and following pandemics.
The mechanisms by which COVID-19 may influence the incidence and severity of mucormycosis and Sjögren's syndrome are complex, multifactorial, and may occur due to post-infection or post-vaccination immune dysregulation. One possibility is molecular mimicry, in which viral antigens may resemble self-antigens, triggering an autoimmune response.17,21 Furthermore, bystander activation, in which the inflammatory environment caused by the virus activates self-reactive lymphocytes, 22 and the cytokine storm, characterized by a surge of pro-inflammatory cytokines, can also play a role in the development or worsening of autoimmune conditions. 23
Autoantibody production, in which viral infections lead to the production of autoantibodies that target self-tissues, has also been described, with evidence of new-onset autoantibodies persisting for at least 12 months post-infection. 20 Although vaccination is crucial to prevent infection, it may also elicit an inflammatory reaction that may exacerbate pre-existing conditions, as observed in studies of post-vaccination autoantibody dynamics.24,25 Further research is necessary to determine the precise mechanisms involved in this complex process, particularly the role of SARS-CoV-2 in triggering autoimmune phenotypes such as Sjögren's syndrome and the interplay between immune dysregulation and secondary infections like mucormycosis17,20
Several factors related to aging may increase susceptibility to fungal infections such as mucormycosis. Immunosenescence, which refers to the age-related decline in immune function, particularly in cell-mediated immunity, is a significant factor. 26 Furthermore, older individuals are more likely to have comorbidities such as diabetes, a known risk factor for mucormycosis. 27 Polypharmacy, a common issue among older adults, can also impair the immune response, further increasing the risk of infections. 28
Age has been shown to be a risk factor for severe COVID-19, which may also be related to dysregulation of the immune system, leading to an increased risk of opportunistic fungal infections. 29 Although vaccination helps prevent severe disease, it may elicit an inflammatory response, particularly in older adults, which may also play a role in the development of mucormycosis. 30 Therefore, older individuals with comorbidities and taking multiple medications are particularly vulnerable to fungal infections such as mucormycosis during and after the COVID-19 pandemic.
Our findings regarding the increase in mucormycosis cases are consistent with reports from India, where a substantial rise in this opportunistic infection was observed during the COVID-19 pandemic, frequently related to increased use of corticosteroids and diabetes prevalence 31 Conversely, in European countries, while mucormycosis cases have been reported, the incidence was lower than what was seen in India or this region. 32 Similarly, the finding that COVID-19 infection may exacerbate the symptoms of Sjögren's syndrome is consistent with a previous study done in Brazil; however, more research is needed to understand these regional variations. 19
The drop in the incidence of tuberculous lymphadenitis is consistent with a previous study that reported a lower number of tuberculous infections during the pandemic. This drop is probably linked to decreased transmission of Mycobacterium tuberculosis due to masking and social distancing but it could also be related to underreporting of tuberculosis cases during the pandemic.33,34 The small number of cases in our study, however, precluded robust statistical analyses; therefore, logistic regression analysis was not performed for cases of tuberculous lymphadenitis.
While we adjusted for several potential confounders in our regression models, we acknowledge that we did not perform formal subgroup analyses to explore potential interactions between COVID-19 status and other factors (e.g. diabetes, corticosteroid use) on the risk of mucormycosis and Sjögren's syndrome. This was primarily due to limited sample sizes within certain subgroups, which would have reduced the statistical power of these analyses. Future research with larger cohorts is needed to investigate these potential interactions.
This study has several limitations. The study is limited by several factors inherent to a retrospective design. The retrospective design and reliance on medical records and telephone interviews may introduce recall bias and inaccuracies in data collection. The exclusion of the period from March 2020 to December 2020 due to healthcare disruptions may also affect the comprehensiveness of the analysis, and potentially underestimate the cases during that period. As we used pathology records as the primary data source, any condition that was not subjected to a biopsy procedure was not included in this analysis. Additionally, the small sample size for certain subgroups, such as pre-COVID-19 mucormycosis cases, may limit the generalizability of our findings. Furthermore, the results were not validated on another cohort, which would be ideal for further validation of the study findings. The study confirms the association between COVID-19 and the increased incidence of mucormycosis reported by previous studies in various locations; however, our findings are novel as we provide a specific view of the association between COVID-19 and mucormycosis in an Iraqi population, using a comprehensive epidemiological approach in an oral pathology setting, with data that compares pre- and post-pandemic periods. Moreover, while some reports have suggested a possible association between COVID-19 and Sjogren's Syndrome, we showed robust statistical results using logistic regression, that demonstrate a clear link between the infection and the worsening of Sjogren's symptoms. Finally, the decreased cases of tuberculous lymphadenitis, while not the main focus of the study, are an important novel finding of the study, with implications for the role of infection control and social distancing measures in the transmission of infectious diseases. The combination of all these three diseases, in one study is also a novel aspect of the research. Potential confounding by including age, gender and known comorbidities as covariates in our logistic regression models, which aimed to control for their effect in our analysis.
Taking our observations into account, our suggestion is that oral healthcare providers pay close attention to oral and maxillofacial involvement during pandemics. Viral infections may involve maxillofacial tissues directly or indirectly by causing immune dysregulation. Additionally, vaccinations may be related to a rise in autoimmune conditions while corticosteroid treatment may cause immune dysregulation and increase the risk of fungal infections. Oral healthcare providers may also need to educate the patients about the possibility of oral involvement and the potential risks associated with vaccination, treatment, and the presence of comorbidities.
Conclusion
In conclusion, the COVID-19 pandemic may have significantly impacted the incidence and severity of certain oral and maxillofacial disorders. This study highlights a notable rise in mucormycosis and Sjogren's syndrome cases post-COVID-19 in Baghdad Iraq. Age and COVID-19 status may be significant predictors of mucormycosis severity, while COVID-19 infection was associated with exacerbations of Sjogren's syndrome symptoms. These findings underscore the importance of vigilant monitoring and targeted therapeutic strategies for managing oral and maxillofacial conditions during and after any viral pandemic. Further research is needed to understand the mechanisms linking COVID-19 to these disorders and to develop effective preventive and treatment protocols.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251326453 - Supplemental material for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study
Supplemental material, sj-docx-1-sci-10.1177_00368504251326453 for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study by Bashar Abdullah, Omar Museedi, Noor Allawi, Fatimah J. Ismael and Saman Warnakulasuriya in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504251326453 - Supplemental material for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study
Supplemental material, sj-docx-2-sci-10.1177_00368504251326453 for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study by Bashar Abdullah, Omar Museedi, Noor Allawi, Fatimah J. Ismael and Saman Warnakulasuriya in Science Progress
Supplemental Material
sj-docx-3-sci-10.1177_00368504251326453 - Supplemental material for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study
Supplemental material, sj-docx-3-sci-10.1177_00368504251326453 for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study by Bashar Abdullah, Omar Museedi, Noor Allawi, Fatimah J. Ismael and Saman Warnakulasuriya in Science Progress
Supplemental Material
sj-doc-4-sci-10.1177_00368504251326453 - Supplemental material for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study
Supplemental material, sj-doc-4-sci-10.1177_00368504251326453 for Impact of COVID-19 on the prevalence of oral and maxillofacial disorders: A retrospective cohort study by Bashar Abdullah, Omar Museedi, Noor Allawi, Fatimah J. Ismael and Saman Warnakulasuriya in Science Progress
Footnotes
Acknowledgements
We would like to extend our gratitude and appreciation to Dr Ameer Hameedi for his assistance with histopathological examination and diagnosis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement:
The data are available from the corresponding author upon reasonable request.
Data availability statement
The data are available from the corresponding author upon reasonable request.
Ethics approval statement
The study was approved by the Institutional Review Board at the University of Baghdad (reference number 936724).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: The study is self-funded. The findings of this study help guide the monitoring and targeted therapeutic strategies for managing oral and maxillofacial conditions during and after any viral pandemic.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.