
Abstract
Strong lockdowns to control COVID-19 pandemic have been enforced globally and strongly restricted social activities with consequent negative effects on mental health. Japan has effectively implemented a unique voluntary policy to control COVID-19, but the mental health impact of the policy has not been examined on a large scale. In this study, we examined the effect of the first declaration on the mental health of affected residents. We used population-level questionnaire data of 17,400 people living under the state of emergency and 9208 who were not through a social-networking-service app and applied a difference-in-differences regression model to estimate the causal effect of the declaration of the state of emergency on psychological wellbeing, stratified by job category. No statistically significant effect of the declaration was observed among all job categories. This suggests that residents’ psychological situation has gradually changed, possibly influenced by other factors such as the surrounding environment, rather than the declaration itself. Given that Japan has a unique policy to control COVID-19 instead of a strict lockdown, our results showed the Japanese-style policy may serve as a form of harm reduction strategy, to control the epidemic with minimal psychological harm, and enable a policy that balances disease control and mental health. Caution is necessary that this study used self-reported data from a limited time period before and after the first declaration in April 2020.
Introduction
The World Health Organization publicly declared the coronavirus disease 2019 (COVID-19) pandemic on March 11, 2020. In response the Japanese prime minister at the time, Shinzo Abe, declared a state of emergency in 7 of Japan’s 47 prefectures on April 7, 2020 1 and extended it nationwide on April 16, 2020 2 This declaration lacked any legal force, and COVID-19 control in Japan was essentially driven by the voluntary effort of residents. 3 Despite this, the number of deaths is remarkably low among the G7 nations (1148 deaths and 58,711 confirmed cases as of mid-August 2020). 4 suggesting that Japan has successfully controlled the infection with a unique voluntary policy.
Globally, strict lockdowns have been enforced that have strongly restricted economic and social activities with consequent negative effects on health and welfare, 5 including current and future mental health. 6 Similar impacts on mental health were observed in past outbreaks of Severe Acute Respiratory Syndrome, and Ebola virus.7–9 However, even though Japan has effectively implemented a voluntary policy to control the infection, the mental health impact of the policy has not been examined on a large scale. In this study, we examined the effect of the first declaration of a state of emergency in response to COVID-19 in Japan on the mental health of affected residents.
Method
Participants
We used data collected as part of the COOPERA (COVID-19: Operation for Personalized Empowerment to Render smart prevention And care seeking) project. 10 COOPERA uses a chatbot on LINE (one of the most popular social networking services in Japan) to ask users to report COVID-19 related symptoms if any, and provides feedback regarding COVID-19 measures to those who use it. The details of COOPERA can be found elsewhere. 10 Those who reported having any COVID-19-related symptoms were additionally asked about mental wellbeing during the past 30 days using a 5-point Likert scale (0–4 points) on three dimensions of mental health that partially utilized the K6 score. The K6 score is one of the most widely used mental health screening scales and originally contained six items. 11 Since the purpose of this service was to screen for COVID-19-related health concerns and to provide appropriate information quickly at the prefectural level, rather than simply screening for psychological distress, the following three items were selected out of the six: “about how often during the past 30 days did you feel nervous?,”“during the past 30 days, about how often did you feel restless or fidgety?,” and “how often did you feel so depressed that nothing could cheer you up?.” This scale has been validated in the Japanese population. 12 We used data on respondents aged 15–101 who lived in Fukuoka and Hyogo Prefectures (hereafter referred to as the “declaration group,” where the state of emergency was announced on April 7) and Fukui, Kyoto, Mie, Nagasaki, and Shiga Prefectures (the “non-declaration group,” where the state of emergency was announced on April 16). We divided the study period into two 1-week periods: the before-declaration period (BD) from March 31 to April 6, 2020 and the after-declaration period (AD) from April 7 to 14, 2020.
Statistical analysis
The three psychological wellbeing questions were summed to a total score between 0 and 12. We used a difference-in-differences (DID) regression model to estimate the causal effect of the declaration of the state of emergency on this score. 13 The DID approach assumes that, if the declaration was not effective in the declaration group, the average change in scores between BD and AD would be equal in both the declaration and non-declaration groups. The causal effect was calculated as the difference in the average change in score between BD and AD in the declaration group minus the change in the non-declaration group. In addition, we fitted the following linear regression model by job category, adjusting for confounder variables including age, gender, fever temperature, and current symptoms:

where
Result
There were 26,608 COOPERA users (declaration group: 17,400 and non-declaration group: 9208). Figure 1 shows the distribution of the total score, stratified by job category, BD/AD and declaration/non-declaration groups. There were 1533 students, 13,977 employees, 4076 unemployed, 4382 part–time workers, and 2630 self-employed respondents. The average changes in the total score in declaration and non-declaration groups were 0.126 (+3.25%) and 0.039 (+0.99%) among employees, 0.119 (+2.61%), and 0.327 (+7.10%) among part-time workers, 0.244 (+5.65%) and 0.064 (+1.47%) among the self-employed, −0.093 (−2.60%) and −0.136 (−3.49%) among students, and 0.325 (+6.89%) and 0.237 (+4.86%) among the unemployed, respectively. The DID analysis showed no statistically significant causal effect of the declaration on the change of total score among all job categories (Supplemental Table S1). The estimated causal effects (i.e.
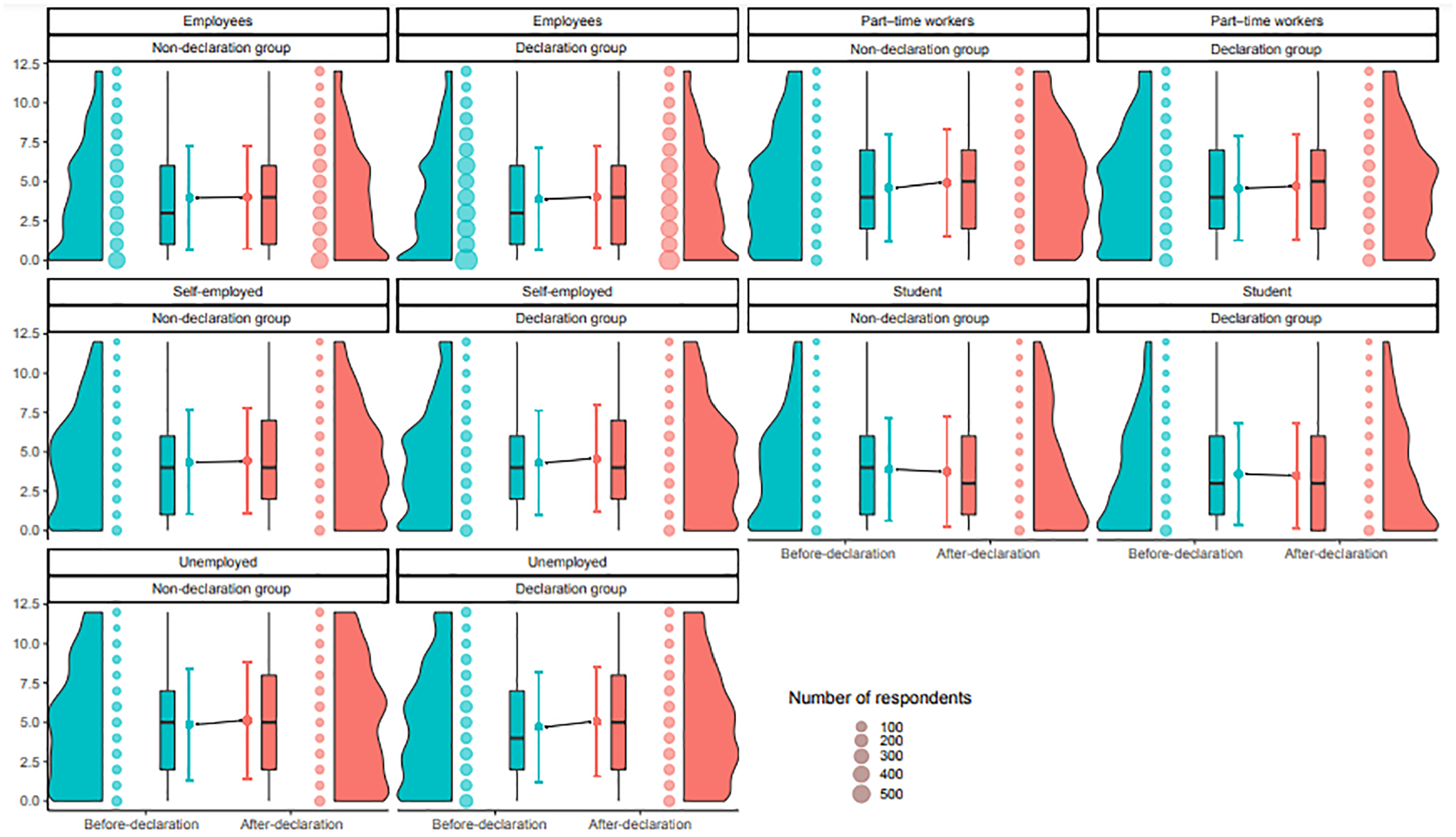
Raincloud plot of total score, stratified by employment categories, Before-declaration (BD)/After-declaration (AD) periods and declaration/non-declaration groups.
Discussion and conclusions
This study investigated the causal effect of the first declaration of a statement of emergency on the mental health of residents in Japan using a large scale monitoring scheme. Our results showed that, as expected, total mental health scores increased after the declaration among most employment categories. However, no statistically significant effects of the declaration were identified when applying the DID approach and the results were validated in a different population. This suggests that residents’ psychological situation has gradually changed, influenced by other factors such as the surrounding environment, rather than the declaration itself. It is worth noting that, unlike other job categories, the total score of students decreased, albeit not statistically significantly, after the declaration. This might be due to the fact that most school events during the end and beginning of school-year period were cancelled due to the declaration. However, further research is needed to understand the particular effect of school closures and the shift to online teaching on students. The limitations of the data used in this study are extensively discussed in previous studies describing the COOPERA system, including the use of self-reported data.10,15
In conclusion, given that Japan opted to control the COVID-19 epidemic using a voluntary rather than a strict lockdown, the Japanese-style policy might minimize psychological harm to those affected, enabling a balance between disease control for COVID-19 and mental health. In the voluntary nature of the Japanese lockdown residents could control the degree to which they were affected. Although the data in this study was limited to the early phase of the COVID-19 pandemic, our results provide useful insight for preparing lockdown strategies for the future resurgence of COVID-19 cases in other countries.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504211029793 – Supplemental material for Effect of emergency declaration on mental health during the COVID-19 pandemic in Japan: A social network service-based difference-in-differences approach
Supplemental material, sj-pdf-1-sci-10.1177_00368504211029793 for Effect of emergency declaration on mental health during the COVID-19 pandemic in Japan: A social network service-based difference-in-differences approach by Akifumi Eguchi, Daisuke Yoneoka, Shoi Shi, Yuta Tanoue, Takayuki Kawashima, Shuhei Nomura, Koji Makiyama, Shinya Uryu, Masayuki Sawada, Yumi Kawamura, Shinichi Takayanagi, Stuart Gilmour and Hiroaki Miyata in Science Progress
Footnotes
Acknowledgements
We would like to thank Fukui, Fukuoka, Hyogo, Kyoto, Mie, Nagasaki and Shiga Prefectures for installing the COOPERA system and providing us with data, LINE Corporation for developing and maintaining the system, and Amazon Web Services, Inc. for providing the data storage space. We are also grateful to the Japanese Society of Infectious Diseases for supervising the questionnaires and information provided to the participants from professional perspectives.
Authors’ contributions
All authors took responsibility for the integrity of the data and the accuracy of the data analysis. All the authors made critical revisions to the manuscript for important intellectual content and gave final approval of the manuscript. The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding bodies.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hiroaki Miyata reports a grant from the Ministry of Health, Labour and Welfare of Japan, outside the submitted work. All other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Ministry of Health, Labour and Welfare of Japan (H29-Gantaisaku-ippan-009), the Japan Agency for Medical Research and Development (AMED) (grant numbers JP20fk0108535) and Daiwa Securities Health Foundation.
Ethical approval
Ethical approval was granted by the ethics committee of Keio University School of Medicine, under authorization number 20190338.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.