
Abstract
Information on the stage of liver cirrhosis is essential for prognostication and decisions on surgical planning for hepatocellular carcinoma (HCC) patients. But a non-invasive liver cirrhosis staging model is still lacking. The aim of our study was to develop a non-invasive model based on routine clinical parameters to evaluate the severity of cirrhosis in hepatitis B related HCC patients. A total of 226 HCC patients with chronic hepatitis B virus (HBV) infection who had liver resection were analyzed in this retrospective study. We found that platelets, prothrombin activity, maximum oblique diameter of right hepatic lobe and spleen length were the independent predictors of liver cirrhosis in HCC patients. By cumulating the weight of risk scores of independent variables, we constructed the PPMS (PLT/PTA/maximum oblique diameter of right hepatic lob/spleen length) index. The areas under the receiver operating characteristic curves (AUROC) of PPMS index were 0.820, 0.667, and 0.650 in predicting ≥cirrhosis 1 (C1), ≥cirrhosis 2 (C2), and ≥cirrhosis 3 (C3), respectively. The optimal cut-off value of the PPMS index for predicting ≥C1, ≥C2, and ≥C3 was 4.392, 4.471, and 4.784, respectively. And the corresponding sensitivity was 63.1%, 63.2%, and 64.7%, the corresponding specificity was 89.4%, 64.3%, and 62.5%, respectively. Our study constructed a non-invasive liver cirrhosis index (PPMS) could distinguish patients from different stages of liver cirrhosis, which might add more preoperative information for HCC patients.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancers worldwide and the second leading cause of cancer-related deaths. 1 The major cause of HCC as well as cirrhosis in Asia is chronic hepatitis B (CHB), a disease caused by hepatitis B virus (HBV). 2 On the other hand, HCC usually occurs on a background of cirrhosis, up to 88% in Yang’s studies. 3 To date, surgical resection remains the best and most prevalent treatment for HCC patients. Knowledge of the stage of liver cirrhosis is essential for prognostication and decisions on surgical planning. HCC patients with no or mild cirrhosis at presentation appear to have better liver reserve function and recover well from surgical trauma. Otherwise, HCC patients with significant cirrhosis are more likely to suffer liver failure after partial liver resection caused by an insufficient quantity and function of the liver remnant. The severity of liver cirrhosis in HCC patients is closely related to preoperative hepatic reserve function as well as postoperative regeneration of remnant liver volume. 4 Thus, staging liver cirrhosis would be helpful to predict disease prognosis and make better determination in avoiding severe complications for HCC patients who are going to have liver resection.
Liver biopsy is recognized as the gold standard for assessing histological stages of liver fibrosis and cirrhosis. However, liver biopsy is an invasive and costly procedure, which hinders its widespread utilization in routine practice. 5 Thus, many fibrosis staging models based on routine laboratory tests, such as aspartate transaminase (AST) to platelet (PLT) ratio index (APRI), gamma-glutamyltranspeptidase to platelet ratio (GPR), and the fibrosis-4 score (FIB-4), have been recommended as a non-invasive tool to detect liver fibrosis and cirrhosis when liver biopsy is not unavailable.6–8 But these non-invasive fibrosis staging models mostly focus on liver fibrosis staging, rather than liver cirrhosis staging. Thus, it is urgent to develop a novel non-invasive liver cirrhosis staging model, especially for those who are going to have liver resection because of HCC.
The aim of the present study was to develop a non-invasive model based on routine clinical parameters to evaluate the severity of cirrhosis in HCC patients with chronic HBV infection.
Patients and methods
Patients and routine clinical data
This is a retrospective study including 306 suspicious HCC patients with chronic HBV infection who had liver resection in the Third Affiliated Hospital of Sun Yat-Sen University (n = 213) and Jiangmen Central Hospital (n = 93) between January 2013 and December 2016. Patients were excluded from this study for the following reasons: pathological diagnosis confirmed not HCC, history of hepatectomy or splenectomy, insufficient pathalogical description about liver fibrosis or cirrhosis, insufficient laboratory parameters or ultrasound imaging indexes. Eventually, a total of 226 patients were included in this study (Figure 1).

Flow diagram describing the selection of the study population.
The study was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-Sen University (Guangzhou, China) and the Jiangmen Central Hospital (Jiangmen, China). Written informed consent was obtained from all participants. This study was conducted in accordance with the World Medical Association Declaration of Helsinki.
Routine clinical data collections
Patient demographic and laboratory parameters were collected at the time before liver resection. Abdominal ultrasound was used to estimate liver and spleen voleme. Maximum oblique diameter of right hepatic lobe, superoinferior diameter of left hepatic lobe, anteroposterior diameter of left hepatic lobe, diameter of main portal vein, spleen length (the maximum spleen bipolar diameter), inner diameter of splenic portal vein and thickness of spleen were recorded.
Liver histological score and definitions
Liver samples from surgical resection were formalin-fixed and paraffin-embedded for histological analysis. Specimens sections with at least six portal areas were stained with hematoxylin and eosin (HE), Masson’s trichrome and reticular fiber staining. Histological diagnoses were interpreted by two pathologists independently, who were blinded to the clinical information. When there was a disagreement between the two pathologists, the final grade of liver cirrhosis was determined after discussion. Liver fibrosis stages was assessed using the Laennec fibrosis scoring system: F0, no fibrosis; F1, portal fibrosis without septa; F2, portal fibrosis with rare septa; F3, numerous septa without cirrhosis; F4A, mild cirrhosis; F4B, moderate cirrhosis; and F4C, severe cirrhosis. The Laennec scoring system is a subclassification of METAVIR score, which subdivides the highest fibrosis stage 4 into 4A, 4B, and 4C. It tightly correlates with the clinical stages of liver cirrhosis, severity of portal hypertension, and Child-Pugh and MELD scores, also adds useful diagnostic and prognostic information that aids in the optimum management of patients with cirrhosis.9,10 In the present study, we defined F0–F3 as cirrhosis 0 (C0), F4A as cirrhosis 1(C1), F4B as cirrhosis 2 (C2), and F4C as cirrhosis 3 (C3).
Statistical analysis
Data analyzes were performed using SPSS version 22.0 software (SPSS Inc., Chicago, IL, USA) and GraphPad Prism 5.0 (GraphPad Software, San Diego, CA, USA). Continuous variables were expressed as mean ± standard deviation (SD) and compared using one-way ANOVA test. Categorical variables were reported as number (percentage). For the formulation of predictive models, univariate analysis was performed on variables between patients with and without cirrhosis. Significant variables from the univariate analysis were then subjected to multivariate analysis by forward logistic regression to identify independent factors associated with cirrhosis. Formulas with risk scores that could best predict liver cirrhosis were constructed by entering different sets of independent variables into the regression model. Correlations between liver cirrhosis model scores and Laennec scoring system were evaluated by the Spearman’s rank correlation coefficient. The area under the receiver operating characteristic curve (AUROC) was used to evaluate the diagnostic accuracy of established model in predicting cirrhosis stage. Optimal cut-off predicting liver cirrhosis stage ≥C1, ≥C2, and ≥C3 was determined according to the maximization of Younden index by receiver operating characteristic (ROC) curve analysis. All statistical analyzes were two-tailed and a p value of <0.05 was considered to be statistically significant.
Results
Clinical characteristics of the population
A total of 306 suspicious HCC patients who had liver resection were enrolled in this study. Eighty patients were excluded as the following reasons: (1) pathological diagnosis confirmed not HCC (n = 14); (2) history of hepatectomy (n = 4) or splenectomy (n = 7); (3) insufficient pathalogical description about liver fibrosis or cirrhosis (n = 29); (4) insufficient laboratory parameters or ultrasound imaging indexes (n = 26). Eventually, 226 patients were included in this study (Figure 1). The distribution of liver cirrhosis stages in the population was as follows: C0, 47 (20.8%) patients; C1, 65 (28.8%) patients; C2, 80 (35.4%) patients; and C3, 34 (15.0%) patients. A detailed demographic and laboratory, ultrasound imaging parameters of the patients were shown in Table 1.
Clinical characteristics of the study population.
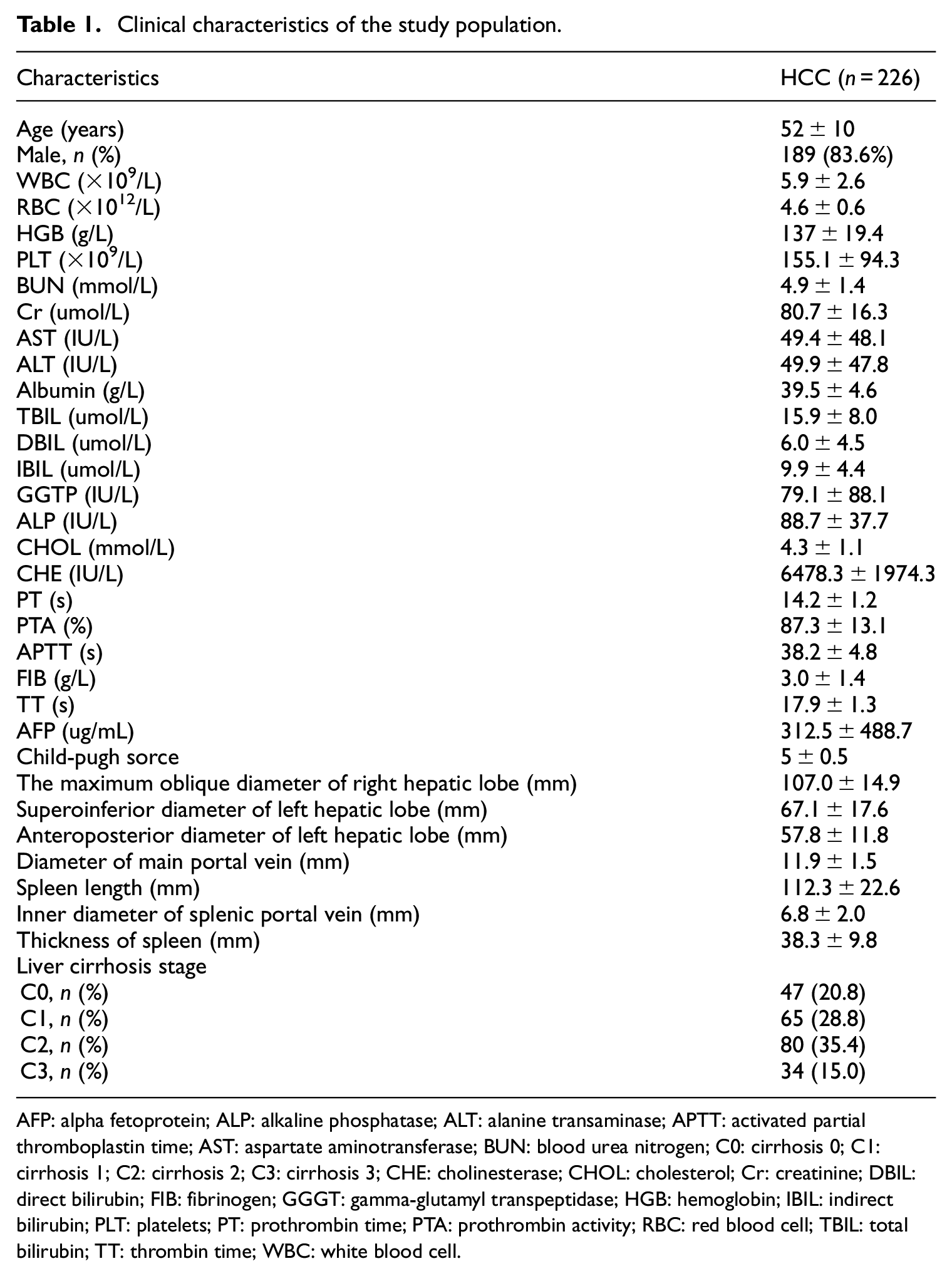
AFP: alpha fetoprotein; ALP: alkaline phosphatase; ALT: alanine transaminase; APTT: activated partial thromboplastin time; AST: aspartate aminotransferase; BUN: blood urea nitrogen; C0: cirrhosis 0; C1: cirrhosis 1; C2: cirrhosis 2; C3: cirrhosis 3; CHE: cholinesterase; CHOL: cholesterol; Cr: creatinine; DBIL: direct bilirubin; FIB: fibrinogen; GGGT: gamma-glutamyl transpeptidase; HGB: hemoglobin; IBIL: indirect bilirubin; PLT: platelets; PT: prothrombin time; PTA: prothrombin activity; RBC: red blood cell; TBIL: total bilirubin; TT: thrombin time; WBC: white blood cell.
Variables associated with liver cirrhosis and construction of a novel index for predicting liver cirrhosis
Variables associated with liver cirrhosis in the population were shown in Table 2. Univariate analysis identified that white blood cell (WBC), red blood cell (RBC), hemoglobin (HGB), platelets (PLT), albumin, total bilirubin (TBIL), direct bilirubin (DBIL), cholesterol (CHOL), cholinesterase (CHE), prothrombin time (PT), prothrombin activity (PTA), maximum oblique diameter of right hepatic lob, diameter of main portal vein, spleen length, inner diameter of splenic portal vein and thickness of spleen were significantly related to liver cirrhosis in HCC patients. In the subsequent multivariable analysis, we found that PLT (OR = 0.996, p = 0.041), PTA (OR = 0.963, p = 0.036), maximum oblique diameter of right hepatic lob (OR = 0.966, p = 0.017) were negatively correlated with liver cirrhosis, while spleen length (OR = 1.053, p = 0.001) was positively correlated with liver cirrhosis. Regression formula for prediction of liver cirrhosis was constructed by cumulating the weight of risk scores of independent variables. We named it PPMS (PLT/PTA/maximum oblique diameter of right hepatic lob/spleen length) index:

Univariate and multivariate analyzes of the variables associated with liver cirrhosis in the study.
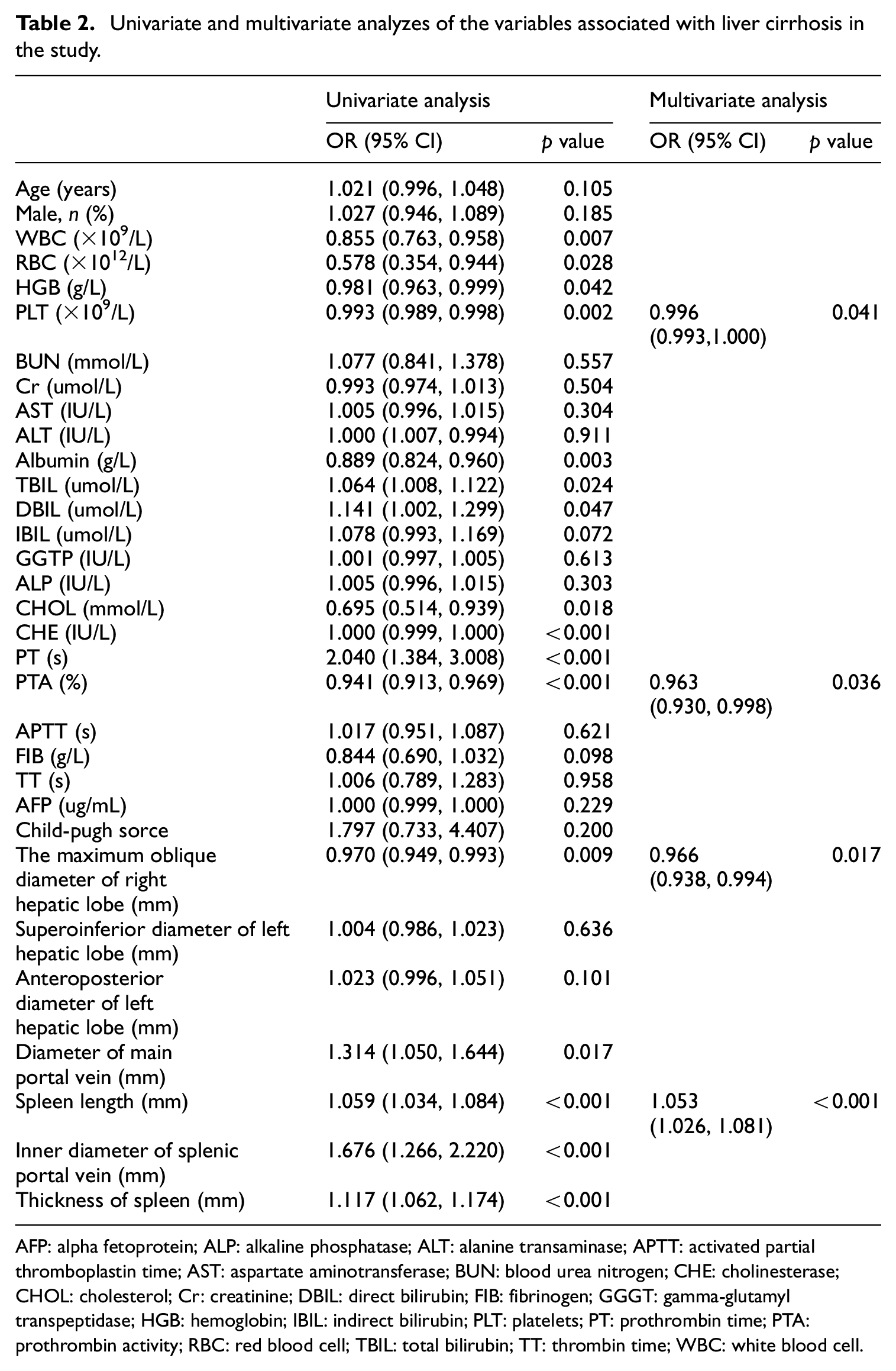
AFP: alpha fetoprotein; ALP: alkaline phosphatase; ALT: alanine transaminase; APTT: activated partial thromboplastin time; AST: aspartate aminotransferase; BUN: blood urea nitrogen; CHE: cholinesterase; CHOL: cholesterol; Cr: creatinine; DBIL: direct bilirubin; FIB: fibrinogen; GGGT: gamma-glutamyl transpeptidase; HGB: hemoglobin; IBIL: indirect bilirubin; PLT: platelets; PT: prothrombin time; PTA: prothrombin activity; RBC: red blood cell; TBIL: total bilirubin; TT: thrombin time; WBC: white blood cell.
In the formula, 6.525 represented the constant, 0.004, 0.037, 0.035, and 0.051 represented the partial regression coefficient B of PLT, PTA, maximum oblique diameter of right hepatic lobe and spleen length, respectively. By entering different sets of independent variables into the formula, the PPMS index can be scored.
Relationship between the Laennec scoring system and the PPMS index
The PPMS index score showed an increasing trend with liver cirrhosis stage, and the mean score in C0, C1, C2, and C3 stage was 3.233 ± 0.178, 4.823 ± 0.183, 5.080 ± 0.195, 5.305 ± 0.286, respectively (p < 0.001, Figure 2(a)). Correlation between histological sub-classification of cirrhosis and PPMS index score was evaluated by the Spearman’s rank correlation coefficient analysis. PPMS index score significantly correlated with the Laennec scoring system, which increased parallel to the rise of histological grade of cirrhosis (r = 0.388, p < 0.001, Figure 2(b)).
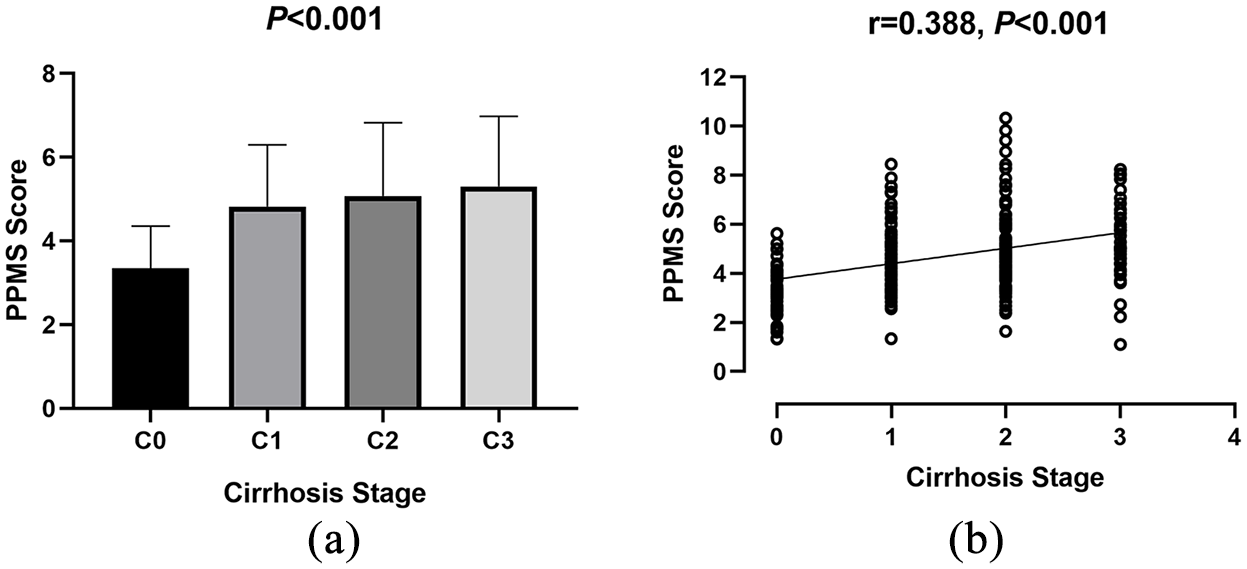
Relationship between the Laennec scoring system and the PPMS index: (a) mean ± SD score of PPMS index in C0, C1, C2, and C3 stage and (b) PPMS index score increased parallel to the rise of histological grade of cirrhosis.
Diagnostic performances of PPMS index for liver cirrhosis
ROC curves of the PPMS index for predicting liver cirrhosis stages according to the Laennec scoring system were plotted in Figure 3. AUROC of the PPMS index in predicting ≥C1, ≥C2, and ≥C3 were 0.820 (95% CI, 0.759–0.881), 0.667 (95% CI, 0.597–0.737), 0.650 (95% CI, 0.553–0.748), respectively (Table 3). According to the maximization of Younden index from the ROC curve analysis, the optimal cut-off value of the PPMS index for predicting ≥C1, ≥C2, and ≥C3 was 4.392, 4.471, and 4.784, respectively. And the corresponding sensitivity was 63.1%, 63.2%, and 64.7%, the corresponding specificity was 89.4%, 64.3%, and 62.5%, respectively.

Receiver operating characteristic (ROC) curves of the PPMS index in diagnosing: (a) ≥C1, (b) ≥C2, and (c) ≥C3.
Diagnostic accuracy of PPMS index for the prediction of liver cirrhosis in the HCC patients.

Discussion
HCC usually occurs on a background of liver cirrhosis, and chronic HBV infection accounts for the most common etiology.1,3 The various cirrhosis stages may have distinct responses to hepatectomy, meaning that a better cirrhosis stage understanding may contribute to better management of these patients and reduce unpredictable surgical related mortality. In this setting, the non-invasive diagnosis of liver fibrosis is a rapidly growing field of research; blood fibrosis tests, liver elastometry, and radiologic techniques are improving in diagnostic accuracy. 11 However, most non-invasive approaches aim in assessment of fibrosis and diagnosis of cirrhosis, but not in classification of cirrhosis according to its severity. In this study, we intended to develop a novel non-invasive model for accurately staging liver cirrhosis based on routine clinical parameters in HCC patients with chronic HBV infection, especially for those who are going to have liver resection.
We found that PLT, PTA, maximum oblique diameter of right hepatic lob and spleen length were the independent predictors of liver cirrhosis in HCC patients. In clinic practice, these four parameters are easily obtainable during the serum examination and routine ultrasonography. Given that, by combining these independent predictors, we constructed the PPMS index with AUROC of 0.820, 0.667, and 0.650 in predicting ≥C1, ≥C2, and ≥C3, respectively. For C1, a PPMS threshold of 4.392 was 63.1% sensitive and 89.4% specific. For C2, a PPMS threshold of 4.471 was 63.2% sensitive and 64.3% specific. For C3, a PPMS threshold of 4.784 was 64.7% sensitive and 62.5% specific.
These four parameters had been widely used in predicting liver fibrosis and cirrhosis. First, an increased sequestration and destruction of PLT is common in the enlarging spleen with increasing fibrosis and worsening portal hypertension. 12 Decreased production of thrombopoietin by hepatocytes with the progression of liver fibrosis also reduces PLT production.6,13 As thus, PLT count has been used in many non-invasive fibrosis staging models, such as APRI, GPR.13,14 Second, the liver performs an important role in biosynthesis, including blood clotting factor: prothrombin. In practice, prolonged prothrombin time is used to calculate the Child-Pugh score, probably due to reduced synthesis and activity of prothrombin in chronic dysfunctional liver.15,16 In accordance with our findings, Jérôme Boursier and his colleagues also found that PTA was an independent factor and developed a stepwise algorithm for easily detection of advanced liver fibrosis in all chronic liver disease patients. 17 Third, during the process of cirrhosis, liver parenchymal volume decreases gradually as the atrophy of left medial segment and right hepatic lobe. Accessing the liver parenchymal volume could be helpful in evaluating the reserved liver function.18–20 In this study, we found that the maximum oblique diameter of right hepatic lob was negatively correlated with liver cirrhosis stages in HCC patients. Also, splenomegaly is a frequent finding of chronic liver cirrhosis as a consequence of portal hypertension. Taken together, combing these cirrhosis relevant variations could be a potential indicator for diagnosing liver fibrosis and cirrhosis.20,21
In the present study, we classified liver cirrhosis into four grades according to the Laennec fibrosis scoring system: C0 equal to F0–F3, C1 equal to F4A, C2 equal to F4B, and C3 equal to F4C. The Laennec histological sub-classification of cirrhosis correlates well with clinical severity of cirrhosis, and can provide useful prognostic information.9,10 However, the Laennec fibrosis score is estimated through an invasive liver biopsied tissue or postoperative liver specimen, which might prevent its wide utilization in preoperative liver cirrhosis evaluation. Here, we built up a novel non-invasive model for staging liver cirrhosis by using four easy obtained clinical parameters, which significantly correlated with the Laennec scoring system.
We acknowledge that there are limitations to our study. First, our study was a retrospective study with relatively small cohort size. Second, intercenter variations in the laboratory testing could not be avoided among centers, as well as inter- and intra-observer variations in ultrasound imaging and liver histological scores. Third, there was no validation study and longitudinal follow-up data to assess the significance of this new model for the diagnostic and prognostic information in HCC patients with chronic HBV infection, which remains to be investigated in our future studies. Fourth, low diagnostic performance in our study should be further validated. Fifth, no comparisons were available with other non-invasive methods, such as FIB-4, APRI, fibroscan, or ARFI, because of different points of focus.
Conclusions
Based on four routine clinical parameters, we constructed a non-invasive liver cirrhosis index for those who are going to have liver resection because of hepatitis B related HCC. The PPMS index could distinguish patients from different stages of liver cirrhosis and might contribute to better managements and reduced unpredictable surgical related mortality of HCC patients. But further investigation is warranted to validate the diagnostic and prognostic performance of the PPMS index.
Footnotes
Acknowledgements
We deeply thank the physicians who performed the hepatectomy surgeries.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and informed consent
The study was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-Sen University (Guangzhou, China) and the Jiangmen Central Hospital (Jiangmen, China). Written informed consent was obtained from all participants. This study was conducted in accordance with the World Medical Association Declaration of Helsinki.