
Abstract
Allergic fungal rhinosinusitis has been well characterized clinically. We report about a patient diagnosed with allergic fungal rhinosinusitis. Nasal cultures revealed a rare fungal pathogen, Aspergillus nidulans. At the time of initial presentation and later recurrence, another rare fungus was found. Trichoderma are unique and have been described in detail. This report describes unique pathogens causing allergic fungal rhinosinusitis. The relevant literature demonstrates the potential morbidity and mortality due to infections from such organisms, indicating the need for physicians to manage and treat this condition carefully to prevent potential complications.
Introduction
Allergic fungal rhinosinusitis (AFRS) is a well-known clinical condition that affects the paranasal sinuses. It is defined as an immunoglobulin E-mediated immune response triggered by fungal antigens. The diagnosis is confirmed based on the Bent and Kuhn criteria. 1 These criteria have been widely accepted and help differentiate AFRS from other forms of fungal rhinosinusitis. One essential component of these criteria is identifying fungal organisms by staining or culture. The dematiaceous family is the most common causative organism of AFRS. 2 This is inconsistent with local data in Saudi Arabia, which indicates that Aspergillus species are the most common causative fungal pathogens (67.8%), followed by dematiaceous fungi (32.2%). 3
Here, we report a unique case of AFRS caused by Aspergillus nidulans in association with Citrobacter koseri. A. nidulans-triggered rhinosinusitis exacerbated by Citrobacter koseri might increase the chance of recurrent sinusitis. Although A. nidulans is a rare cause of AFRS, its potential virulence needs to be considered during patient management. This patient experienced AFRS recurrence, and the second culture contained Trichoderma species. This is rare and to our knowledge has not been reported with A. nidulans.
Case report
A 20-year-old immunocompetent Saudi male with complaints of progressive bilateral nasal obstruction associated with hyposmia for 1 year presented to the clinic. He also reported symptoms consistent with allergic rhinitis. Physical examination revealed bilateral nasal polyps (grades 3 and 4 in the right and left nasal cavities, respectively, as per the Meltzer 4 clinical scoring system for nasal polyps). Sinus computed tomography (CT) revealed opacified sinuses (Figure 1(A) to (D)). The patient was scheduled for sinus surgery and received preoperative steroids. Eosinophilic mucin was found intraoperatively, with no evidence of mucosal invasion. Fungal staining and culture identified the organism to be A. nidulans. C. koseri was noted in subsequent tissue culture. Based on these findings, the final diagnosis was AFRS because the patient met the Bent and Kuhn criteria. 1
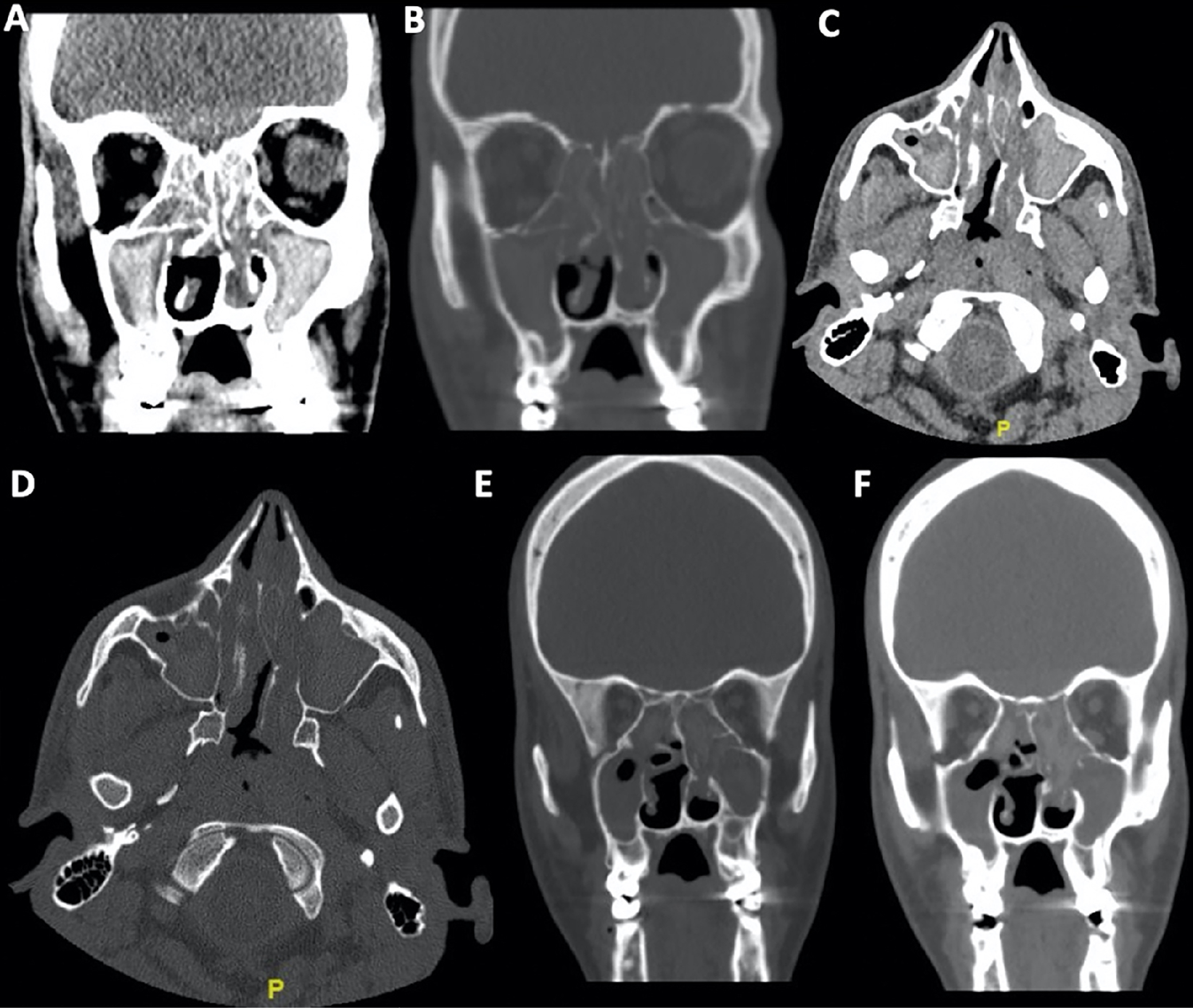
Preoperative computed tomography scans representing the initial (A–D) and recurrent (E and F) sinusitis. A: coronal view; soft tissue window. B: coronal view; bone window. C: axial view; soft tissue window. D: axial view; bone window. E: coronal view; bone window. F: coronal view; soft tissue window.
The patient received carbamazepine and levetiracetam for a seizure disorder. He also underwent multiple pelvic surgeries for developmental hip dysplasia during childhood. Postoperatively, he was maintained on a nasal high-volume douche and topical intranasal steroids. Despite regularly using fluticasone nasal spray and intermittent budesonide (1 mg/2 mL) nasal drops, the patient returned with complaints of nasal obstruction and discharge that had persisted for 1 year, that is, these symptoms initiated 3 years after the first surgery. Imaging studies confirmed AFRS recurrence (Figure 1(E) and (F)). The patient had a Sinonasal Outcome Test-22 Items (SNOT-22) score of 26/110, with the nasal component being affected the most (SNOT-22 items 1-7, 11-12) (Figure 2). He underwent revision surgery 4 years after the first surgery, and eosinophilic mucin was observed intraoperatively again. A fungal culture grew Trichoderma species. The nasal polyp specimen showed high eosinophil infiltration, with more than 70 eosinophils per high-power field. The patient was followed up during weeks 1 and 6 postoperatively and has shown significant improvement in sinonasal symptoms.
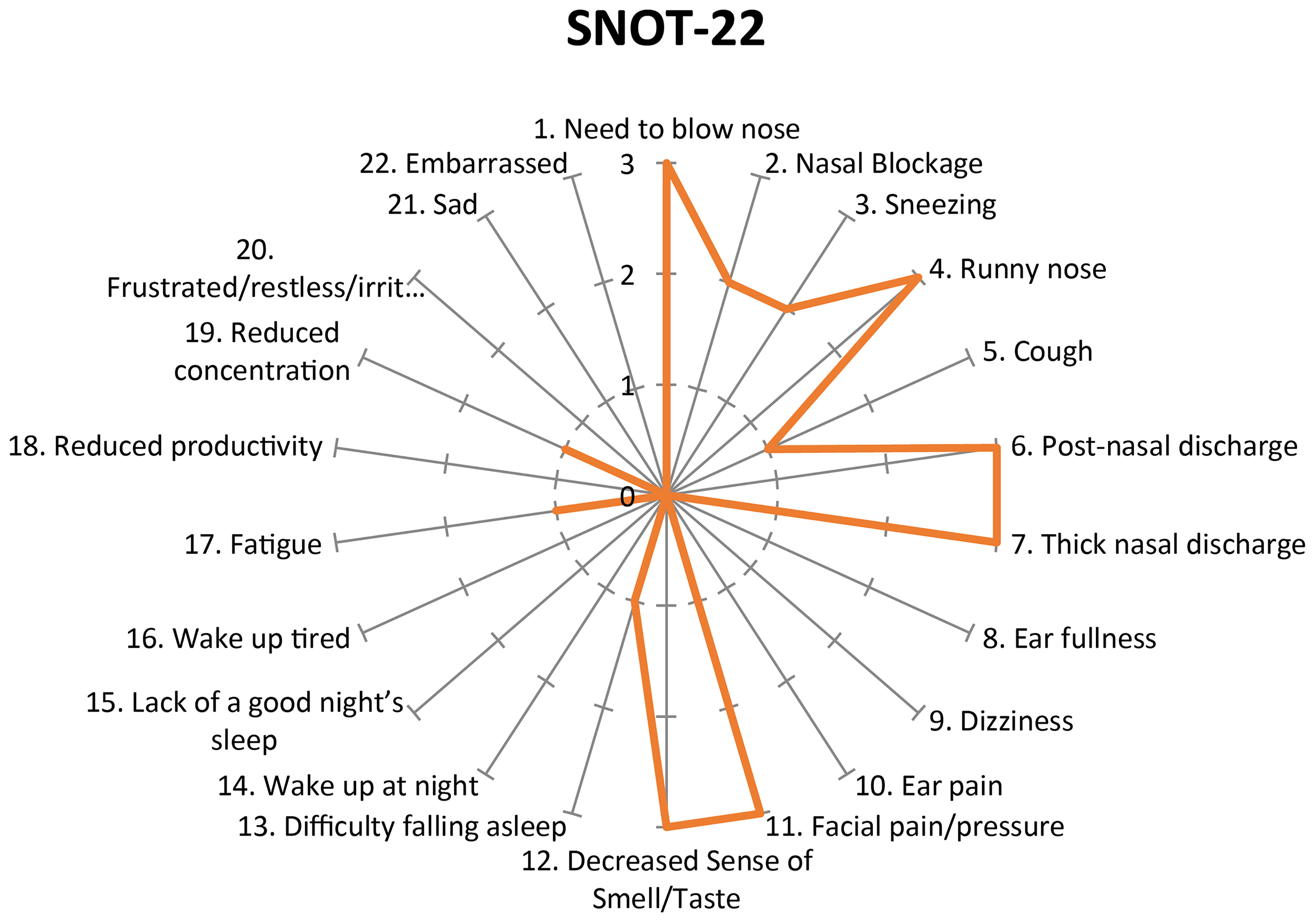
SNOT-22 score prior to recurrence. Note the maximum in any item (thick gray line) is 3/5 on a 0–5 scale as reported by the patient.
Discussion
Among pathogenic aspergilli, A. fumigatus is most ubiquitous in the environment and is the major cause of disease, followed by A. flavus, A. niger, A. terreus, and A. nidulans (Figure 3). 5 A. nidulans has been reported as a cause of AFRS in only one patient with bilateral nasal obstruction due to sinonasal polyposis, who underwent endoscopic sinus surgery with polypectomy. 6 In a retrospective study in Saudi Arabia, among 40 AFRS cases in which fungi were identified by culture, A. flavus was identified most frequently (33 cases), followed by A. niger (4 cases), A. terreus (2 cases), and unspecified Aspergillus species in one case. 3 A. nidulans was not reported as a causative fungus.
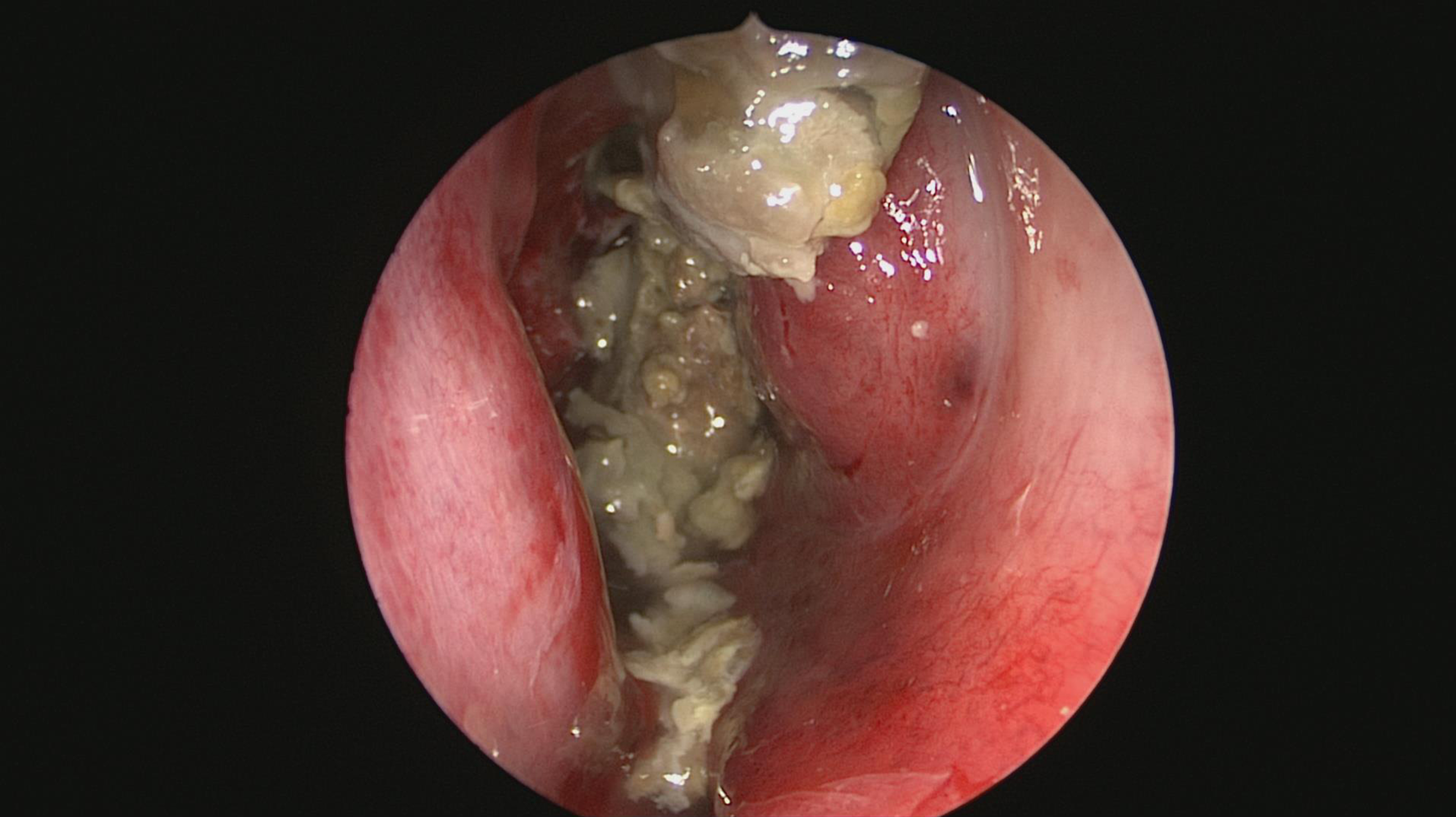
An intraoperative view of eosinophilic mucin (previously known as allergic mucin).
The pathogenicity of A. nidulans has been well documented in the literature.
A. nidulans affects the maxillary sinus, and in two cases of fungal ball, A. nidulans was related to the foreign material during dental treatment.7,8 Although A. flavus has been implicated as a common cause of chronic granulomatous invasive fungal sinusitis, one case with concomitant Pott disease and tuberculosis was linked to A. nidulans. 9 Additionally, the lower airway is not immune to this pathogen; a rare case of chronic necrotizing pulmonary aspergillosis was attributed to A. nidulans. 10
Morbidity/mortality rates among different Aspergillus species have not been studied well, given the rarity of A. nidulans as a cause of invasive and non-invasive sinusitis. One study included cases diagnosed to have chronic granulomatous disease (CGD) with osteomyelitis due to A. nidulans and compared them with cases caused by A. fumigatus. Osteomyelitis caused by A. nidulans was associated with pulmonary infection, and about 50% of these patients with CGD died, whereas no patient with A. fumigatus-induced osteomyelitis died, indicating that A. nidulans might be associated with higher mortality. 11
C. koseri is a rare cause of sinusitis. A patient reported having severe psychomotor retardation due to epilepsy displayed preoperative purulent nasal discharge containing Pseudomonas aeruginosa and C. koseri. Later his CT revealed brain atrophy and pneumoceles of the frontal sinuses with sinusitis. Sinusitis recurred after endoscopic sinus surgery, and the patient underwent revision surgery. Macrolide therapy, daily irrigation, and frequently lying in the prone position were performed to promote drainage from the frontal pneumoceles; there was no infection recurrence up to 5 months after the second surgery. 12 Interestingly, our patient also had a history of epilepsy, which was controlled with medication; however, he was immunocompetent with normal cognitive function, suggesting that the severity in the previous case could have been due to another underlying condition.
Early diagnosis and management can help cure sinusitis and prevent complications. Different treatment lines are used to treat invasive and non-invasive A. nidulans infection, including debridement and antifungal and gene therapy, all of which have good outcomes.13–15 Similar to A. nidulans, Trichoderma species can cause disease in immunocompromised patients and were reported to cause acute invasive sinusitis. 16 Additionally, Trichoderma longibrachiatum was identified in an immunocompetent patient diagnosed with sphenoid sinusitis. 17 T. longibrachiatum caused AFRS in another patient who was successfully treated with a combination of sinus lavage, oral corticosteroids, itraconazole, and allergen immunotherapy. 18 These, along with our case, are the first reported AFRS cases caused by Trichoderma species, to the best of our knowledge.
Given the rarity of these fungi, potential morbidity/mortality, and likelihood of disease recurrence, we recommend long-term regular follow-up and repeated surveillance sinonasal endoscopy to detect recurrence signs.
Limitations of the study include the possibility of false-positive identification of A. nidulans. Misidentification of many Aspergillus species as A. nidulans can occur due to similar phenotypic characteristics. 19 When these rare fungi are encountered, we recommend performing genome sequencing. The fact that this is a single case report is another limiting factor preventing generalization of our findings.
In conclusion, the growth of these rare fungal organisms in culture and a confirmed AFRS diagnosis should alert physicians about the potential morbidity/mortality and the need for prompt, aggressive, and timely management.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from King Saud University Institutional Review Board (E-20-5470).
Statement of informed consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.