
Abstract
The coronavirus 2019 (COVID-19) pandemic has caused dramatic changes in the daily lives of Romanians, affecting their mental health. The COVID-19 pandemic has evolved at three significant peaks, which sequentially occurred on: April 29, 2020; September 18, 2020; and the third wave registered the highest severity on November 27, 2020. Little is known about the mental health changes during this phase of this pandemic. This study evaluated mental health levels in Romania at the end of the first wave of the pandemic and amidst the third and most severe wave. We administered a two-phase internet-based survey among 543 and 583 participants, respectively, recruited through snowball sampling at a 6-month interval. The IPAT Anxiety Scale measured anxiety, the Beck’s Depression Inventory measured depression, and the Dissociative Experiences Scale measured dissociation. We observed no statistically significant differences in the number of participants with clinically relevant scores at either time point. In the first survey, 23.8%, 19.2%, and 32.6% reported being clinically anxious, clinically depressed, and showed clinical dissociation, respectively. Binary logistic regressions indicated that age, education level, and previous traumatic events were significantly associated with clinical levels of anxiety and depression. Moreover, multiple linear regression analysis reported a collective significant effect of gender, age, psychological impact, traumatic events, and dissociation on predicting high levels of anxiety and depression. Romanian adults’ mental health status was affected during the COVID-19 pandemic, and it did not change 6 months after the first lockdown.
Introduction
The novel coronavirus disease 2019 (COVID-19) has brought dramatic changes to everyday life, including economic and health impacts worldwide. The world faced significant, unique challenges characterized by a high level of insecurity, affecting humankind in all facets of life: intrapersonal, interpersonal, social, professional, financial, and spiritual.1,2 Anxiety, worry, and insecurity were provoked by the adverse effects on health 1 and the severe restrictions imposed, which significantly reduced the degree of personal freedom. Cross-sectional3–9 and longitudinal10,11 studies during the early stages of the COVID-19 pandemic found high rates of certain mental health symptoms—anxiety, depression, stress, and other mental health disorders—in different countries. A meta-analysis based on 9074 participants found that prevalence was 32% for anxiety, 34% for depression, and 30% for stress. 12 Many studies4,8,13 reported that distress during lockdown was associated with younger age and being female.
Previous pandemics have shown that mental health impacts can last longer and have a higher prevalence than the pandemic itself. In these circumstances, many health professionals have predicted a significant increase in the incidence of mental disorders.3,11,13 They expect mental health to become more problematic than the immediate effects of the virus. Various authors and professionals in the trauma field13–16 have affirmed that we are dealing with an unprecedented major collective trauma because of the broad extent and duration of the pandemic and our insufficient knowledge about the virus.
The Romanian government established a state of lockdown from March 16 to May 16, 2020. Between September and December, restrictions increased, with some regions going into quarantine. Between this study’s two surveys, the total number of confirmed COVID-19 cases increased from 16,895 to 365,212, and the number of deaths from COVID-19 increased from 1107 to 9075. 17
One of the few quantitative surveys to examine the impact of the COVID-19 pandemic on the life of Romanians was conducted in the first weeks of the COVID-19 crisis. It revealed a matrix of stress sources specific to the new pandemic context in Romania: limited freedom of movement (69%), changing personal plans (44%), obligation to isolate at home (37%), income reduction (24%), modified professional goals (18%), suspension of employment contracts (8%), technological unemployment (7%), job loss (4%), leave due to suspended courses (4%), and others (4%). Of the respondents, 8% responded that they had not been affected. 18
In contrast to other countries, existing studies in Romania concerning the prevalence of mental disorders in the general population are outdated, 19 and the studies conducted by the Romanian public health authorities are limited to declared patients. 20 The lack of data on anxiety, depression, and dissociation incidence in Romania’s general population during the pandemic required new research to reveal whether these mental health symptoms will persist in the long term or decline after the lockdown measures end.
The goal and research questions
The study’s main goal was to examine changes in adult mental health in the Romanian population during the COVID-19 crisis, based on measurements of personal perceptions and experiences. A secondary aim was to involve part of the general population in knowledge, exploration, and expression of their views on the current pandemic phenomenon.
This exploratory research on the pandemic phenomenon is intended to address the following questions:
How did the assessed psychological states of individuals change between two-time points: the end of the lockdown and 6 months later?
What socio-demographic and subjective factors correlate with symptoms of anxiety and depression?
How do emotional and cognitive dissociation influence anxiety and depression?
How does personal COVID-19 infection or infection in close family or friends influence the evaluated population’s psychological state?
Methods
Study design
Given the confinement situation, during which the population’s mobility and social contact were significantly reduced, we used a combination of snowball and random distribution sampling through social media to recruit study participants. Snowball sampling is useful when a sampling frame is difficult to identify. The goal was to collect the largest sample possible in a short time at a low-cost because the COVID-19 situation was rapidly evolving. Many previous studies have also used snowball sampling as a useful tool to assess mental health problems of different populations during the COVID-19 pandemic.4,5,10,21
To answer the research questions we designed an anonymous online survey that we administered at the end of Romania’s first lockdown (t1) and again after 6 months (t2).
Study sample
The inclusion criteria were as follows: (a) an adult of age 18 years or older (psychometric measures used in the study were designed for adults only); (b) living in Romania; (c) having provided consent to participate; and (d) desiring to support this research, as shown by self-selecting, which demonstrates sensitivity to and interest in the pandemic phenomenon.
Data collection
The online survey was presented in a Google Form and was promoted by distributing the survey link via email and social networking sites to reach the target population. Participants were requested to roll out the online questionnaire to as many people as possible, allowing numerous people swift access to the survey. First, the survey obtained the explicit consent of users, who were only allowed to proceed to the survey questions after providing written consent. Participation was voluntary and anonymous, and respondents could choose to withdraw from the study at any point. All questions were anonymized to preserve confidentiality.
Data collection was conducted from May 9 to May 15, 2020 (first survey) and November 8 to November 14, 2020 (second survey). A total of 1126 people participated in the initial assessment (n = 543) and the second evaluation (n = 583).
Ethical approval of the research protocol and instruments
The study protocol and instruments were approved by the research committee of the Department of Psychology and Pedagogy at the Spiru Haret University in Braşov, under document number 1/Psiho/6.04.2020.
Measurement and instruments
Argumentation
Subjective measures from self-reporting indices are invaluable for affective research because they provide insights into personal experience and serve as control parameters to track individual differences. 22 Self-reporting measures are also appropriate when the research objective is to evaluate a person’s subjective emotional experience about a particular event. 23
Diagnosing mental symptoms in the general population by professionals was not possible during the pandemic period because the risks of contamination were extremely high. Therefore, research conducted on the general population during this period typically used self-reporting methods to show that anxiety, depression, and psychological impact were based on personal feelings.10,24
Socio-demographic factors and subjective experiences
Socio-demographic factors included gender, age, and education level. Subjective experiences included traumatic events during the participant’s lifetime, the self-reported psychological impact of COVID-19, whether participants had themselves been infected with COVID-19, and whether they had loved ones infected with the virus.
Traumatic life events were measured using a scale with the following possible answers: no events; a few; many.
The self-declared psychological impact of the COVID-19 outbreak was measured using a scale with the following possible answers: normal–light; moderate; severe; extreme.
The questions regarding a participant’s COVID-19 infection and cases of infected loved ones had two possible responses: yes and no.
Anxiety, depression, and dissociation
Anxiety was measured using the IPAT Anxiety Scale, 25 which comprises 40 items divided into five subscales, each of which is assumed to measure one of the five oblique first-order factors whose intercorrelations define the second-order factor of anxiety. As per Catell’s 25 understanding, the characteristic features of anxiety were associated with personality traits and manifested as anxiety in stressful situations. Cronbach’s alpha for the IPAT Anxiety Scale in this study was .897.
Depression was measured using Beck’s Depression Inventory (BDI). 26 BDI is a 13-item self-report questionnaire assessing the severity of depression symptoms. Cronbach’s alpha for BDI in this study was .844.
Dissociation was measured using the Dissociative Experiences Scale (DES-II), a screening tool for dissociative disorders that measures several dissociation types, including problematic and ordinary dissociative experiences. People with post-traumatic stress disorder typically exhibit high scores. 27 The DES-II consists of 28 questions with responses ranging from 0% to 100% (increasing by units of 10%). Cronbach’s alpha for the DES-II in this study was .958.
Statistical analysis
IBM SPSS for Windows Version 21 was used for the statistical analysis. Descriptive statistics were conducted to describe the demographic characteristics and scales’ mean values. Independent samples t-tests were used to compare the mean scores for anxiety, depression, dissociation, and self-declared impact, between the first and second survey. Chi-squared tests were used to analyze the differences in categorical variables between the first and second surveys. A separate bivariate logistic regression analysis evaluated the degree of association between the independent variables and anxiety, depression, and dissociation. The significance level was calculated using a p-value <.05 and a confidence interval (CI) of 95%.
Additionally, the bootstrap method was used to verify and validate statistical results to counter the disadvantages of snowball sampling, such as the small size of the male group compared to the female group. Bootstrapping is a statistical procedure that resamples a single dataset to create many simulated samples and increase statistical precision. 28 The bootstrap method enables the development of a probability model, based on the information provided by the sample, thereby, disproving the assumptions for the theoretical distribution and facilitating the inferences regarding the study population. 29 Therefore, the results obtained using the bootstrap technique are more reliable and robust than the findings obtained from classical statistical methods. As a result, the bootstrap method is often used in the other studies. 30
Results
Demographics
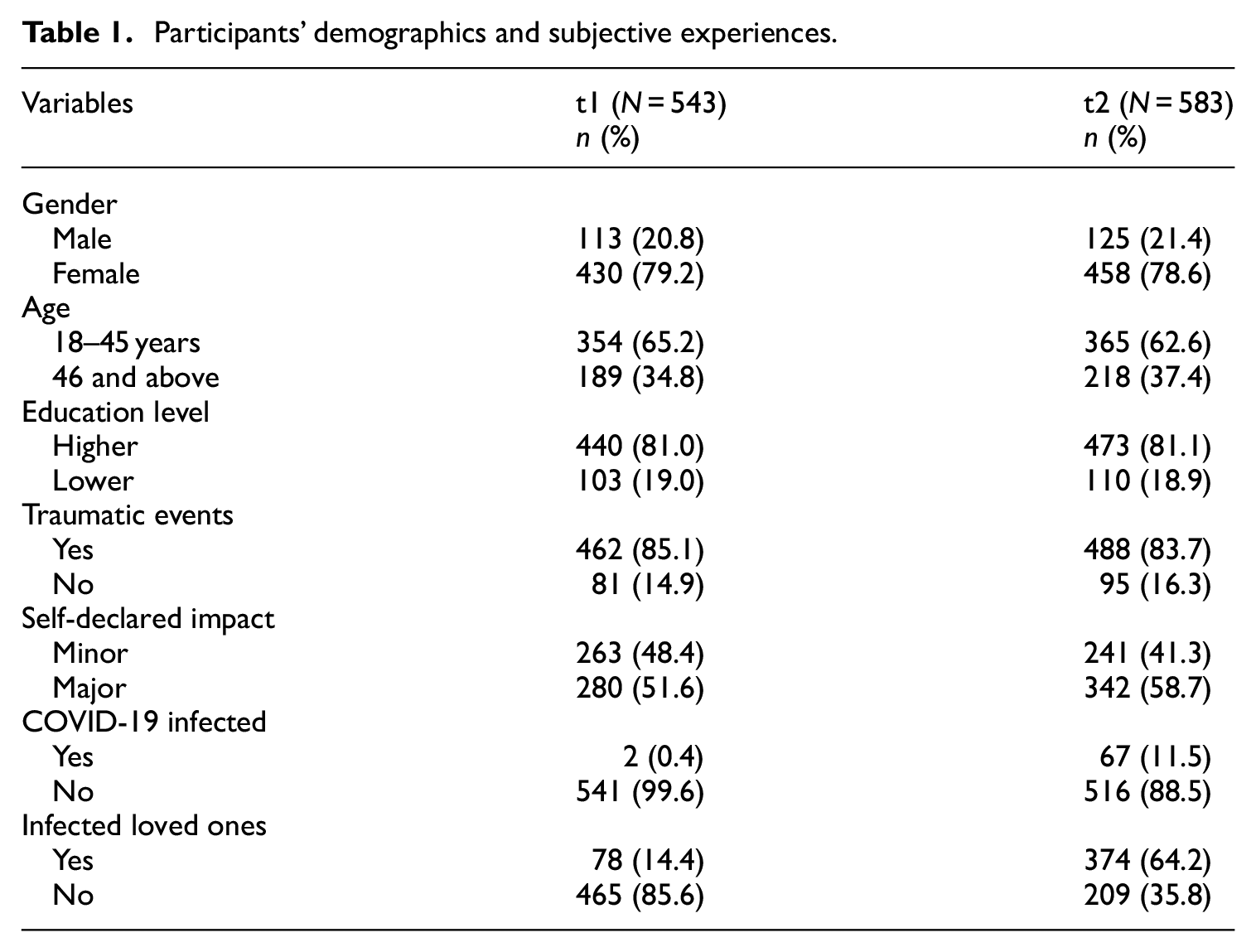
Overall, 888 (78.9%) participants were female, and 238 (21.1%) were male. The latest census conducted in 2018 revealed that the Romanian population comprised 48.9% males and 51.1% females. Nevertheless, the primary reason for the high gender disparity in the sample is the higher likeliness of women to self-select and participate in online surveys, which has been reported in a previous study. 31 Similarly, several other studies, examining the psychological impact during the pandemic, have reported unequal gender proportions.1,4,5,7,9 However, the proportional similarity in the two surveys and the bootstrap statistical analysis validate the results obtained from the current study sample.
The distribution throughout the first three age groups was approximately equal: 18–35 years (29.8%), 36–45 years (34%), and 46–65 years (33.5%). People over the age of 65 accounted for 2.7% of the sample. Responses to the age variable were dichotomized, with 18–35 years and 36–45 years categorized as “younger age” and 46 and above as “older age.” This age dichotomization follows the Behavioral Risk Factor Surveillance System age standardization 32 and the International Consortium in Psychiatric Epidemiology age adjustment to conduct cross-national comparative studies on the prevalence and correlation of mental disorders. 33
More than four in five participants (81.1%) had an associate’s or a bachelor’s degree (higher level) and 213 (18.9%) had a high school diploma only (lower level).
Subjective experiences
The response “no traumatic events” was reported by 176 participants (15.6%), “a few” by 655 (58.2%), and “many” by 295 (26.2%). These responses were dichotomized, with “a few” and “many” categorized as “yes” and “no traumatic events” categorized as “no.”
“Normal–light” impact of the COVID-19 pandemic was reported by 504 participants (44.8%), “moderate” by 475 (42.2%), “severe” by 137 (12.2%), and “extreme” by 10 (0.9%). These responses were dichotomized, with “moderate,”“severe,” and “extreme” categorized as “major” and “normal–light” categorized as “minor.”
In total, 69 (6.1%) participants reported having been infected with COVID-19 themselves, and infected loved ones were reported by 452 participants (40.1%).
The demographics and subjective experiences of all participants are presented in Table 1.
Participants’ demographics and subjective experiences.
Anxiety
Sum scores for anxiety ranged from 0 to 67 (Mean [M] = 31.11, Standard Deviation [SD] = 11.92). According to the IPAT Anxiety Scale, 25 for male participants, sum scores of 0–36 were considered normal, 37–45 moderate, 46–49 severe, and above 50 extremely severe. However, for female participants, sum scores of 0–40 were considered normal, 41–49 moderate, 50–53 severe, and above 54 extremely severe. IPAT offers a different scoring pattern based on gender because the level of anxiety is generally higher and growing among women. 25 The scores were dichotomized, with moderate, severe, and extremely severe categorized as anxious and all others categorized as not anxious.
Depression
Sum scores for depression ranged from 0 to 21 (M = 4.08, SD = 4.09). According to BDI, 26 sum scores below four were considered normal. Sum scores of 4–7 were considered mild, 8–15 moderate, and above 15 severe. Scores obtained on this scale were dichotomized, with moderate and severe depression categorized as depressed and all others categorized as not depressed.
Dissociation
Sum scores for dissociation ranged from 0 to 83.93 (M = 17.33, SD = 16.53). We established interval classes for the sum scores of this variable because they were not determined. Using the normal distribution hypothesis, we followed a normalization procedure to distinguish five classes: very low, low, medium, high, and very high. These five classes were dichotomized, with high and very high (M > 27) categorized as dissociated and all others categorized as not dissociated.
Comparative results
Mean scores and standard deviation for anxiety, depression, and dissociation between the first and second time points and the independent sample t-test results are presented in Table 2. No statistical differences were found for any of the measured variables.
Measures of anxiety, depression, and dissociation at 2 months after the lockdown declaration (t1) compared to 6 months after (t2).

CI: confidence interval; df: degrees of freedom; M: mean scores; p: probability value; SD: standard deviation; t: t-test for correlation coefficient; t1: first survey; t2: second survey.
We believe that the comparison of the results is more relevant from a clinical perspective. Overall, at t1, 23.76% of the participants were anxious, 19.15% depressed, and 32.60% dissociated. After 6 months (t2), 25.73% of the participants were anxious, 17.84% depressed, and 29.67% dissociated.
Table 3 presents the distribution of demographics, anxiety, depression, and dissociation at the first and second time points, expressed in percentages.
Distribution of demographics, anxiety, depression, and dissociation in the first and second time points (percentages).

MP: measurement point (t1: first survey, t2: second survey).
Between the two measurements, there were some minor differences in the number of participants with clinically relevant scores categorizing them as anxious, depressed, or dissociated. The Chi-squared tests showed no statistically significant differences between t1 and t2 for the number of participants with clinically relevant scores: at t1, 129 participants (23.8%) were anxious, 104 (19.2%) were depressed, and 177 (32.6%) were dissociated. At t2, 150 participants (25.7%) were anxious (χ2 (1) = 0.58; p = .44), 104 (17.8%) were depressed (χ2 (1) = 0.32; p = .57), and 173 (29.7%) were dissociated (χ2 (1) = 0.75; p = .38).
However, important differences were observed for gender. Between t1 and t2, anxious males decreased by 8.1%, while anxious females increased by 4.8 percentage points. These differences were not statistically significant (corrected by bootstrap method, 1000 samples): for males at t1, n = 32 (28.31%) and at t2, n = 25 (20.20%), χ2 (1) = 2.25; p = 0.13); for females at t1, n = 97 (22.55%), and at t2, n = 125 (27.29%), (χ2 (1) = 2.65; p = 0.10). Although not statistically significant, this trend was noted because the self-declared impact results validated it.
The number of participants who reported a major impact between the two measurements increased by 7.1 percentage points, which was statistically significant: at t1, n = 280 (51.6%) and at t2, n = 342 (58.7%), (χ2 (1) = 5.72; p = .02). The highest increase (of 9.1%) was observed among women: at t1, 219 (50.9%) and at t2, 275 (60.0%), (χ2 (1) = 7.46; p = 0.006).
Between t1 and t2, infected people increased from 2 (0.4%) to 67 (11.5%). People with infected close relatives increased from 78 (14.4%) to 374 (64.2%). There was also an increase in the proportions of anxious (7.0%) and depressed (5.4%) individuals in this category.
Socio-demographic and subjective experiences associated with anxiety, depression, and dissociation
Binary logistic regressions were conducted to identify socio-demographic factors associated with anxiety, depression, and dissociation (see Table 4).
Results of binary logistic regression estimating the odds ratios of anxiety, depression, and dissociation.

CI: confidence interval; OR: odds ratio.
Statistically significant at p-value < 0.05 regression with and without bootstrap (results are based on 1000 bootstrap samples).
Statistically significant at p-value < 0.05 only bootstrap (results are based on 1000 bootstrap samples).
Results from the two surveys were similar. Anxiety correlated with three of the six independent variables studied. Younger people and those with a lower education level were likely to be about two times more anxious than older and more highly educated respondents. Respondents who had experienced traumatic events were likely to be two and a half times more anxious than those who had not experienced trauma.
Younger people and those who had experienced traumatic events were likely to be more than twice as depressed as older respondents and those with no history of trauma.
Dissociation showed the biggest difference between the two surveys, as seen in Table 4. At t1, those with a lower education level were likely to be more than one and half times more dissociated than highly educated respondents. Those who had experienced traumatic events were likely to be two and a half times more dissociated than those who had not. However, at t2, those with a higher education level were likely to be more than one and a half times more dissociated than less educated respondents.
Mental health predictors
Multiple regression analysis was performed to examine the effect of different measured variables on mental function. For this purpose, anxiety and depression were chosen as the dependent variables, while dissociation was considered an independent variable. The bootstrap method was employed as a modern solution to simplify multiple linear regression analysis. 34 Bootstrap methods improve the reliability of the prediction model and prevent biases generated by a small sample size; additionally, the failure to comply with some of the conditions imposed by the linear model, 35 such as the normality assumption are overlooked by this method. In this analysis, the bootstrap results are based on 2000 bootstrapped samples.
Multiple linear regression analysis indicated that there was a collective significant effect of gender, age, psychological impact, traumatic events, and dissociation, on anxiety at t1 (F(1, 537) = 82.52, p < .001, R2 = .24). Further examination of the of individual predictors revealed that gender (B = −2.25, p < .05, CI [−4.44, −.06]), age (B = −1.18, p = .03, CI [−2.23, −.13]), psychological impact (B = 3.46, p < .001, CI [2.08, 4.80]), traumatic events (B = −3.60, p = .01, CI [−6.20, −.98]), and dissociation (B = .25, p < .001, CI [.19, −.30]), were significant predictors in the model. The results at t2 were similar.
Similarly, multiple linear regression analysis with depression at t1 indicated a collective significant effect of age, psychological impact, traumatic events, and dissociation (F(1, 538) = 38.59, p < .001, R2 = .21). Upon further examination, the individual predictors of age (B = −.59, p = .01, CI [−.95, −.23]), psychological impact (B = 1.63, p < .001, CI [1.17, 2.10]), traumatic events (B = −1.49, p < .001, CI [−2.29, −.64]), and dissociation (B = .58, p < .001, CI [.38, .79]) were found to be significant predictors in the model. However, despite similar results for the rest of the model at t2, the results reported an additional predictor of gender at t2 (B = −.99, p < .01, CI [−1.74, −.25])
Discussion, limitations, and future research
Principal findings
To the best of our knowledge, this is the first repeated cross-sectional study to examine the disassociation levels in an adult sample and the mental health status of Romanians during the global crisis of COVID-19 pandemic.
First, the results showed that, although the number of confirmed COVID-19 cases increased sharply between the first and second survey administrations, there were no significant changes in the mean anxiety, depression, and dissociation scores over the 6 months. Although there were some changes over the 6 months in the number of participants reporting symptoms above the clinical threshold on the anxiety, depression, and dissociation scales, the differences were not statistically significant. Our findings showed that the number of participants with moderate or severe anxiety or depressive symptoms remained mostly unchanged throughout the 6 months. These results are consistent with a recent longitudinal study on mental health in Austria during COVID-19. 36
Both surveys showed the following:
Approximately one in four respondents (t1 = 23.8% and t2 = 25.7%) experienced moderate to severe levels of anxiety symptoms. This is consistent with previous research in other countries showing the proportion of adults who reported moderate to severe levels of anxiety during lockdown: 21% in the UK, 11 28.8% in China, 5 28.8% in the Philippines, 8 and 28% in India. 6
Approximately one in five respondents (t1 = 19.2% and t2 = 17.8%) experienced moderate to severe levels of depressive symptoms. These results are consistent with those collected by the Office for National Statistics data for the UK adult population in June 2020, 37 suggesting that 19.2% of adults reported moderate to severe levels of depression, and 18%–20% in Austria. 36
Approximately one in three respondents (t1 = 32.2% and t2 = 29.7%) experienced high or very high levels of dissociative symptoms.
Approximately one in two respondents suffered from either anxiety, depression, or dissociation (t1 = 46.0% and t2 = 46.7%) and reported being very affected, indicating a major negative impact of the pandemic (t1 = 51.6% and t2 = 58.7%). These data suggest that slightly over half of the population has been negatively affected during the pandemic. These results are consistent with previous research on the first months of lockdown. For example, a study of the Chinese population 5 found that 53.8% of respondents rated the outbreak’s psychological impact as moderate or severe. In the US, a Kaiser Family Foundation poll found that 53% of American adults reported that their mental health had been negatively impacted by worry and stress. 3
Second, our study highlighted predictions for mental health effects and possible trends. Gender was reported as a good predictor for mean symptom values (anxiety to t1 and t2, depression to t2), but not clinically relevant values. However, the findings indicated an increase and decrease of number of anxious people among women and men, respectively. Furthermore, women reported a statistically significantly higher negative psychological impact between the two surveys. Moreover, women’s mental health status was alarming, 6 months after the end of the lockdown, with 60% of them reporting a significant impact; approximately one in three women (27.3%) suffered from clinical anxiety, while one in five (19.4%) suffered from clinical depression. Therefore, our findings suggest that women are much more affected than men, especially in the long term. Men may have adapted better than women during the pandemic because women shoulder most of the extra burdens imposed by the pandemic and associated lockdowns, such as overseeing children’s online schooling, caring for aging parents or other infected family members, and higher loss of jobs than men due to the pandemic. 38 Several other studies reported a more significant psychological impact of the lockdown among females, in the form of higher levels of stress, anxiety, and depression.4,5,39,40 However, studies conducted prior to the pandemic reported that women show consistently higher prevalence rates for anxiety disorders.41–44 Furthermore, women also show higher prevalence rates for depressive disorders than men. 45
Our findings identified age as a predictor of developing clinical mental health symptoms during the pandemic. Young adults were twice as affected by the pandemic and lockdown compared to older adults. This finding is consistent with an Irish study that reported that young people were more vulnerable during the pandemic period. 13
Education level was identified as a clinical predictor of negative effects on mental health, but not as a predictor of mean values. Respondents with lower education levels proved to be almost twice as anxious (at t1 and t2) and depressed (at t1) than those with higher educational levels.
The self-reported psychological impact was also found to predict negative effects on mental health. This psychological impact is believed to be a measure for each respondent’s perception and interpretation, whereby a negative perception and interpretation can lead to increased anxiety and depression levels. For example, Lazarus 46 argued that individual interpretation and perception are more important than the event itself in forming reactions to stress.
A history of previous traumatic life events was the most potent predictor for developing clinical symptoms as well as for mean values of anxiety and depression during the pandemic. Respondents who reported previous traumatic events were two and a half times more likely to experience clinical symptoms than those with no previous traumatic events. This result is consistent with psychological theories asserting that traumatic stress makes those affected more vulnerable. 47 Many continue to experience anxiety, which reduces their resilience to subsequent challenging events such as the lockdown.
Third, results regarding the relationship between anxiety and dissociation allowed us to understand respondents’ changes in dissociative symptoms more deeply. Dissociation is a defensive process in which thoughts, emotions, or sensations fail to be included in consciousness and memory. 48 Dissociation reactions mitigate the negative effect of powerful, overwhelming emotional experiences, temporarily reducing anxiety or fear. 49 Although dissociation works in the short term, it is not healthy in the long term. 49 Our results showed a slight increase in anxiety, alongside a small reduction in dissociation at the 6-month interval (t2). This suggests an inverse relationship between anxiety and dissociation over time. It is also important to note the correlation between people with dissociation and self-reported previous traumatic events. At t1, a higher proportion of respondents reporting previous traumatic events had dissociative symptoms compared to respondents with no previous trauma (statistically significant difference: t1, 34.6% and 18.5% at t2, χ2 (1) = 8.19; p = .004). However, at t2, the proportion of respondents with dissociative symptoms nearly equalized across the two categories. Respondents who had experienced traumatic events previously, familiar with this reaction, have shown higher dissociations since the beginning of the pandemic. On the other hand, respondents without any previous experience of traumas developed a significant dissociation over a longer period and not from the beginning. This shows that in case of a traumatic situation, which occurs insidiously and develops continuously and persists over time (perspective for observing the pandemic), the dissociation develops over a longer period. However, as an independent variable in the multiple regression analysis, dissociation predicted anxiety and depression well.
Fourth, despite the considerable increase in confirmed COVID-19 cases, personal experiences with COVID-19 reported by infected respondents or respondents with infected loved ones did not predict anxiety and depression significantly through average or clinical values. Therefore, the extent to which respondents were psychologically affected did not appear to be influenced by the direct effects of the virus. We assume that none of the respondents experienced any severe forms of the COVID-19 disease. However, our results were inconsistent with the findings of a Chinese study, 50 which reported that 10 acutely ill patients, infected with COVID-19, who received treatment in hospital isolation reported higher anxiety and depression levels.
Limitations and future research
This study has some limitations. Although this study did not aim to identify symptom prevalence, its main limitations include self-report data and the generalizability of the results. As a result, the current study findings should not be generalized to the overall population.
First, our non-probabilistic sampling strategy introduced several sources of bias: self-report bias, selection bias, and sampling bias. Consequently, some categories of people were under-represented (e.g. men, individuals with lower education).
Second, this study primarily employed self-reported questionnaires to identify and evaluate psychiatric symptoms, and thereby did not perform a clinical diagnosis. An accurate psychiatric diagnosis is established through a structured clinical interview and functional neuroimaging.51–53 Therefore, this study’s results should only be seen as evaluations of the severity of anxiety and depression symptoms and their trajectories.
Third, the second survey respondents were not the same individuals who responded to the first survey. The anonymous questionnaire made this type of sampling unavoidable.
Fourth, the gender ratio was not representative of the Romanian population. However, this disadvantage was managed by further statistical analysis with the bootstrap method, which validated the research results through multiple resampling.
Finally, we cannot report the severity of anxiety and depression symptoms caused solely by the pandemic crisis without pre-pandemic data.
Despite these limitations, our study provides valuable insights into personal experiences related to mental health during the pandemic and contributes to the limited data available on this topic.
Recommendation
The current study findings are consistent with existing research reporting that large-scale natural disasters are traumatic and produce several immediate and long-term mental disorders. 54 Therefore, it is essential to urgently implement effective measures for supporting the population’s mental health. For this purpose, Romanian state authorities and mental health experts should be focused on creating awareness by disseminating unbiased and accurate knowledge regarding the disease, outlining the correct isolation measures, and supporting individuals psychologically and financially in the present and future. Young people and adults, who have experienced traumatic events in the events, should be able to access interventions, which help them build resilience through the development of more adaptive functioning under psychological distress. Cognitive behavior therapy (CBT) is the most evidence-based treatment for people with mental health problems to reduce psychiatric symptoms, particularly Internet CBT, which could help in preventing the spread of the infection amidst the pandemic.55–57
However, only the end of the pandemic can act as an ultimate tool for improving mental health. For this purpose, international authorities have proposed the solution of population vaccination to increase mass immunization. Thus, it is necessary to vaccinate the intended 67% population to cross the herd immunity threshold. 58 A study conducted in Asian countries among healthcare workers, reported a 95% willingness to get vaccinated, with independent predictions for high perceived pandemic risk and pro-socialness index, and low vaccine harm index. 58
Conclusions
This study compared Romanian adults’ psychological status immediately after the COVID-19 lockdown to their status 6 months later to identify changes in people’s situations and perceptions regarding the pandemic. This study is novel because it evaluates dissociation levels within an adult sample, and it introduces the predictive model of mental health based on self-reported psychological impact, traumatic events, and dissociation.
To conclude, the mental health of Romanian adults was affected both in the initial phase of the COVID-19 pandemic and afterward, particularly in younger adults, those with a lower education level, and those reporting previous traumatic events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.