
Abstract
Making up 13.4% of the United States population, African Americans (AAs) account for 28.7% of candidates who are currently waiting for an organ donation. AAs are disproportionately affected by end-organ disease, particularly kidney disease, therefore, the need for transplantation among this population is high, and the high need is also observed for other solid organ transplantation. To this end, we worked with the AA community to derive an empirical framework of organ donation strategies that may facilitate AA decision-making. We used a cognitive mapping approach involving two distinct phases of primary data collection and a sequence of data analytic procedures to elicit and systematically organize strategies for facilitating organ donation. AA adults (n = 89) sorted 27 strategies identified from nominal group technique meetings in phase 1 based on their perceived similarities. Sorting data were aggregated and analyzed using Multidimensional scaling and hierarchical cluster analyses. Among 89 AA participants, 68.2% were female, 65.5% obtained > high school education, 69.5% reported annual household income ≤ $50,000. The average age was 47.4 years (SD = 14.5). Derived empirical framework consisted of five distinct clusters: fundamental knowledge, psychosocial support, community awareness, community engagement, and system accountability; and two dimensions: Approach, Donor-related Information. The derived empirical framework reflects an organization scheme that may facilitate AA decision-making about organ donation and suggests that targeted dissemination of donor-related information at both the individual-donor and community levels may be critical for increasing donation rates among AAs.
Introduction
Making up 13.4% of the United States population, African Americans (AAs) account for 28.7% of candidates who are currently waiting for an organ donation. 1 Given AAs are disproportionately affected by end-organ disease, particularly kidney disease, 2 AA organ donation rates are lower than Caucasians, 3 therefore, the need for transplantation among this population is high,4,5 and the high need is also observed for other solid organ transplantation.6–8 Despite this need, AAs achieve transplantation at significantly lower rates than their Caucasian counterparts.3,9 Since the new kidney allocation system was implemented in late 2014, the number of transplants among AAs has increased, but known racial disparities in transplant rates persist. 5 Given that racial concordance rates are >95% among donor-recipient pairs,10,11 this disparity has been explained, in part, by lower organ donation rates among AAs. 1 The known barriers for AA organ donation include lack of knowledge, myths about donation, and mistrust of the medical system. 12 However, there is a gap in how AAs view and organize the perceived strategies that facilitate organ donation. Therefore, the utilization of formative research tools to identify strategies for optimal organ donation program development designed to increase organ donation rates among AAs is paramount. Using nominal group technique (NGT), 13 a formative research method, we previously identified knowledge about donation-related risks and the donation process as key facilitators for AAs willingness to donate. 14 While community-driven identification of strategies for improving organ donation rates is critical to the development of interventions to promote organ donation, prioritized strategies do not provide information on how responses are viewed/mapped cognitively.14,15 In other words, prioritized strategies alone do not provide any context for how AAs organize or view those strategies based on perceived similarities and differences.
Cognitive mapping is a patient-centered mixed-method approach that involves a two-phase formal group process and integrates respondents’ input and a sequence of statistical analyses to generate maps that aggregately represent the responses with thematic clusters.16,17 In contrast to other qualitative methods, cognitive mapping helps researchers understand how individuals view and organize responses or how they arrive at a particular decision. Functionally, cognitive maps are internal spatial representations that provide an unconscious framework for decision making; and in their absence organization schemes designed to facilitate decision-making cannot be derived. 18
We, therefore, sought to build on our previous work 14 to better understand how organ donation strategies are represented cognitively through the identification of an organ donation organization scheme that reflects the factors influencing decision-making about organ donation in the AA community. To this end, we used a card sort task and multidimensional scaling 19 along with hierarchical cluster analysis 20 to derive an empirical framework of organ donation strategies that may be used as a basis for the development of interventions aimed at facilitating AA decision-making about organ donation.
Methods
Study design
This research was based on a cognitive mapping approach involving two distinct phases of primary data collection and a sequence of data analytic procedures to elicit and systematically organize strategies for facilitating organ donation. During Phase 1 NGT meetings, AA participants (n = 28) generated and prioritized responses to a single specific question “What would make it easier for people to decide to become organ donors?”. 14 The second phase of the cognitive mapping approach involved a card-sorting and rating task among a cohort of AA participants and a sequence of analyses to understand how responses from Phase 1 were represented cognitively.
Participant recruitment
Card sorting and rating participants were recruited from local AA communities using a snowball approach; 113 potential participants were approached and 89 agreed to participate for a 78.8% participation rate. Inclusion criteria were age ≥18 years, self-defined race as AA, ability to speak and write in English, and cognitive ability to provide consent. Research indicates that as few as 30 card-sorting participants who are reprehensive of the actual population can provide an optimal estimation of the similarity matrix and yield results similar to those of several hundred.21,22 All participants provided written informed consent, and were asked to complete a baseline demographic questionnaire (age, education, income, and attitudes toward deceased and living donation (5-pint Likert scale)). Each participant received a $25 VISA gift card for effort and time. The study received Institutional Review Board approval.
Card-sorting task and rating instrument
Participants sorted a set of 27 index cards, each of which was labeled with a strategy generated from Phase 1 NGT meetings. The NGT methodology and results were published previously. 14 To derive a scheme for organizing organ donation strategies, we developed an open card-sorting task (Q-sort). 17 Each participant was instructed to sort the cards into at least two but not more than 10 piles with a minimum of two cards in each pile based on how he/she perceived the strategies to be similar. The data from each completed card sort task were then aggregated across all participants to form a group co-occurrence matrix. This matrix indicated the number of times that the participants sorted each strategy together with every other strategy and provided data for calculating similarities/distances among all pairs of strategies. For each strategy, participants were asked to indicate whether the strategy would influence their own decision to become an organ donor. Participants used a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree) to assess the potential influence of strategies.
Statistical analyses
Multidimensional scaling
The similarity measures derived from the aggregated group co-occurrence matrix were modeled using nonmetric multidimensional scaling (MDS ALSCAL) based on squared Euclidean distances. 18 MDS analysis was used to model the relative similarities/distances between strategies within a multidimensional space. Specifically, MDS provided relative ordering of strategies along a continuum of more or less, with the interpretive goal of deriving meaning from the ordering of objects along a dimension. 19
The derived MDS solution was evaluated by examining specific goodness-of-fit criteria: (1) S-stress indicated the level of error that results from the discrepancies between the actual distance data (i.e. observed similarities of pairs of strategies) and the modeled representation of those data (i.e. a map of calculated inter-point distances between pairs of strategies); (2) RSQ value represented the extent to which the derived spatial representation of strategies corresponded to the observed similarities in the data. S-stress <0.15 and a RSQ >0.90 indicated excellent goodness-of-fit for the model. 19
Hierarchical cluster analysis
Cluster analysis was used to identify groups or clusters of homogenous strategies.20,21 The MDS results included coordinates defining the location of each strategy within a derived multidimensional space and were used as data for cluster analysis. Results from the combined MDS/cluster analysis are represented geometrically by a map reflecting different aspects of the perceived similarity of facilitative strategies. For our analysis, pairs of strategies perceived as similar (i.e. those frequently sorted together) were represented as points closer together on the map. The derived cognitive map afforded the opportunity to discern both the relative ordering of clusters and the ordering of individual strategies within each cluster along each dimension.
Descriptive analyses, chi-square tests, and independent-samples t-tests were used to characterize the study sample. All analyses were conducted using IBM SPSS 25 (Armonk, NY: IBM Corp.). Statistical significance was set at p < 0.05.
Results
Demographic characteristics and donation-related attitudes
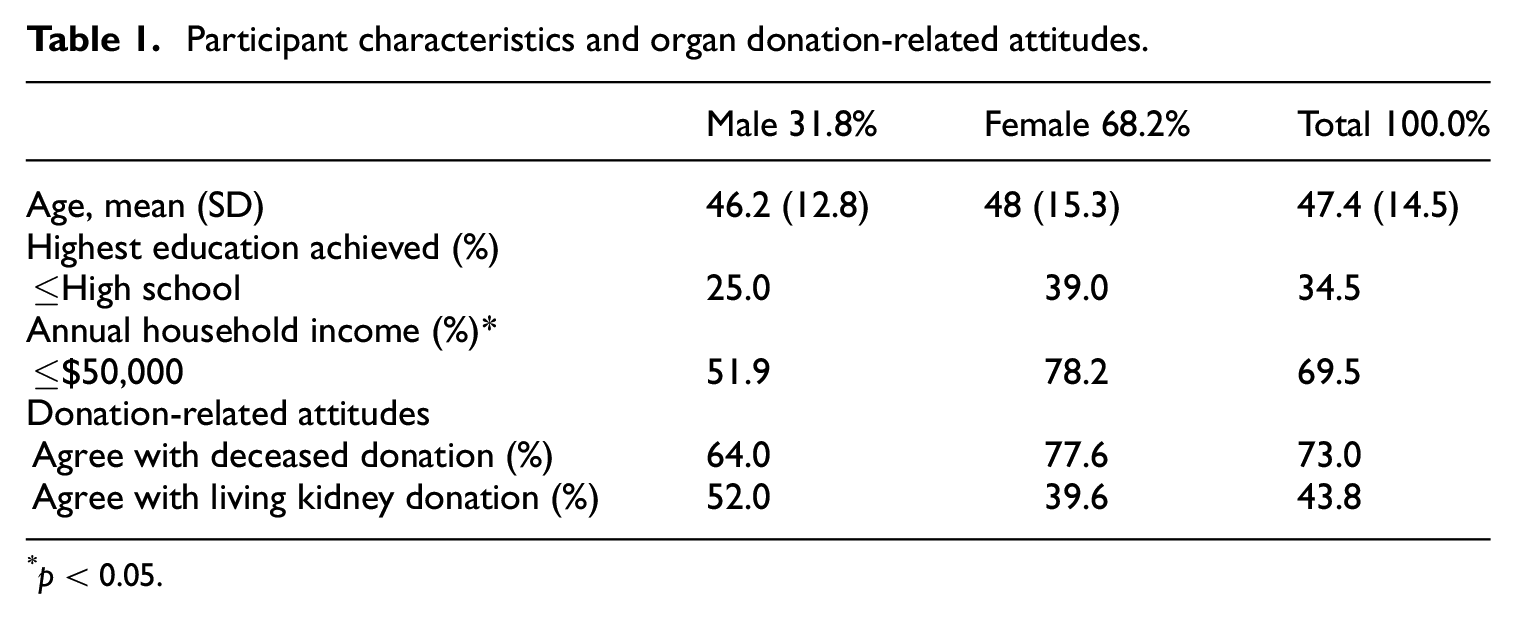
Among 89 AA participants, 68.2% were female, 65.5% obtained > high school education, 69.5% reported annual household income ≤$50,000. The average age was 47.4 years (SD = 14.5), ranging from 18 to 74 (Table 1). Among 73 participants who responded to the two organ donation attitude questions (response rate of 82%), 73% of participants reported agreeing with organ donation after one’s death. In contrast, only 44% of participants agreed with living kidney donation.
Participant characteristics and organ donation-related attitudes.
p < 0.05.
Results from multidimensional scaling
The measures of overall goodness-of-fit for the MDS analysis indicated that a two-dimensional solution provided a better model (S-stress = 0.13, RSQ =0.91) than a one-dimensional solution (S-stress = 0.29, RSQ = 0.76) and was comparable in fit but more interpretable than a three-dimensional solution (S-stress = 0.08, RSQ = 0.96).
The MDS solution can be interpreted by examining how strategies are represented along the horizontal and vertical dimensional axes. Interpretation of the map is facilitated by contrasting the meaning of strategies located at the extremes of each dimension. We interpreted one dimension of the MDS solution as relating to providing “Donor-related Information” about organ donation (Figure 1). The vertical axis (y-axis) was anchored on the top by “Providing information to help people see how big the need is” (strategy 8 in Cluster 1), “Tell people the steps involved in becoming an organ donor to make it easier for them” (strategy 10 in Cluster 1, objective donor-related information about organ donation processes), “Highlight specific types of organ donations that are needed, e.g., like blood-drives and types of blood needed” (strategy 12 in Cluster 3), and “Let people know there are different kinds of organ donation—some organs can be donated while you are alive, some after you pass away” (strategy 27 in Cluster 1). The y-axis was anchored on the bottom by “Help people overcome the fear that paramedics might let them die if they knew they are organ donors” (strategy 25 in Cluster 2), “Support family members who are worried about organ donation” (strategy 18 in Cluster 2, subjective donor-related information about dealing with fear), and “Make sure the medical system can be trusted” (strategy 4 in Cluster 4).

Two-dimensional scatter plot of the cognitive framework utilized by as in the decision-making process about organ donation.
The second dimension, represented on the horizontal axis (x-axis) in Figure 1, was related to facilitative “Approaches” about organ donation, and was anchored at the extremes on the left by responses including “Have workplace program about organ donation” (strategy 16 in Cluster 5) and “Have church elders talk about the importance of organ donation” (strategy 14 in Cluster 5). These are public or community approaches. The x-axis was anchored on the right by “Tell stories about people who have benefited from organ donation” (strategy 17 in Cluster 1), “Tell people about all the pros and cons of organ donation” (strategy 26 in Cluster 1), “Tell people about the chances that the organ donation will be successful—not rejected” (strategy 15 in Cluster 1), and “Tell people that the organs will waste away after they pass away” (strategy 23 in Cluster 2). These are private or individual approaches.
Results from hierarchical cluster analysis
The hierarchical cluster analysis revealed five distinct clusters to which each of the 27 organ donation strategies was assigned exclusive membership. Because there are no assumptions that can be made about the distribution of the data used in this analysis, a subjective decision was made to interpret a five-cluster solution. This decision was informed by examining the pattern and order that strategies joined to form a cluster at different stages and by visually inspecting the graphical representation (tree diagram and icicle plot).
The five clusters resulting from the hierarchical cluster analysis were superimposed on the multidimensional scaling map (Figure 1). An interpretation of the five clusters was made on the basis of the strategies composing each cluster (see individual strategies listed in the Table 2). The five clusters were interpreted to represent: (1) fundamental knowledge, (2) psychosocial support, (3) community awareness, (4) community engagement, and (5) system accountability.
Mean and standard deviation for the Likert scale rating for each strategy and cluster.

The Total N includes participants who did not respond to the question of living donation.
p < 0.05.
Results from rating instrument
Participants’ agreement or disagreement about whether a particular strategy would affect their own decision to become an organ donor are presented in Table 2. Overall, 23 strategies received an average rating score >4. The top five strategies were: (1) Provide facts about organ donation to help people deal with their fears (4.56 ± 0.62); (2) Tell people about all the pros and cons of organ donation (4.51 ± 0.73); (3) Let people know there are different kinds of organ donation—some organs can be donated while you are alive, some after you pass away (4.50 ± 0.72); (4) Talk about the positive sides of organ donation (4.43 ± 0.67); and (5) Let people know that organ donation can really help others (4.41 ± 0.83). The strategy “Pay people or their families for organ donation” received the lowest mean rating value with the largest standard deviation (3.09 ± 1.48) among all 27 strategies. The cluster mean indicated the participants’ average agreement across strategies within each specific cluster. Fundamental knowledge (Cluster 1) was rated as the most influential (4.32 ± 0.57) during the organ donation decision-making process (Table 2).
Participants who agreed with living donation top five rated strategies were: (1) Provide facts about organ donation to help people deal with their fears (4.66 ± 0.55); (2) Let people know there are different kinds of organ donation—some organs can be donated while you are alive, some after you pass away (4.59 ± 0.50); (3) Describe the myths that some people have about organ donation (4.53 ± 0.67); (4) Tell stories about people who have benefited from organ donation (4.53 ± 0.62); and (5) Talk about the positive sides of organ donation (4.50 ± 0.67). Overall, participants who agreed with living donation gave fundamental knowledge (Cluster 1, 4.36 ± 0.48), psychosocial support (Cluster 2, 4.31 ± 0.52), and community awareness (Cluster 3, 4.35 ± 0.53) similar weight in their organ donation decision-making process (Table 2).
Participants who disagreed with living donation top five rated strategies were: (1) Tell people about all the pros and cons of organ donation (4.58 ± 0.71); (2) Provide facts about organ donation to help people deal with their fears (4.49 ± 0.71); (3) Make sure the medical system can be trusted (4.44 ± 1.05); (4) Let people know that organ donation can help others (4.38 ± 0.81), and (5) Let people know there are different kinds of organ donation—some organs can be donated while you are alive, some after you pass away (4.38 ± 0.87). Overall, participants who disagreed with living donation rated fundamental knowledge (Cluster 1, 4.24 ± 0.65) as the most influential during the organ donation decision-making process (Table 2).
Compared with participants who disagreed with living donation, those who agreed with living donation had significantly higher mean ratings in the following individual strategy “Tell stories about people who have benefited from organ donation (4.53 vs 4.07)”, “Have a national organ donor drive day for people to sign up (4.41 vs 3.85),”“Get others who are just like us to provide stories about organ donation (4.38 vs 3.98),”“Have family doctors talk about organ donation during a check-up (3.97 vs 3.44),” and higher cluster mean for the “Cluster 3: Community Awareness (4.35 vs 4.00)” (Table 2).
Discussion
Using a well-validated patient-centered mixed-method approach, we derived an empirical framework consisting of five distinct domains of organ donation strategies that may facilitate AAs decision-making about organ donation. The findings suggest that interventions and systemic change to support AA decision-making about organ donation should utilize an organizing framework based on fundamental knowledge, psychosocial support, community awareness, community engagement, and system accountability. The information solicited from AA community participants suggested that interventions focused on improving knowledge about organ donation were most influential when making decisions about organ donation. This was of particular importance among those participants that disagreed with living donation. More granular cognitive mapping results suggested that knowledge specific to the needs of organ donors was critical to facilitating organ donation within the AA community, representing one extreme of the two-dimensional model. This finding is consistent with a conclusion from a systematic review based on 19 studies. 23
Efforts to better understand lower organ donation rates among AAs have been ongoing since the early 1980’s.24–26 Similar to our findings, a recent study by DuBay et al. 26 found the most important perceived barrier for influencing organ donation among AAs was “lack of information.” However, the primary focus of these studies has been related to donation after death. Little to no attention has been paid to developing educational programming specific to living kidney donation, yet results from our study suggest that donor-specific information may be needed to increase living donation among AAs, such as pros and cons, steps involved in becoming a donor, process of donation, requirements of donor (e.g. age, health condition), long-term safety and outcomes after donation. Expectations and experiences from previous donors may help potential donors. 27 Participants of our study wanted to know “stories about people who have benefited from organ donation” and “Get others who are just like us to provide stories about organ donation. Those participants who agreed with living donation valued more about these two strategies. A newly published research showed that the narratives were slightly more successful than statistics in increasing intention of organ donation. 28
Participants need psychosocial support to overcome fear or myths about organ donation. The strategy of “Provide facts about organ donation to help people deal with their fears” received a high mean rating from participants who disagreed (4.49 ± 0.71) and agreed (4.66 ± 0.55). “Support family members who are worried about organ donation” and “Describe the myths that some people have about organ donation” were also rated by participants as important strategies. In one recent qualitative study conducted with 123 living kidney donors in Australia and Canada, prior donors reported challenges including fears of health, system shortfalls, and lifestyle interference. 27 Existing studies indicate that psychosocial support for potential donors 29 and donors27,29,30 and family 31 are important to facilitate organ donation in all populations, especially in AA population. 3
Smaller studies have described the addition of home-based educational programs to existing clinic-based models to encourage living donor kidney transplantation among AA end-stage renal disease patients. 28 These home-based educational programs included use of minority health educators, brochures highlighting minority transplant recipients and donors, and discussions of race-specific outcomes. Program implementation resulted in increased living donor inquiries and evaluations and living donor transplants early but failed to demonstrate sustained increases.32,33 Importantly, these programs were designed to target transplant candidates, not potential donors. A recent study reported that a community-based organ donation education program for AA adults was successful in improving their attitudes and beliefs, but not effective in changing their negative beliefs about organ donation or registration behaviors. 34 This suggests that only providing information about organ donation may not be enough to facilitate organ donation among AAs. Data gleaned from the AA community and highlighted in our study suggests that interventions such as educational programs may need to provide information specific to potential donors in order to facilitate AA decision-making about organ donation. While multiple efforts to improve organ donation rates among AAs have been made, most have failed to engage the AA community from program inception to implementation. As such it is not surprising that fewer than 15% of AA transplant candidates achieve living donor transplantation, 1 yet AAs comprise 33% of the kidney transplant waiting list. 5 Results from our study highlighted the importance of engaging the community (e.g. workplace program, church elder, family doctors) and increasing community awareness (e.g. organ donation –drive, use of TV ads, communicate about organ donation to younger people, highlight specific types of organ donations that are needed). Interventions with community involvement may have better outcomes to improve organ donation registration among the AA population.
One domain of strategies from our study is system accountability. “Make sure the medical system can be trusted” received the highest mean ratings from participants who disagreed with living donation within the system accountability cluster. Mistrust in the medical system is one of the barriers to organ donation among AAs. Williamson and colleagues conducted a qualitative study to examine organ donation-related medical mistrust beliefs in AAs, and reported that societal distrust, distrust of general institutions, distrust of medical institutions, and organ donation-specific medical mistrust were four categories of medical mistrust beliefs. 35 An intervention including the content of health care systems may improve organ donation-related mistrust in the medical system among AAs. There has been a long-time argument about payment or financial compensation for organ donors.36,37 However, in our study, the strategy of “Pay people or their families for organ donation” received the lowest mean ratings from both disagreed and agreed groups. This suggests that financial incentive alone may not be an effective approach for facilitating organ donation among AAs.
Our formative assessment has several limitations. Because study participants were recruited from local AA communities, their opinions, although valuable, may not be representative of all AAs. Our approach and sample size, however, did allow for an understanding of variations in opinions. 38 In addition, our research focused on organ donation in general. Similar research should be undertaken to identify actual living-donor perspectives on organ donation educational strategies. Living donor-level data reflecting donor views regarding what they perceived as effective or ineffective interventions would likely achieve a more comprehensive/integrated intervention approach for facilitating increases in AA organ donation rates. Lastly, we did not ascertain whether participants were registered donors, and as such, our ability to isolate the perspectives of non-registered potential donors is limited.
Our findings highlight the importance of donor-related information and targeted dissemination of information at both the individual-donor and community levels in the cognitive framework utilized by AAs in the decision-making process about organ donation. Further study is needed to better understand the relationship between the identified cognitive map and participant behavior with regard to donor registration and living donor inquiries.
Footnotes
Authorship
Locke, Reed, Shewchuk, and Qu participated in research design and writing of the manuscript; Locke, Qu, Shewchuk, Reed, Stegner performed the research; Qu, Shewchuk, Reed performed data analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center of Excellence in Comparative Effectiveness Research for Eliminating Disparities (National Center on Minority Health and Health Disparities [NCMHD] Grant 3P60-MD000502) from the National Institutes of Health (NIH) and the Charles Barkley Health Disparities Research Award through the University of Alabama at Birmingham Minority Health and Health Disparities Research Center (NCMHD Grant 5P60-MD000502).