
Abstract
Different methods have different diagnostic value under diverse clinical conditions. This study was conducted to analyze the clinical practical value of different assays in different situations and to establish the concept of an allergen diagnosis strategy.
This study used Phadia CAP, Advan Sure (AdvS), Euroline Camera (ELC), and Allergy Lateral Flow Assay (ALFA) kits to detect allergen specific immunoglobulin E (sIgE) in the sera from 30 allergic asthma patients, with Phadia CAP as the gold standard.
This study found high sensitivity for Dermatophagoides pteronyssinus in AdvS (92.6%), ELC (88.9%), and ALFA (85.2%), but poor sensitivity for F. domesticus in all three assays. Furthermore, the AdvS, ELC, and ALFA assays could detect 20, 21, and 8 allergens in one panel, respectively. The combination of the results showed that 93.3% and 46.7% of patients tested positive for ≥5 and ≥10 types of allergens, respectively. All patients who were tested positive for the Marine fish mixture were positive for both Shrimp and Crab. Similarly, patients who were tested positive for Chicken also tested positive for Pork. Optimal scale analysis showed a strong connection between Peanut, Soybean, Wheat, Japanese Hop, Western ragweed, and Oak allergens (Cronbach’s α = 91.1%).
The ELC assay was more suitable for use in pollen-rich areas, whereas the ALFA assay was easy to establish in areas with poor medical conditions. An allergen diagnosis strategy needs to be considered for use in clinical practice.
Keywords
Introduction
The detection of serum allergen-specific immunoglobulin E (sIgE) is an important step in the diagnosis of allergic diseases. The ImmunoCAP assay is the “international gold standard” for allergen detection, and it has wide application in the clinical practice for several years. 1 However, there are limitations associated with the use of ImmunoCAP in regions with poor medical facilities and shortage of medical resources because of the expensive reagents and sophisticated instruments required for this assay. 2
As a result of the development of medical science and biotechnology, the diagnostic methods for allergens have become more accurate and advanced. However, compared to sophisticated diagnostic techniques,3,4 inexpensive and simple methods for screening allergies would be more important in developing countries with large populations comprising potentially allergic patients. 5 This is because these regions need assays that are easy to establish and are affordable for their patients, although the assays may only indicate the sensitization of patients instead presenting accurate serum sIgE levels. Unfortunately, research on the clinical applications of handy allergen detection techniques have been neglected, especially in China and Africa, which have a wide variety of allergens and urgently needed a suitable method for the in vitro detection of allergens.
Therefore, in this study, we simultaneously used four diagnostic methods, including Phadia CAP, Advan Sure (AdvS), Euroline Camera (ELC), and Allergy Lateral Flow Assay (ALFA), to detect the serum sIgE for allergens (Dermatophagoides pteronyssinus, Blatella germanica, Artemisia vulgaris, Felis domesticus) in the same patient sample, with ImmunoCAP as the gold standard, to illustrate the clinical value of these assays in different regions as well as to provide a new allergy map for each patient.
Materials and methods
Patients
In this prospective study, we used the sera of 30 patient’s with allergic asthma that were randomly obtained from the serum bank of the Allergy Information Repository from January 2017 to December 2018 in Guangzhou, China. The samples were selected based on the following inclusion criteria: (1) patients who had clinical symptoms of allergy, such as wheezing, dyspnea, and/or chronic cough, that were not caused by a cold, sneezing, runny nose, nasal obstruction, or nasal itching; (2) patients who were positive for at least one of the allergen serum sIgE, including D. pteronyssinus, F. domesticus, B. germanica, and A. vulgaris on an assay conducted on the Phadia 1000 (≥0.35 kU/L; ThermoFisher, Sweden); and (3) no history or current use of specific allergen immunotherapy, with no autoimmune diseases, parasitic infections, or cancer. The diagnosis of asthma was recorded based on the Global Initiative for Asthma 6 criteria that were evaluated by a respiratory specialist.
Measurements
All sera samples were simultaneously assayed for allergen sIgE levels using the AdvS (The Republic of Korea, LG), ELC (Germany, EUROIMMUN), and ALFA (Germany, DR FOOKE) assays. Results ≥0.35 kU/L were considered positive, in accordance with the respective manufacturer’s guideline. The degree of allergy was defined in accordance with the radioallergosorbent test (RAST) class as follows: Class 1: 0.35–0.70 kU/L; Class 2: 0.70–3.50 kU/L; Class 3: 3.50–17.50 kU/L; Class 4: 17.50–50.00 kU/L; Class 5: 50.00–100.00 kU/L; and Class 6 is ≥ 100.00 kU/L. An introduction to the three assays and detailed information of the test panels are presented in the Appendices .
Statistical analysis
Statistical analyses were conducted with the SPSS 25.0 (SPSS, Chicago, IL). The categorical data are reported as percentages that shows the proportion of positive results, and the chi-squared test was used to compare the variances of data among the study groups. Correlation analyses between the sIgE results of Phadia CAP, AdvS, ELC, and ALFA were undertaken using the Spearman’s test, with the correlation coefficients presented as “rs.” The consistency of the results stratified by the RAST classes between the Phadia CAP, AdvS, ELC, and ALFA assays are presented as the Kappa index (ka). The diagnostic performance, including the sensitivity, specificity, positive or negative predictive values, and accuracy, of AdvS, ELC, and ALFA were calculated using the ImmunoCAP results as the reference standard. The correlation between the allergen serum sIgE level was calculated with the optimal scale analysis. p < 0.05 was considered statistically significant.
Results
Comparison of the results of the AdvS, ELC, and ALFA assays
Totally, there were 27 (90.0%), 5 (16.7%), 16 (53.3%), and 11 (36.7%) patients positive to D. pteronyssinus, F. domesticus, B. germanica, and A. vulgaris respectively by the gold-standard test (Phadia CAP assays). Then, the comparison results show that there was a high sensitivity for D. pteronyssinus in the AdvS (92.6%), ELC (88.9%), and ALFA (85.2%) assays. However, the sensitivity for F. domesticus was poor in the above mentioned three assays (all <50.0%). For B. germanica, the sensitivity in ELC was highest (75.0%), whereas, for A. vulgaris, the sensitivities of ELC and ALFA were 75.0% (Table 1). For A. vulgaris, there were eight patients had positive results in ImmunoCAP, AdvS, ELC, and ALFA assays at the same time (Figure 1).
Diagnostic performance of AdvS, ELC, and BioIC.
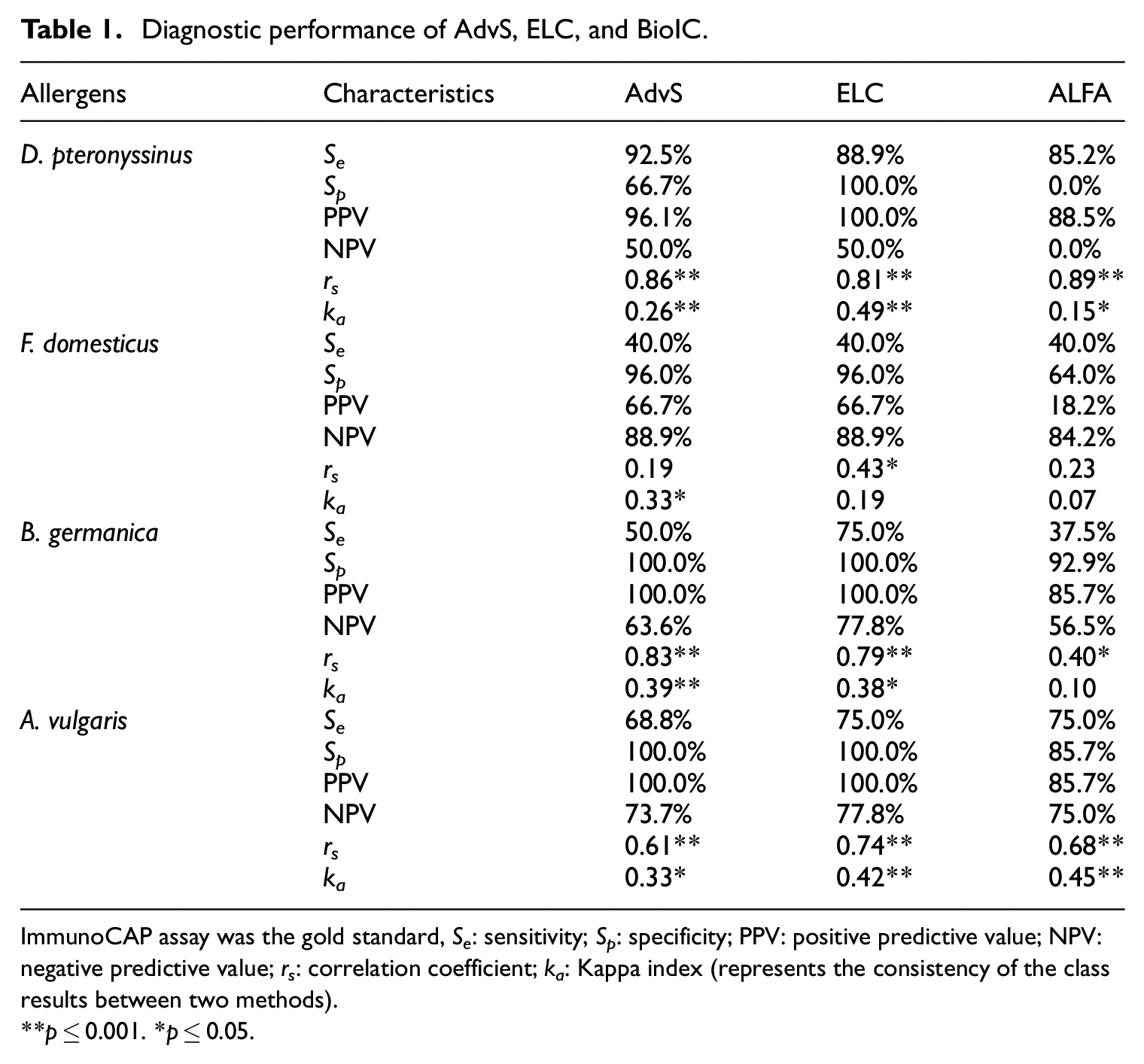
ImmunoCAP assay was the gold standard, Se: sensitivity; Sp: specificity; PPV: positive predictive value; NPV: negative predictive value; rs: correlation coefficient; ka: Kappa index (represents the consistency of the class results between two methods).
p ≤ 0.001. *p ≤ 0.05.

Venn diagram-based analysis. The agreement of the results of allergens: (a) D. pteronyssinus, (b) F. domesticus, (c) B. germanica, and (d) A. vulgaris from four assays. For A. vulgaris, there were eight patients had positive results in ImmunoCAP, AdvS, ELC, and ALFA assays at the same time.
Co-sensitization map of patients with asthma
Interestingly, the AdvS, ELC, and ALFA assays could detect 20, 21, and 8 allergens and allergen mixtures in one panel, respectively. A total of 10 allergens, including Alternaria. alternata, Western ragweed, Dermatophagoides farinae, Oak, Chicken, Pork, Wheat, Japanese hop, Grass mixture (Bermuda grass, Cocksfoot, Timothy grass, and Sweet vernal grass), and Tree mixture (Birch and Alder), were the unique allergens only identified in the AdvS panel. Mutton, Beef, Scandent hop, Carbohydrate cross-reactive determinants (CCD), Mold mixture (Penicillium chrysogenum, Cladosporium herbarum, Aspergillus fumigatus, and Mucor racemosus), Freshwater fish mixture (Salmon, Bass, and Carp), Marine fish mixture (Cod, Lobster, and Scallop), and Trees (Willow, Aspen, and Elm) were the eight unique allergens only in ELC panel. Blomia tropicalis allergen was the only unique in the ALFA panel (Appendices).
Therefore, a total of 33 allergens were tested with sera of 30 subjects with allergic asthma (Figure 2). Among them, 93.3% patients tested positive for five or more allergens, and 46.7% patients tested positive for ≥10 types of allergens. With regard to the fish allergens, 16.7% and 13.3% patients simultaneously tested positive for the Marine fish mixture and Freshwater fish mixture; moreover, the patients who were tested positive for the Marine fish mixture tested 100% positive for both Shrimp and Crab allergens. With regard to the meat allergens, the positivity rate for Pork and Chicken were 6.7%, whereas 3.3% patients were positive for Beef. Furthermore, patients positive for Chicken were all positive for Pork. For pollen allergens, the highest positivity rate was observed for the Grass mixture (50.0%), followed by CCD (36.7%); in addition, the patients who were tested positive for CCD simultaneously tested positive for Crab, Trees, Common ragweed, D. pteronyssinus, and D. farinae. Moreover, among the patients with an A. vulgaris allergy, 81.3% and 87.5% were also positive for the Grass mixture and B. germanica, respectively. In addition, all of the patients who were tested positive for Soybean allergy were positive for Wheat allergy (Figure 2(a)). In the optimal scale analysis, the closer the points are, the stronger is the correlation between them. We found that there was a strong connection between the Scandent hop, Common ragweed, and CCD as well as between Peanut, Soybean, Wheat, Japanese hop, Western ragweed, and Oak (Cronbach’s α = 91.1%) (Figure 2(b)).
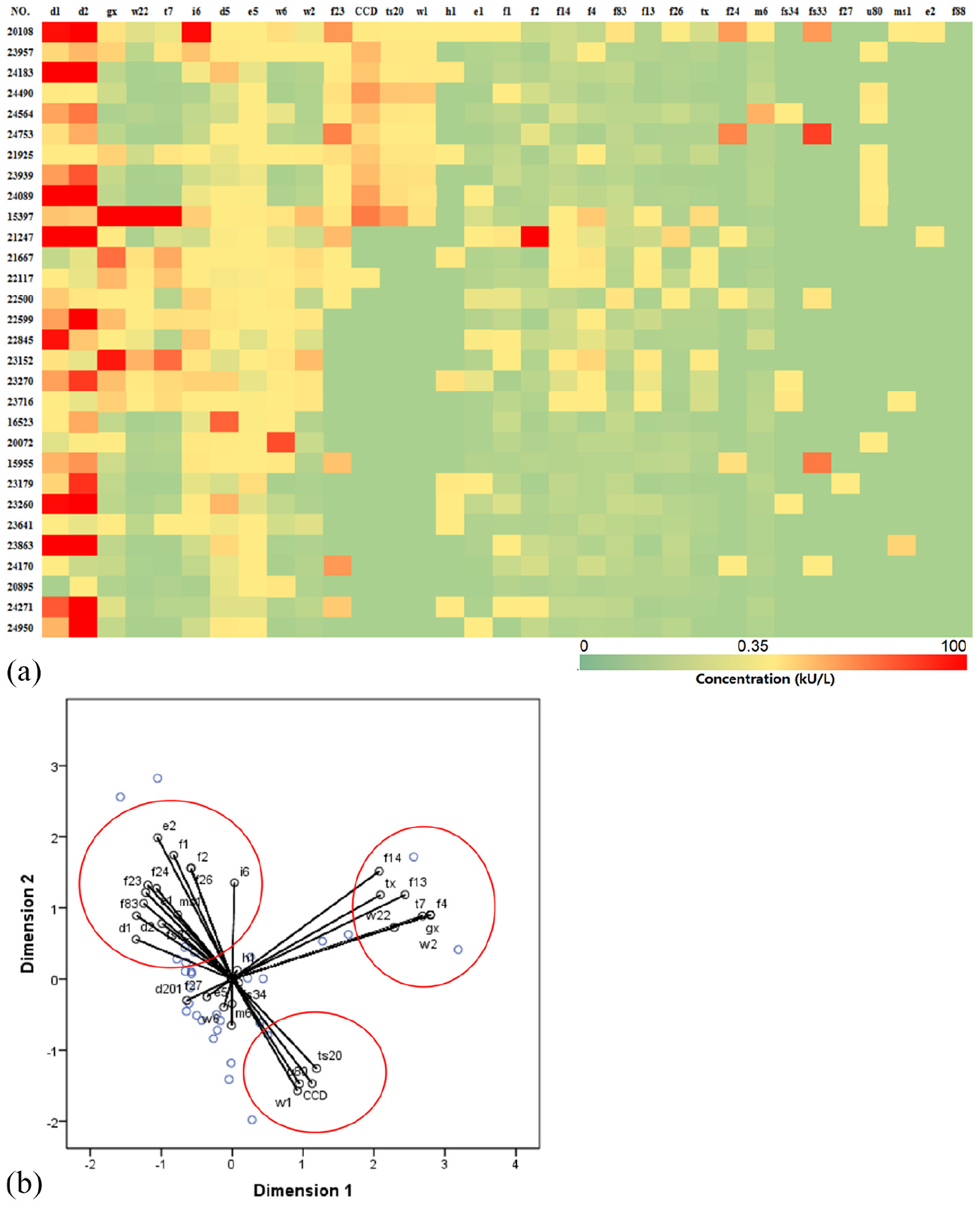
Thermogram and optimal scale analysis of patients with multiple sensitizations: (a) the thermogram and (b) optimal scale analysis based on the patient’s specific immunoglobulin E (sIgE) concentration by ImmunoCAP.
Discussion
In a previous research study, we found that in more than 32.7% of patients with chronic obstructive pulmonary disease (COPD) and 45.9% of those with asthma had atopy, 7 and allergen detection played an important role in patients with chronic respiratory diseases. For this reason, in the present study we have examined and partly compared four different measuring systems for sIgE. For D. pteronyssinus, AdvS had the highest sensitivity, while for B.germanica, ELC had the highest sensitivity. In addition, Freshwater-fish-mixture, Marine-fish-mixture, and Scandent hop were the unique panels in ELC, which were not available when using ImmunoCAP. Meanwhile, the ELC assay included a variety of pollen allergens in a single panel, which made it more suitable for asthma patients in pollen-rich areas, such as Northern China. 8 The ALFA assay, which was handy and inexpensive, had a high sensitivity and specificity to mite allergens; therefore, using it in the areas with poor medical conditions, especially in the tropical or subtropical regions, where dust mites was the main allergen9,10 can effectively reduce the medical costs and prove easy to establish allergen identification. AdvS could supplement the deficiencies of other assays because it included rare allergens such as pork and chicken, which was also mentioned in a Korean study. 11 For the asthma patients with simultaneous skin atopy, doctors can prescribe the AdvS allergen detection test.
Several previous studies have only focused on the in-depth analysis of a single detection technology and their findings have not been translated into actual clinical practice.12,13 Faced with increasingly new diagnostic technologies, there is a need to pay greater attention to the diagnostic strategy of these technologies under different conditions.
The allergen diagnosis strategy is a concept that encourages the selection of the most cost-effective, appropriate, and comprehensive method to assess the patient’s allergy status in different situations. 14 The outcome of this strategy depends on the studies of the allergen detection technology and the epidemiology of allergic diseases. In this study, we identified and described these aspects to guide doctors to prescribe the accurate allergen tests in developing countries. The small sample size and lack of sample size calculation analysis were the main limitation of this study; however, it does not detract from the sound clinical basis of this concept and the validity of the experimental results.
In addition, in this study, we used four diagnostic methods to detect allergens in a 30-patient study sample. We found that rare allergens that may escape detection on routine analysis, such as the Marine fish mixture, showed a high positivity rate as well as potential co-sensitization. With the changes in people’s lifestyle in recent years and the modernization of cities in China, 15 the types of allergens are increasingly becoming abundant and unpredictable. In Guangzhou, the traditional marine fish dishes may be an important source of local allergens. However, in current clinical practice, due to the lack of domestic methodologies that are suited for clinical application in local hospitals, the importance of Marine fish allergens has been ignored in local patients. Therefore, the development of allergen detection technology by the manufacturer and the selection of allergen detection 16 assay by the doctor needs to consider the local situation.
Conclusion
The ELC assay was more suitable for use in pollen-rich areas. The ALFA assay was easy to use in the areas with poor medical conditions. Therefore, the allergy map should gradually complement the clinical management of patients with allergies in the future, especially for asthma.
Footnotes
Appendices
Acknowledgements
We thank everyone involved in the collection, detection, and date management of the serum samples. We thank Professor Hammer Tsui for English editing.
Author contributions
B.Q.S. conceived and designed the experiments. H.S.H wrote the main manuscript text. X.W.Z., Z.F.H., and C.X.L. designed and performed the measurements. W.T.L., H.S.H., and H.C. interpreted the experimental data and performed data analysis. All authors approve and agree to the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (Project No.: 81601394), Bureau of Traditional Chinese Medicine Scientific Research Project of Guangdong (Project No.: 20192048), Science and Technology Innovation Committee Project of Guangzhou (Project No.: 201831802).
Ethics approval
Ethical approval for this study was obtained from First Affiliated Hospital of Guangzhou Medical University (GYFYY-2016-73).
Informed consent
Written informed consent was obtained from all subjects before the study.
Author biographies
She is currently the Vice Chairman of the Allergy Prevention and Control Committee of the Chinese Preventive Medical Association; Vice Chairman of Allergy Medicine Committee, Chinese Association of Research Hospitals; Leader of China Allergen Prevention Group; Chairman of the Special Committee for Allergy Prevention and Control, Guangdong Preventive Medical Association; Vice chairman of the first committee of Cell Morphology Diagnosis Branch of Guangzhou Medical Association; Member of the Standing Committee of the Respiratory Committee of the Chinese Women Physicians Association; Member of the Allergic Diagnosis and Immunotherapy Group of Chinese Medical Association; Chairman of Guangdong Zhong Nanshan Medical Foundation; Member of the Standing Committee of Pulmonary Allergy, Guangdong Chest Disease Society; Member of the Standing Committee of Guangdong Allergy Society; Member of the Standing Committee of Multidisciplinary Diagnosis and Treatment of Diffuse Substantial Pulmonary Disease, Guangdong Chest Disease Society; First member of Medical Law Branch of Guangdong Medical Association; Standing director of the Chinese Medicine Immunization Professional Committee, World Federation of Chinese Medicine Societies; Member of the Standing Committee of Laboratory Medicine Branch of Guangzhou Medical Association, expert of medical malpractice technical appraisal of Guangzhou Medical Association, evaluation expert of National Natural Science Foundation, editorial member of the 7th Editorial Committee of International Journal of Respiration, high-level health talents in Guangzhou. She has made speeches in academic exchanges at home and abroad and hosted academic conferences on allergy. Since 2013, she has hosted national, provincial and municipal continuing education classes on the new progress in the diagnosis and treatment of allergic diseases every year.