
Abstract
Breast cancer is one the most common malignancies and leading cause of cancer-related mortality in women. Recent studies suggested that hypercholesterolemia may be the potential modifiable risk factors for breast cancer. Cholesterol was well-known for its strong association with cardiovascular disease for long. Moreover, solid evidence has been provided by different studies to illustrate the correlation between lipid and incidence in multiple cancers. Although the conclusion remains controversial or sometimes contrary, which may be due to the multifactorial nature of the disease and the disparity of ethnic population, it is critical to elucidate the relationship between specific cholesterol components in certain population and the exact underlying mechanism of the lipid-associated signaling pathway in breast cancer. The implications of dysregulated lipoproteins as therapeutic targets or options for breast cancer provide novel strategies for us in combating with this malignant disease, which may be achieved by manipulating lipid levels with pharmacological compounds.
Introduction
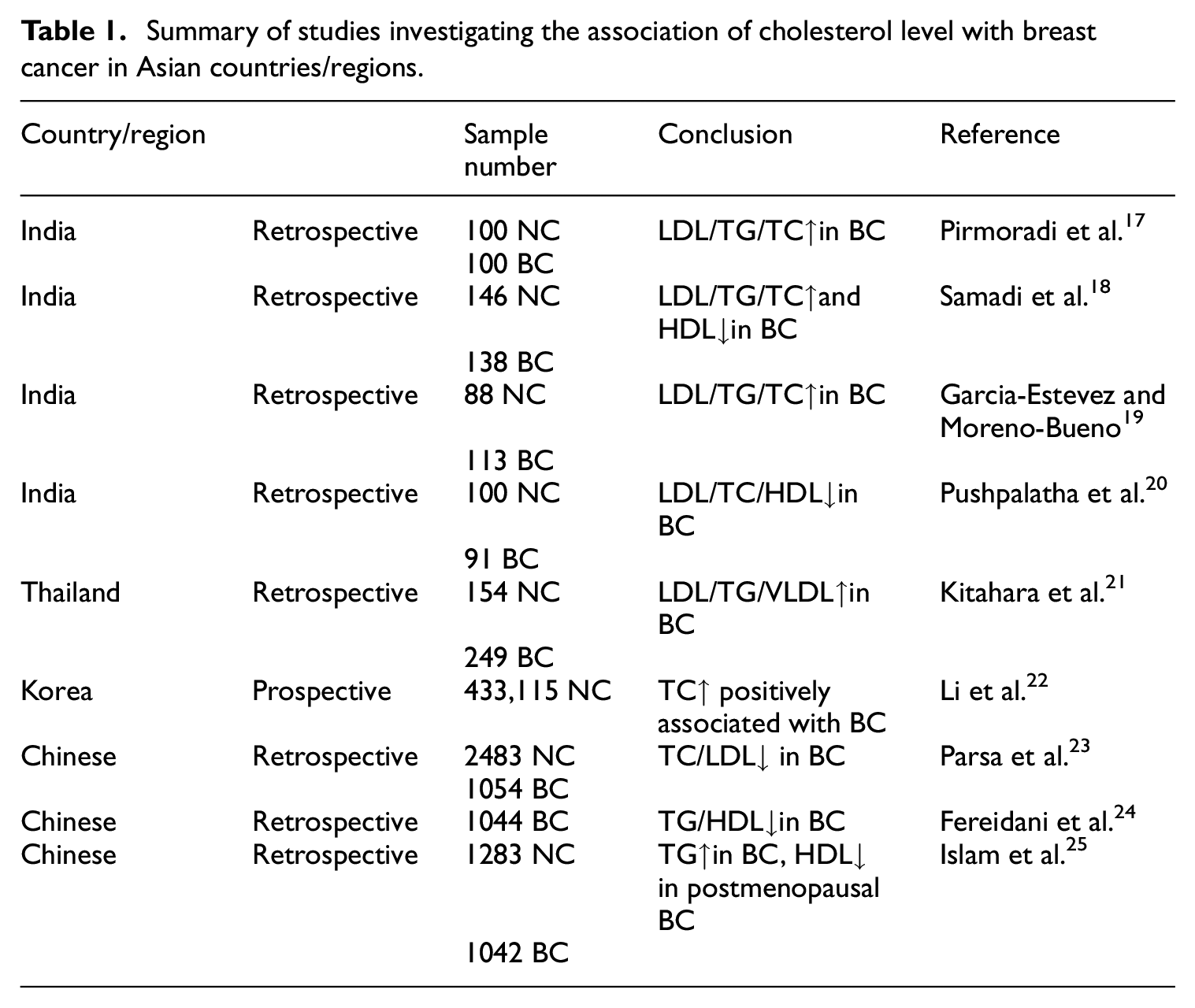
Breast cancer (BC) is the most common cancer in women and the second leading cause of cancer-related mortality worldwide. There were more than 2 million new diagnosed cases in 2018. 1 The etiology for breast cancer includes well-known risk factors such as genetic background, family history of breast cancer, personal history of breast cancer, exposure to estrogen, age. 2 Beside the above uncontrollable ones, risk factors including diet, weight, exercise which could be controlled by lifestyle modification have received increasing attention due to their roles in breast cancer development. 3 Cholesterol level, which is closely related to lifestyle changes, has been reported to be strongly associated with cardiovascular disease for long time. The lipoprotein profile includes total cholesterol (TC), triglycerides (TG), low-density lipoprotein (LDL), very low-density lipoproteins (VLDL), and high-density lipoprotein (HDL). Cholesterol levels, mostly focused on total form and LDL, are reported to be associated with cancer incidence in multiple cancer types such as prostate, 4 colorectal 5 and testicular cancer. 6 In breast cancer, controversial epidemiologic results have been reported in cholesterol level and breast cancer risk.7–10 Studies investigating the correlation between antihyperlipidemic agents such as statins and the risk of breast cancer onset are conflicting as well.11,12 Even for the dietary cholesterol intake, there is no consistent conclusion for its relationship with breast cancer risk.13–15 The great disparity of results in specific population indicated that biological differences may play a role in the involvement of cholesterol in breast cancer development. Since there is unclear link between cholesterol and breast cancer development, especially in Asian population, it is critical to further delineate by stratifying into total cholesterol, HDL, and LDL. 16 The studies investigating cholesterol and breast cancer risk in Asia were summarized in Table 1. Accumulating evidence supports a close association between dyslipidemia and breast cancer in Asian countries/regions. Most of the investigations suggested higher TC/TG/LDL and lower HDL levels in breast cancer patients than normal individuals. However, there is still great disparity of study results from different centers, which indicated that geographical distribution and ethnic factor may play vital role. Regarding this, two principal questions to be answered before fully elucidation of the relationship between breast cancer and specific lipid profile: (1) What’s the correlation between circulating lipid (e.g. LDL/HDL/VLDL) with breast cancer in specific population? (2) Whether breast cancer heterogeneity including different subtypes may explain the contradictory influence of lipid observed on breast cancer remains largely elusive.
Summary of studies investigating the association of cholesterol level with breast cancer in Asian countries/regions.
New contribution
Cholesterol has major public health importance as a significant etiology for coronary heart disease and ischemic stroke. Cholesterol is carried by lipoproteins such as VLDL, LDL, and HDL in circulation, which confer different functions in our body. LDL is well recognized as “bad” cholesterol for its contribution in forming atheromatous plaque, which is a significant risk factor for vascular morbidity and mortality. In contrast, HDL is well known as “good” cholesterol since the inverse correlation between reduced HDL levels and an increased risk of coronary disease and myocardial infarction.
In recent years, accumulating evidence has been revealed that cholesterol metabolism is involved in cancer development. For example, increased cholesterol levels are associated with a higher cancer incidence, and cholesterol-lowering drugs exhibit beneficial effects by reducing the risk and mortality rate in a number of caners such as breast, prostate, and colorectal cancer. In glioblastoma multiforme, regulating cholesterol metabolism via the mevalonate pathway may be a promise novel adjunctive clinical therapy. 17 However, the conclusions remain controversy among different study groups, which suggested that the effect of cholesterol in cancer development may be population specific. Most of the current studies are focusing on the relationship between LDL and cancer, especially the implication of LDL-lowering drugs in cancer treatment. Only limited literature reported on the linkage between HDL and breast cancers. Hence, we are still facing two major challenges before we take cholesterol manipulation into our consideration for breast cancer treatment strategy: (1) To illustrate the correlation between breast cancer and different cholesterol components such as VLDL, LDL, and HDL; (2) To investigate the potential clinical implications of lipid modifying agents especially HDL boosting medication in breast cancer.
In this review article, we have summarized the updated population-based epidemiological data and experimental evidence of different lipoproteins in Asian countries. Contradicting conclusions have been drawn by different research groups among Asian countries on the relationship of TC, TG, LDL, and breast cancer. HDL has been demonstrated a consistent inverse correlation with breast cancer. Only very limited study was reported on HDL as a therapeutic target or option for breast cancer especially in Asian, leaving large gap for clinician and scientists to fill in. Future studies may focus on the following aspects to investigate the potentials of HDL in treating breast cancer: (1) it may serve as desirable molecules for anticancer drugs delivery; (2) Reconstituted HDL nanoparticles may directly delivery cytotoxic anti-cancer agents into cytoplasm via HDL receptor; (3) The potential beneficial effect of HDL-raising drugs such as cholesteryl ester transfer protein inhibitor, fibrates, and niacin in treating breast cancer.
TC and breast cancer
TC is the overall amount of cholesterol in circulation including different components including TG, LDL, HDL, and VLDL. According to reported studies both in Asian and Western countries, the impact of TC as a risk factor for breast cancer is still conflicting. Biological signaling molecules may affect modulate cell growth, migration and invasion ability by interacting with cholesterol membrane in breast cancer cells. 18 The cholesterol-derived sex hormone such as estrogen play critical role in the development and pathogenesis of breast cancer. 18 Some groups revealed an inverse association between low serum cholesterol and cancer while no significant correlation found in other groups.19–23 Other studies suggested that diet pattern contain high cholesterol and refined grain associated with a lower risk of breast cancer. 24 A meta-analysis of 13 studies investigating the associations between breast cancer risk and TC revealed the hazard ratio (HR) was 0.97 (95% CI 0.94, 1.00; dose-response per 1 mmol/l increment). 9 By contrast, a study including large cohort of over 664,000 patients demonstrated that women above 40 with high cholesterol levels were 45% less likely to develop breast cancer than those without high cholesterol. What’s more, the risk of death was 40% lower in breast cancer patients with high cholesterol. 19 This controversy prompted some authors to look into the use of statins to lower cholesterol. However, no conclusive remark was made in this topic neither.11,12,14,15,25 The intrinsic correlation between TC and breast cancer might be masked by the contribution of different components, which makes it necessary to analyze each component individually.
TG and breast cancer
TG consists of three molecules of fatty acid and one molecule of alcohol glycerol, serving as the backbone of many types of lipids. High level of TG has long been considered as risk factor for atherosclerosis since a wide range of TG-containing lipoproteins transport cholesterol in circulation. 26 Data from most studies indicated positive association between TG level and breast cancer as listed in Table 1. A study recruiting 464 triple negative breast cancer (TNBC) patients found that patients in the highest tertile of TG (≥1.23 mmol/l) had three times higher overall mortality compared to TNBC patients in the lowest tertile (≤0.82 mmol/l) (HR 2.99, 95% CI 1.17–7.63), and the 5-year overall survival was 19% lower in the highest versus lowest tertile of TG (65% vs 84%). 27 Similarly, in general breast cancer patients with high levels of TG have been reported to show a poor prognosis.7,28–30 Apart from the positive association of TG and breast cancer risk, TG is also considered as a prognostic factor for recurrence. 31 Some experiments have been carried out to investigate the underlying mechanism of TG in breast cancer occurrence and development. The proto-oncogene Src, well-known pro-mitogenic signaling cascades to cause tumors, plays a critical role in TG synthesis, which endows cells with advantages in proliferation and metastasis in breast cancer. 32 However contradictory results were reported in other studies. A meta-analysis of prospective cohort studies involving 1,189,635 participants and 23,369 breast cancer cases suggested that serum levels of TG may be inversely associated with breast cancer risk. 33 Being the most common lipid found in the body, although the potential underlying mechanism of TG in breast cancer remains to be clarified, TG may function as an oncogenic player by providing energy to cancer cells or regulating cholesterol such as LDL and HDL by means of lipoproteins.
LDL and breast cancer
LDL helps to transport cholesterol which is essential for membrane and synthesis of the steroid hormones to maintain normal function of the cells. 34 Being referred as the “bad cholesterol,” LDL is well recognized as a major risk factor for atherosclerosis, predisposing to major cardiovascular events such as myocardial infarction and stroke. 35 LDL receptor was demonstrated significantly upregulated in breast cancer cells to increase LDL uptake as to meet the demand of rapid proliferating cancer cells. 36 There was in vitro evidence showed that LDL promoted cell proliferation and migration ability in ER-positive cells 37 but not in ER-negative cells, 38 suggesting that the role of LDL in breast cancer may be subtype-dependent. In breast cancer cells treated with LDL, oncogenic pathway genes such as pJNK, pAKT, and pERK were upregulated while cell-cell junction-related genes Claudin7 and Ocludin downregulated, resulted in enhanced cell migration and decreased adhesion.39–43 In fact, one prospective study demonstrated that high plasma LDL levels were associated with HER2-positive breast cells. 44 Besides in vitro evidence, in animal models of hyperlipidemia, elevated LDL receptor expression was reported to accelerate cholesterol-mediated breast cancer growth, which could be reversed by LDL receptor silencing. This finding highlights the potential importance of LDL in cancer development. 45 In human breast cancer, LDL receptor was found to be upregulated in HER2 positive and TNBC, both of which were more cholesteryl ester-rich and more progressive with higher Ki-67 expression and tumor necrosis compared with luminal subtype tumors. Therefore, increased LDL internalization due to LDL receptor upregulation led to cholesteryl ester accumulation in vessel endothelial cells, which was believed to be associated with more malignant breast cancer phenotype. 46 It has become abundantly clear that oxidized LDL which could be absorbed by endothelial cell led to promote the expression of pro-inflammatory genes and recruitment of monocyte into vessel wall, resulting in endothelial dysfunction, and injury.47–49 During breast cancer carcinogenesis, lipid peroxidation is considered as one of the main reasons causing DNA structural alterations.50,51 There was a study illustrated that oxidized LDL promoted breast cells viability via PI3K/AKT oncogenic signaling pathways in microRNA-mediated manner. 52 Oxidized LDL lecithin-like receptor 1 (OLR1) is the main receptor for facilitating the oxidized LDL into breast cancer cells, which also positively correlates to tumor stage and grade. 53 OLR1 is demonstrated to play oncogenic role by upregulating NF-κB and inhibiting apoptosis 54 as well as promoting migration. 55
VLDL and breast cancer
VLDL particles are produced by the parenchymal cells of the liver and are TG rich. Its function is to carry TG to muscle and adipose tissue for hydrolyzation to provide fatty acids that can be oxidized to produce ATP. Ninety percent of the serum TGs in the fasting state were carried by VLDL. 56 They can be re-esterified to glycerol and stored as fat when there is no need for energy production, which is main contributor for obesity. 57 Obesity is one of the most important risk factors for breast cancer which correlated with poor survival rate.58,59 Epidemiological studies in Asian countries have shown a strong relationship between breast cancer and VLDL.60–62 Experimental studies demonstrated that VLDL increased breast cancer cell migration and invasion ability by upregulating the mesenchymal markers expression and promoted angiogenic activity through enhanced secretion of angiogenic factors. 37 What’s more, VLDL was reported to play oncogenic role in drug-resistant HER2-positive breast cancer cells. 63
HDL and breast cancer
HDL contains a wide spectrum of lipoprotein particles with density ranges from 1 to 1.2 g/ml. The major HDL apolipoproteins are ApoA-I and II, both of which are required for normal HDL biosynthesis. Being the most abundant apolipoprotein in plasma, ApoA-I consist approximately 70% of HDL particles. ApoA-II is synthesized only in liver, constitutes approximately 20% of HDL protein. 64 It is widely accepted that HDL as “good cholesterol” since multiple epidemiological studies clearly demonstrated that HDL levels are inversely associated with the risk of cardiovascular disease and its thrombotic complications.65–67 HDL plays a major role in reverse cholesterol transport, removing excess cholesterol from circulation and deliver to liver for metabolic disposal. 68 Besides cholesterol clearance, HDL enhances its protective effect against cardiovascular disease by other biological properties such as antithrombotic, cytoprotective, anti-inflammatory, vasodilatory and antioxidative functions.69–72 Cancers including breast cancer show specific alterations in different aspects of metabolism such as lipid metabolism, which lead to dysfunction in structural cell membrane synthesis, lipids energy homeostasis, lipid-related signaling activating inflammation-related pathways. With all the changes mentioned above and considering the multiple functions of HDL, more and more attention is being drawn to the relationship between HDL and cellular processes, including cell growth, proliferation, differentiation, and motility. 73 Concerning HDL and breast cancer, discordant results were found in different countries or regions. Most of the studies conducted so far have identified inverse correlation between cancer and HDL, however, some meta-analyses found only a modest, null or even positive correlation between cancer and HDL levels. The reason for this may be due to confounding factors such as obesity, insulin resistance, smoking habit which may reduce HDL levels and prone to cancer development. 74 A meta-analysis of six prospective studies investigating the associations between HDL levels and the risk of breast cancer found that HR was 0.86 (95% CI 0.69, 1.09; dose-response per 1 mmol/l increment). 9 One prospective study in France found an inverse association between HDL and breast cancer risk. 75 In contrast, a Mendelian randomization study showed that raised HDL increased the risk of estrogen receptor (ER)-positive breast cancer patients from European ancestry. 76 Meanwhile other studies failed to find any association between HDL and breast cancer risk or survival.77–79 However, most of the studies demonstrated decreased HDL levels in Asian breast cancer patients (Table 1). Despite the discrepancies in these studies, it is still proposed that HDL functionality might have a bearing on the breast cancer. It is critical to keep in mind that clinical or methodological factors such as study design, geographic variation, follow up length, sample size play unneglectable roles in the result interpretation. For this reason, it may be important to determine the potential underlying mechanisms for the association between HDL and breast cancers by basic scientific research. 80 Interestingly, HDL and its modified forms were confirmed to be oncogenic in most breast cancer experimental studies according to reported literature. 81 HDL was reported to stimulate proliferation of breast cancer cell lines in dose-dependent manner.82,83 The most abundant HDL apolipoprotein ApoA-I was found to be inversely associated with breast cancer risk.62,75,84 Overexpression of ApoA-I in inherited breast cancer mice model showed reduced the levels of oxidized LDL and increased 27-hydroxycholesterol, which could promote tumor growth. 85 The HDL receptor scavenger receptor class B type I (SR-B1), which mediates cholesterol uptake, was reported to be abundantly expressed in human breast cancer tissue compared with adjacent normal tissue.86,87 SR-B1 contributes to the tumor development and malignant processes via AKT and ERK1/2 signaling pathways in breast cancer. 88 ATP-binding cassette transporter A1 (ABCA1) and ATP-binding cassette transporter G1 (ABCG1) that recruits ApoA-I as receptor and mediates cholesterol to HDL, respectively, were identified to play a pivotal role in regulating cholesterol within the cells, which is essential to cell function and survival.89–91 Although HDL has been identified to be correlated with breast cancer development, very limited study was reported on its implication as a therapeutic target or option for breast cancer especially in Asian, leaving large gap for clinician and scientists to fill in. Having considered the biological and functional properties of HDL, future studies are needed to investigate the potentials of HDL in treating breast cancer in following aspects: (1) HDL may serve as desirable molecules for anticancer drugs delivery due to its affinity and ability to accumulate within cancer cells;92,93 (2) Reconstituted HDL nanoparticles (rHDL NP)-based formulations to directly delivery cytotoxic anti-cancer agents into cytoplasm via facilitation of HDL receptor SR-B1, may overcome the drug resistance which caused by the pumping units located in the membranes of malignant cells94–96; (3) The inverse correlation between HDL levels and breast cancer indicated the therapeutic potential of HDL-raising drugs such as cholesteryl ester transfer protein inhibitor (e.g. anacetrapib, evacetrapib), fibrates and niacin. 97 The summarized lipoprotein-associated signaling pathways in breast cancers were listed as Figure 1.

The lipoprotein-associated signaling pathways in breast cancers.
Conclusions and future challenges
The deregulation of cholesterol homeostasis in breast cancer merits a review of its own. In this article, we summarized population-based epidemiological data and experimental evidence of different lipid components especially in Asian countries. Although conflicting or sometimes contradictory results have been rendered from different institutes, which may be possibly owing to multifactorial nature of the disease, it would be quite challenging to establish a causal relationship between cholesterol and breast cancer in specific Asian population. Large scale retrospective or prospective analysis and mechanistic studies both in vivo and in vitro are needed for fully elucidation of cholesterol’s role in breast cancer development. The lipid manipulation such as HDL-raising agents may provide us novel strategy toward this malignant disease, which still warrant further investigations on basic research and preclinical trials.
Limitations of the review
In this review, we summarized the relationship between TG, TC, LDL, VLDL, HDL, and the occurrence and development in breast cancer, aiming to provide a comprehensive picture in this field. However, inconsistent conclusions were drawn in different studies among various populations or countries. In future study, larger cohort of patients with specific subgrouping such as ethnic group will be more informative for a conclusive relationship between lipid profile and breast cancer. This will help to provide insight into the development of novel strategy for breast cancer prevention and treatment.
Footnotes
Authors’ contributions
Yanghui Wei and Jiawei Chen performed literature research and drafted the manuscript. Yao Huang, Weiqin Yang and Juan Chen reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical approval was not sought for the present study because this was a review article and did not involve any patients.
Informed consent
Informed consent was not sought for the present study because this was a review article and did not involve any subjects.