
Abstract
The COVID-19 has been spreading across the world since December 2019. The pandemic has created tremendous fear of death from infection and awful psychological pressure on healthcare professionals (HCPs). The measures of psychological effects of the COVID-19 outbreak on the Bangladeshi HCPs are unknown. The present study aimed to assess the mental health outcomes of Bangladeshi HCPs and associated risk factors. We conducted this cross-sectional study from July 15 to September 20, 2020. A total of 355 HCPs aged between 20 and 60 years residing in Bangladesh participated in this study. All the participants completed a self-administered questionnaire through Google Forms consisting of socio-demographic characteristics and mental health outcomes. We measure loneliness, depression, anxiety, and sleep disturbance using the UCLA loneliness scale-8, patient health questionnaire-9, 7-item generalized anxiety disorder scale, Pittsburgh sleep quality index. The present study observed the prevalence of loneliness, depression, anxiety, and sleep disturbance among HCPs were 89%, 44%, 78%, and 87%, respectively. The factors significantly associated with the development of mental health problems among HCPs were working environment, economic condition, education level, area of residence, marital status, gender differences, professional category, body mass index, and smoking habit. Moreover, we have seen significant correlations among the different mental health outcomes. In Bangladesh, a large portion of HCPs reported mental health issues during the COVID-19 pandemic. COVID-19 pandemic incredibly impacted the psychological health of Bangladeshi healthcare professionals. Appropriate supportive programs and interventional initiatives might help the HCPs with mental health problems during and after this pandemic.
Keywords
Introduction
Human civilization is continuously facing challenges due to the COVID-19 outbreak with a speedy transmission across the world. 1 Therefore, the world is probably passing the most critical time after spreading the coronavirus in almost all countries. 2 After the alarming level of spread and severity of infection, WHO officially declared the COVID-19 as a pandemic on March 11, 2020.3,4 Major pandemic outbreaks bring many negative impacts on human life and society. 5
Bangladesh reported the first three confirmed COVID-19 cases on March 8, 2020. 6 Like most nations, in Bangladesh, nearly all non-essential human activities were banned by lockdown or restricting movement in the early stage of COVID-19. 7 All the hospitals unexpectedly received thousands of critically infected COVID-19 patients. The authority compelled them to enforce their emergency protocols. 8 Like others, healthcare professionals (HCPs) are more prone to be infected by a coronavirus.9–11 Globally, the COVID-19 pandemic has put the HCPs in an unprecedented situation to make difficult choices and work under intense pressure. 12 From the very beginning, HCPs have been facing enormous problems due to the scarcity of personal protective equipment (PPE), allocation of limited resources to equally severe COVID-19 patients, management of their physical and mental health.13,14 Worldwide, the authorities advised general people to go slow in regular activities and to maintain social distancing to minimize the risk of infections. However, the HCPs had to go the opposite direction to serve the nations. 14 The HCPs have been attending a long job shift with limited facilities due to the rapid increase in their demand to manage the pandemic. 15 Also, many physicians were unprepared to deal with the new virus. Till now, many things are unknown about it, and there is no well-established therapeutic approach. 16 In this situation, the fear of getting infected, carrying the virus to family members, friends, or colleagues were the major mental health issues for each HCPs.9,17 Also, there is a reported suicide case of patients from the hospital due to the treatment negligence in Bangladesh. Because the nurses and doctors suspected the person might be COVID-19 positive, they did not want to get infected. 18 This fear of infection and transmission of the virus may lead the HCPs to be isolated from their family members, changed their routine, and reduced their social support network. 16
There are many limitations in Bangladesh to deliver healthcare services during this pandemic. 19 Therefore, the COVID-19 pandemic discovers several loopholes in the healthcare system, including a limited number of testing and isolating, inadequate quarantine of the mass people, the weak infrastructure of the healthcare system, insufficient PPEs, etc. 20 In Bangladesh, the infection and mortality rate of the physician is high. The possible reasons behind this may be the lack of infection control techniques, inadequate training to deal with COVID-19 patients, inappropriate use of PPEs, the patient’s tendency to hide information, etc. 21 The above factors had created fear among all HCPs treating COVID-19 or non-COVID-19 patients in Bangladesh. This fear of getting coronavirus infection might develop mental health problems among them.
The COVID-19 pandemic might trigger mental health problems among the general population as well as HCPs.22,23 Loneliness is associated with poor physical and mental health and higher mortality risk.24–29 Till to date, the effective ways to limit the viral spread are frequent hand washing, use of face masks, lockdown, quarantine, and social distancing. 30 But adopting social distance in daily life contradicts the deep-rooted human nature to be connected with others and therefore brings about the feeling of loneliness. 31 As the HCPs are always in close contact with the COVID-19 patients, this may make them a super spreader of coronavirus. 32 Therefore, self-isolation and quarantine from family members are frequent for them. These factors due to the HCP’s nature of profession may create additional psychological pressure on them. 33 Besides other health problems, several cross-sectional studies reported poor sleep quality among lonely people.34–37 Both loneliness and poor sleep quality impacted the mental health of HCPs. 38 Compare to non-clinical staff, frontline medical staff are 1.4 times more likely to feel fear of infection and twice more likely to suffer from anxiety and depression. 39 Therefore, the frontline fighters of the COVID-19 pandemic are more susceptible to develop mental health problems than others. In developing countries, the healthcare system is already overburdened. These flooded COVID-19 cases are likely to induce anxiety, depression, and stress among the HCPs. 40 The situation became worse due to the inadequate supply of essential hand hygiene tools and insufficient PPEs to HCPs.21,41 Evaluation and preserving the mental health of HCPs are the key to manage any pandemic situation. 42 As frontline fighters in the COVID-19 battle, HCPs cannot deny their duties and responsibilities. From the very beginning, Bangladeshi HCPs are fighting with COVID-19 under tremendous pressure. However, the authority has paid little attention to their mental health. 43 Therefore, the present study aimed to evaluate the mental health outcomes of Bangladeshi HCPs during the COVID-19 pandemic assessing loneliness, depression, anxiety, and sleep disturbance.
Method
Study participants
Here, we assumed the response rate, confidence level, and margin of error as 50%, 95%, and 5%, respectively. Based on this assumption, we required 385 responses to achieve a minimum of 80% statistical power. Initially, we collected a total of 386 responses. After screening, we excluded 31 responses due to partial or incomplete information. Finally, we included the responses from 355 HCPs (106 physicians, 77 pharmacists, 91 nurses, and 81 medical technologists) aged between 20 and 60 years in the analysis. All the participating HCPs were of Bangladeshi ethnicity and residing in Bangladesh at that time. We collected responses from all HCPs working in Bangladesh who were willing to participate in this survey. Exclusion criteria were any previous history of psychiatric disorders, neurological disease, acute medical conditions, or the presence of any chronic diseases. All the participants voluntarily provided their information.
Data collection tools
We collected the responses from the HCPs using the google survey tool (Google Forms) from July 15, 2020, to September 20, 2020. Also, we sent the link of the questionnaire to the participants through e-mail, Facebook, Messenger, WhatsApp, Instagram, etc. We designed a self-administered questionnaire covering informed consent, mental health assessment scales, and information about socio-demographic characteristics. We provided support through video conferences or phone calls to resolve the raised doubt or for the proper understanding of the questionnaire.
Socio-demographic measures
A predesigned structured questionnaire was used as a pilot to record the socio-demographic characteristics of the respondents. The socio-demographic features included the category of HCPs, age, gender, body mass index (BMI), religion, marital status, level of education level, working place, economic status, residence, living condition, and smoking history.
UCLA loneliness scale
We applied the short form of the UCLA loneliness scale (ULS-8) containing eight questions to measure loneliness. 44 Each question had a maximum of four points based on the responses. The total score of the ULS-8 scale ranges from 8 to 32. The higher score represents the high degree of loneliness. An individual’s total ULS-8 score from 8 to 16, 17 to 21, 22 to 26, and 27 or more suggests no, mild, moderate, and severe loneliness, respectively.45–47
Patient health questionnaire
The patient health questionnaire-9 (PHQ-9) contains nine questions to assess the depression status of the respondents for the last 2 weeks. Here, each question scored from 0 to 3 points based on the responses. The total score on the PHQ-9 scale ranges from 0 to 27. The higher scores indicate the presence of more severe depression. 48 A total score below 10, 10–15, 16–21, and 22–27 represents no, mild, moderate, and severe depression, respectively. 47
The generalized anxiety disorder scale
The 7-item generalized anxiety disorder scale (GAD-7) contains seven questions to evaluate how often an individual is bothered by each of the seven features in the last 2 weeks. The total score of the GAD-7 scale ranges from 0 to 21, where a higher score indicates a high degree of anxiety.48,49 Based on the responses, each question may contribute up to four points. The total score below 5, 5–9, 10–14, and 15–21 indicate no anxiety, mild, moderate, and severe anxiety, respectively. 47
Pittsburgh sleep quality index
We used the Pittsburgh sleep quality index (PSQI) to assess the sleep quality in the last month. PSQI contains nineteen specific questions from seven different domains. Each domain score ranges from 0 to 3. The total final score ranges from 0 to 21. The higher total PSQI score indicates poor sleep quality. The total PSQI score below five and above five indicates no sleep disturbance and poor sleep, respectively.47,50,51
Statistical analysis
We performed all statistical analyses using a statistical package for social sciences (IBM SPSS, version 25.0) and Microsoft Excel 2016. After data sorting, editing, coding, classification, and tabulation, we imported the excel file into IBM SPSS software for further analysis. We applied descriptive statistics to analyze the characteristics of the respondents. Also, we conducted chi-square tests to associate between the mental health outcomes and related factors. The binary logistic regression analysis showed the relationships between the risk factors and psychometric measurements.
Results
Characteristics of the respondents
We demonstrated the socio-demographic characteristics of the respondents in Table 1. In total, 355 HCPs (physicians: 106, pharmacists: 77, nurses: 91, and MT: 81) participated in this study. Among them, males and females were 57% and 43%. Two-thirds of the participants were within 20–40 years of age. The majority of the respondents were married (77%), non-smoker (73%), lower economic class (72%), urban people (76%), and living with family (74%). Two-third of the HCPs working in a hospital or clinic had a graduate or higher level of education.
Distribution of variables and their association with different mental health problems among the healthcare professionals.
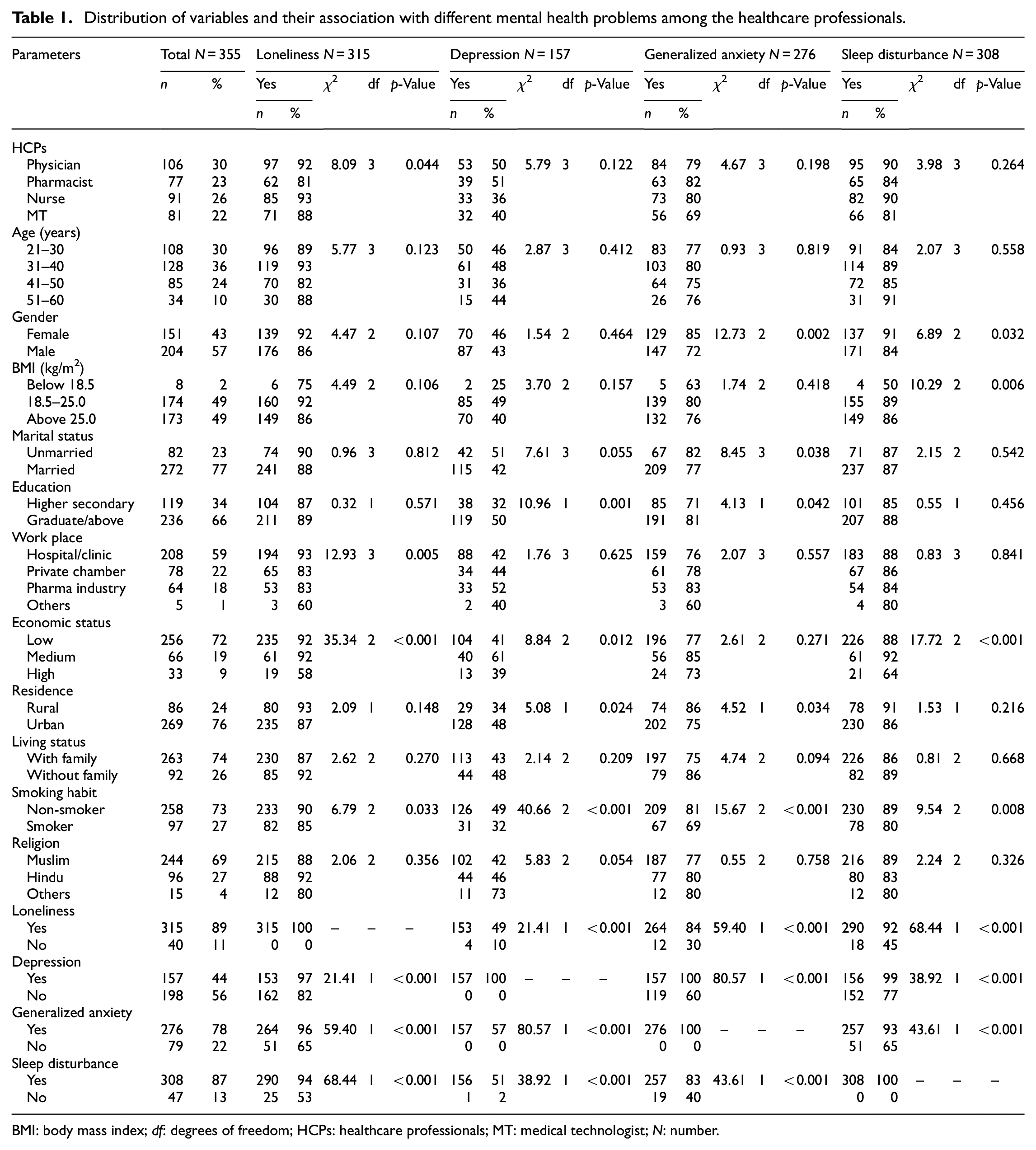
BMI: body mass index; df: degrees of freedom; HCPs: healthcare professionals; MT: medical technologist; N: number.
Psychometric parameters
The estimations of loneliness, depression, anxiety, and sleep disturbance were 89%, 44%, 78%, and 87%, respectively. (Figure 1 and Table 1). The high prevalence loneliness was observed in (i) physicians versus pharmacists (92% vs 81%, p = 0.044), (ii) hospitals or clinics versus other working places (93% vs 60%, p = 0.005), (iii) medium versus high economic background (92% vs 58%, p < 0.001), (iv) with versus without depression (97% vs 82%, p < 0.001), anxiety (96% vs 65%, p < 0.001), and sleep disturbance (94% vs 53%, p < 0.001). The frequency of having depression were higher in (i) individuals with higher education versus lower education (50% vs 32%, p = 0.001), (ii) medium versus high economic status (61% vs 39%, p = 0.012), (iii) residing in urban versus rural area (48% vs 34%, p = 0.024), (iv) non-smoker versus smoker (49% vs 32%, p < 0.001), (v) with versus without having loneliness (50% vs 10%, p < 0.001), anxiety (57% vs 0%, p < 0.001), and sleep disturbance (51% vs 2%, p < 0.001). Similarly, HCPs were more prone to have anxiety in (i) females versus males (85% vs 72%, p = 0.002), (ii) unmarried versus married (82% vs 77%, p = 0.038), (iii) higher education versus lower education (81% vs 71%, p = 0.042), (iv) rural versus urban area (86% vs 75%, p = 0.034), (v) non-smoker versus smoker (81% vs 69%, p < 0.001), (vi) with versus without significant loneliness (84% vs 30%, p < 0.001), depression (100% vs 60%, p < 0.001), and sleep disturbance (83% vs 40%, p < 0.001). And, finally the sleep disturbance was higher among (i) females versus males (91% vs 84%, p = 0.032), (ii) medium versus high economic class (92% vs 64%, p < 0.001), (iii) non-smoker versus smoker (89% vs 80%, p = 0.008), (iv) with versus without considerable loneliness (92% vs 45%, p < 0.001), depression (99% vs 77%, p < 0.001), and anxiety (93% vs 65%, p < 0.001).
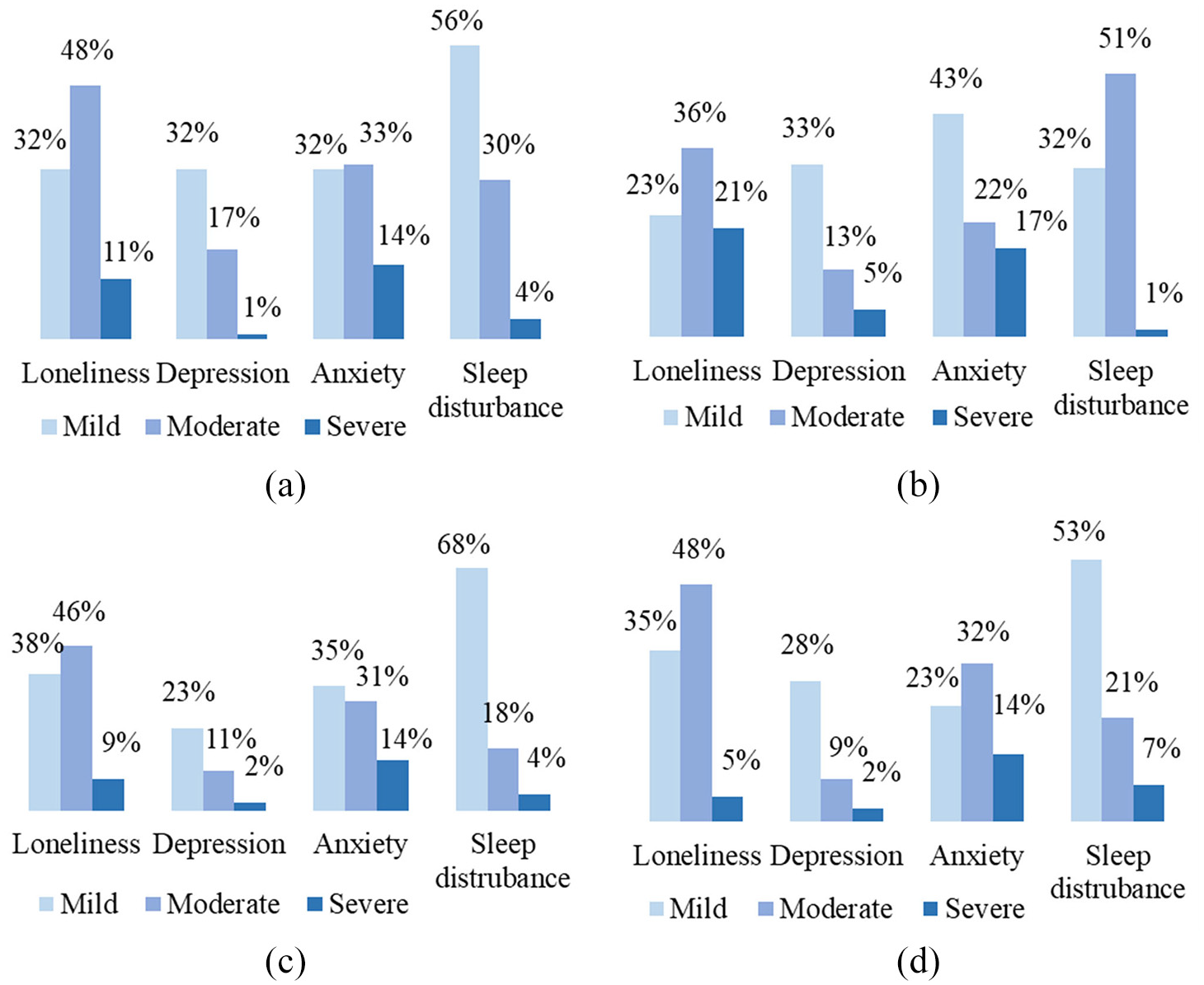
Prevalence of mental health problems among the healthcare professionals based on the severity: (a) physician, (b) pharmacist, (c) nurse, and (d) medical technologist.
Regression analysis
The relationships between dependent variables and independent covariates were estimated using the binary logistic regression model (Table 2). The probability of having loneliness among Bangladeshi HCPs was 13.80 times more in the higher education group than low education group, 39.90 times higher in the low-economic class than high economic class, 43.02 times higher in the medium financial status than the high economic background, 9.25 times higher in respondents with anxiety disorders, and 5.58 times higher in the respondents with sleep disturbance, respectively. We observed the possibilities of having depression were 4.01 time higher in pharmacists than other HCPs, 2.62 times more with high academic qualification than the low educational background, 0.29 times lower in rural respondents than urban, 0.15 times lower in the respondents who were living with family than who were not living with family, 8.53 times higher in non-smoker than a smoker, 23.81 times more in the respondents with sleep disturbance. The likelihoods of having anxiety among HCPs were 16.51 times higher in females than males, 0.21 times lower in HCPs who were working in hospitals than other places, 0.07 times lower in the low economic background than high economic class, 0.048 times lower in medium economic class than high economic class, 5.43 times higher in rural residents than urban, 0.33 times lower in non-smoker than a smoker, and 22.22 times higher in the respondents with loneliness, respectively. The chances of having sleep disturbance in HCPs were 0.03 times lower in females than males, 10.80 times higher in the low BMI group than normal BMI group, 8.43 times more in low economic class than high economic group, 3.80 times higher in rural respondents than urban group, 7.35 times more in those who already have loneliness, and 33.33 times more in the respondents with depression, respectively.
Regression analysis of variables by mental health problems among the healthcare professionals.

BMI: body mass index; CI: confidence interval; HCPs: healthcare professionals; MT: medical technologist; N: number; OR: odds ratio.
Discussion
The present study is one of the first-ever studies assessing the mental health outcomes of Bangladeshi HCPs due to the COVID-19 pandemic. We carried out this study among physicians, pharmacists, nurses, and medical technologists working in Bangladesh to ensure healthcare service during this pandemic. In the present study, a lion share of HCPs working in different hospitals, clinics, and private chambers reported their mental health problems. Many of them suffer from loneliness, depression, anxiety, and sleep disturbance as they are continuously serving COVID or non-COVID units of hospitals under extensive mental pressure. We observed the high prevalence of loneliness in physicians working at hospitals or clinics with medium economic background. Moreover, we observed higher loneliness levels among the HCPs with or without depression and anxiety. The depression was higher in HCPs with medium financial status residing in the urban area. Similarly, the anxiety level was higher in unmarried female HCPs. Also, the medium economic class female HCPs reported a higher sleep disturbance who already had loneliness or depression. Everyone is susceptible to psychological disorders during any pandemic situation. Moreover, the HCPs are more prone to be affected by mental health problems. 52 The possible reason for their diminished mental health is the isolation from family members, the risk of carrying viruses, and the continuous fear of getting infected.53,54 Increased social isolation, quarantine time, social distancing, and loneliness are the adverse consequences of the COVID-19 pandemic that are significantly associated with depression, anxiety, sleep disturbance, self-harm, and suicide attempts.55,56 Primary health care workers who are in direct contact with the known COVID-19 patients or suspected COVID-19 patients are the most susceptible to be infected by the virus.16,57 The HCPs have to provide service for more work shifts due to increased demand for healthcare needs with limited resources, 15 keeping PPEs on the body for such a long period that may cause difficulty in breathing, physical discomfort, and mental health burden. 16
Moreover, we observed a connection between mental health problems of HCPs with gender difference, level of education, smoking habit, job role, area of residence, economic background, and working environment. Many recent study findings are consistent with the present survey outcomes. A recent study among nurses and physicians working at COVID-19 units reported high levels of stress, anxiety, and post-traumatic stress disorder. 58 The possible reasons behind this might be the long working period, direct contact with the COVID-19 patients, fear of infection, and tension. Another study revealed that physicians’ social support level was positively associated with sleep quality. 59 A study among nurses in China found that one-third of the frontline nurses suffered from depression, anxiety, and sleep disturbance during the COVID-19 pandemic that showed consistency with the current findings. 52 The present study findings are consistent with the results of similar past studies.13,60 According to a meta-analysis including 13 cross-sectional studies where a total of 33,062 HCPs reported significantly elevated levels of anxiety, depression, and sleep disturbance during the COVID-19 pandemic. 61 About half of the HCPs suffering from depression, anxiety, and sleep disturbance in China than any other occupation or general population with similar age groups. 62 In Bangladesh, insufficient PPEs, intense workload, fear of getting the infected lead to physical tiredness, anxiety, depression, and sleep disturbance among HCPs. 63 The psychological response of HCPs to a pandemic may depend on different factors that may affect their mental health to cause depression, anxiety, loneliness, sleep disturbance.57,64 Therefore, the authority should implement comprehensive guidelines to evaluate and manage the mental health issues of the HCPs for ensuring the proper treatment of COVID-19 patients.
The present study has few limitations. There might have a possible bias in recruiting the participants since we used an online survey due to the COVID-19 pandemic. The online investigation using Google Form may not be the best method for data collection. However, we took it as a safe and effective tool during the pandemic situation. And finally, the self-report assessment might not be consistent with the clinical diagnosis.
Conclusion
The world is currently fighting the public health issues in this COVID-19 pandemic. We assessed mental health problems among HCPs in the present study. Here, a large proportion of HCPs in Bangladesh reported different mental health problems during the COVID-19 pandemic. The consequences of the mental health problems of HCPs may impose a prolonged negative impact on the total healthcare system. Therefore, the authority should give more attention to the mental health issues of Bangladeshi HCPs during this pandemic. This study results may help in identifying HCPs who are at greater risk of mental health problems. Mental health support programs, providing adequate quality PPEs, decreasing workload, introducing remote healthcare services, and providing essential infection control training might reduce the impact of COVID-19 on mental health among HCPs. We recommend further longitudinal studies to find the actual associations between mental health issues of HCPs and COVID-19-related factors.
Footnotes
Acknowledgements
The authors would like to thank the participants for their cooperation to conduct this study.
Author contributions
MAUR, SAP, SQ, and MRI: Conceived the idea and involved in the design of the study. MAUR, SAP, and SQ: Coordinated for the data collection. RD and SD: Analysed the data and drafted the manuscript. MRI: Reviewed the manuscript for important intellectual content, edited the manuscript, and supervised the whole work. All the authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was self-funded.
Ethics approval and consent to participate
This study was approved by the ethical review committee of the department of psychiatry, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. We briefed about the objective of the study and written consent was taken from each participant.
Consent for publication
We obtained written permission from all the study participants or their legally authorized primary caregivers for the publication of anonymous data in journal articles.
Availability of data
The data supporting the present study findings can be obtained from the corresponding author upon reasonable request.