
Abstract
As the coronavirus disease 2019 (COVID-19) spreads globally, hospital departments will need take steps to manage their treatment procedures and wards. The preparations of high-risk departments (infection, respiratory, emergency, and intensive care unit) were relatively well within this pandemic, while low-risk departments may be unprepared. The spine surgery department in The First Affiliated Hospital of Anhui Medical University in Hefei, China, was used as an example in this study. The spine surgery department took measures to manage the patients, medical staff and wards to avoid the cross-infection within hospital. During the outbreak, no patients or healthcare workers were infected, and no treatment was delayed due to these measures. The prevention and control measures effectively reduced the risk of nosocomial transmission between health workers and patients while providing optimum care. It was a feasible management approach that was applicable to most low-risk and even high-risk departments.
Strengths and limitations of this study
Comprehensively valuable strategies were provided to prevent the transmission of COVID-19 in spine surgery department, as well as other low-risk departments.
All these measures have been applied and no patients or health workers have been infected.
Our measures are limited to low-risk departments and more studies are required to verified their feasibility.
Introduction
On April 2, 2020, the number of people diagnosed with the coronavirus disease 2019 (COVID-19) worldwide crossed 1 million and healthcare systems around the world were scrambling to meet the demands. 1 A previous study reported that of the 44,672 cases, a total of 1716 were healthcare workers (3.8%), of which 14.8% were classified as severe or critical cases and five died. 2 Therefore, the exposure and possible infection of healthcare workers posed a massive challenge to the delivery of medical services in hospital. 3 Compared with high-risk departments, the management strategy of low-risk departments were relatively weak. Possible reasons include: (1) Input of asymptomatic COVID-19 infection. (2) General susceptibility of patients on the ward. (3) Relative scarcity of medical resources. (4) The infection control measures were relatively weak. (5) Mostly open management. Although general outpatient clinics no longer received patients, emergency patients in low-risk departments often had severe symptoms and underlying diseases that require immediate treatment, while their COVID-19 infection status were unknown. Therefore, low-risk departments need to pay more attention to the outbreaks and formulate prevention and control measures.
Measures
This study take the spine surgery department in The First Affiliated Hospital of Anhui Medical University in Hefei, China as an example. The spine surgery department took drastic measures: established the emergency group (Figure 1(a)), modified treatment procedures (Figure 1(b)), took knowledge training about COVID-19, and standardized management of wards.
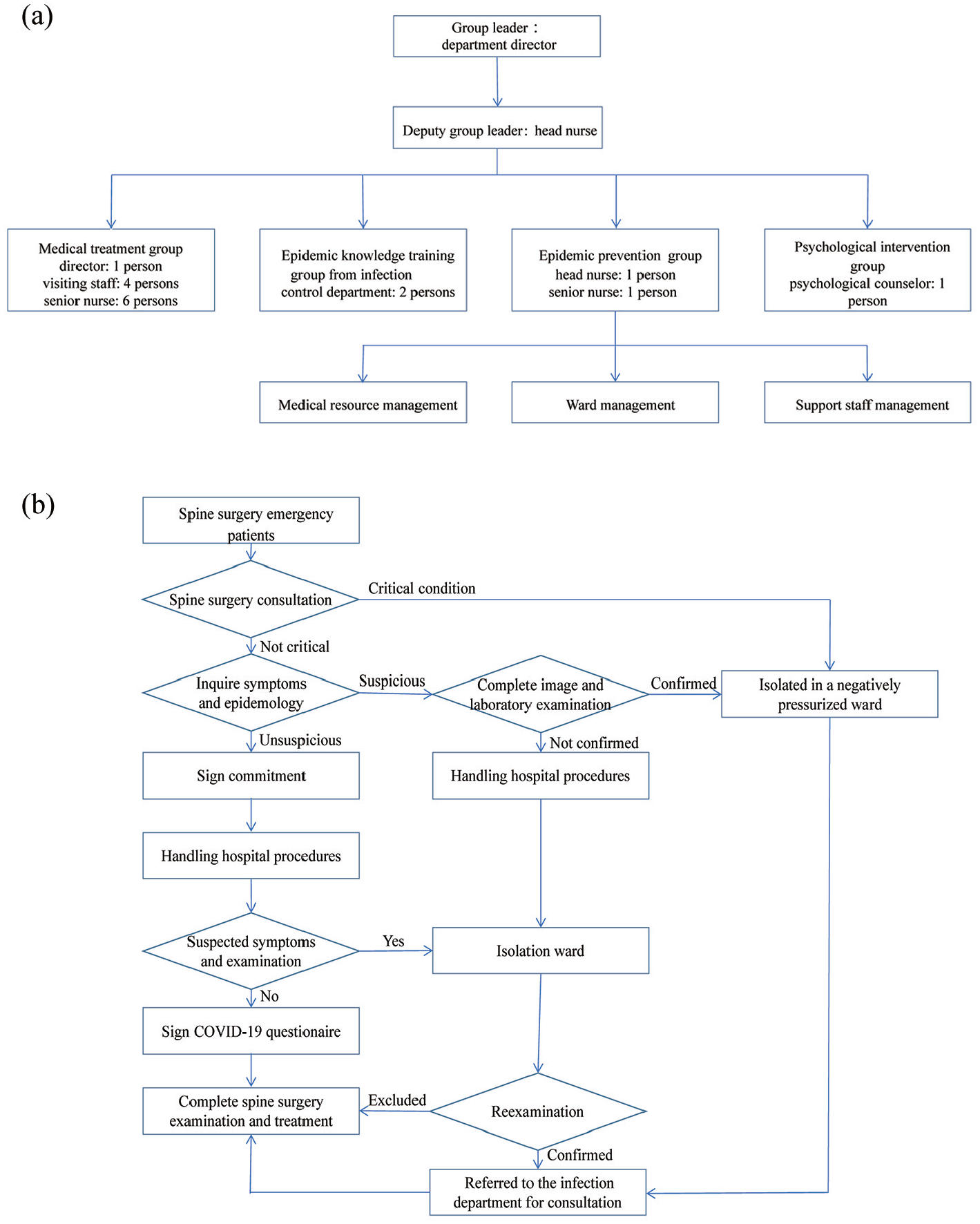
The composition of emergency group and treatment procedures in spine surgery department: (a) The emergency group was arranged based on its function and their job was the same as the group name. As the group leader, the department director was responsible for the arrangement of the work of each member. And the head nurse was responsible for the specific implementation of work as a deputy group leader. (b) Part of the procedures were based on the patients’ COVID-19 infection status and vital signs.
The emergency group was organized according to its functions. The treatment procedures were as follows: monitoring the patients’ vital signs while assessing the COVID-19 infection risks, including: symptoms (cough, fever), epidemiology history (traveled or resided in Hubei province or other communities with cases within 14 days, exposed to patients with fever or respiratory symptoms, exposed to suspected or confirmed cases).4–7 Chest CT and laboratory tests were performed to suspected cases. Once diagnosed, patients were referred to the infection department for consultation and isolated in a negatively pressurized room. Meanwhile, confirmed or suspected patients were reported to the infection controlling department and Hefei Centers for Disease Control and Prevention. Patients without COVID-19 infection were treated as soon as possible. After operations, patients were discharged early and recovered at home. Confirmed patients were treated, and operators took precautions for infection prevention. Suspected patients were treated as confirmed patients if their vital signs were unstable, otherwise, they were isolated until the diagnosis was confirmed or excluded. As the procedures were partly based on the patients’ statements, all patients were required to sign: Inpatient Epidemiological Investigation Commitment, Inpatient COVID-19 Initial Screening Questionnaire, and Spine Surgery Department on COVID-19 Epidemic Prevention Commitment.
For patients with suspected, confirmed, or unknown COVID-19 infection status, their COVID-19-related symptoms were generally treated before surgery to prevent increased surgical risk. If their vital signs were unstable and need urgent surgery they would be placed in a special designated operating room. Also, the operating room, the recovery room, and the access to the operating room were all separated and negatively pressurized. All of the essential apparatus in the operating room were wrapped by plastic wrappings, and all post-operative items, including single-use consumables, were handled exclusively. 8 All surgeons were trained in advance to put on and take off personal protective equipment (PPE) for self-protection. 9 There was a reduced stuff turnover and a reduced number of participants (students were excluded) during the operation. 8 The surgical team made the decision on the choice of open or laparoscopic approach to shorten the duration of the procedure and reduce the risk of exposure.
For health workers, the training contents covers basic knowledge of COVID-19 and prevention measures through a web-based platform. Training contents were adjusted in accordance with their work situation. The instructor in charge would answer their questions and hold online examination. For patients and their families, the COVID-19 related information was broadcasted in a continuous loop by a mobile nursing vehicle in the ward, including: wearing a mask, avoiding contact with other people and animals, when and how to wash hands, covering mouth with a tissue when coughing/sneezing), notifying the doctor in time if unwell, healthy diet, and good sleep. 7
The wards ran from east to west and the last two wards on the west side were converted into the isolation wards with additional monitoring and rescue equipment (Figure 2). The last two isolation wards were separated to receive only one suspected patient and three confirmed patients, respectively. Once the suspected patients were confirmed, they were sent to the confirmed isolation ward and the suspected isolation ward were disinfected. This is a feasible way to protect suspected patients. In addition, the original six-bed wards was converted into a three-bed room. Every ward was taken as an unit, patients, and their families were prohibited from entering other wards and were allowed to be accompanied by only one fixed family member. Moreover, they were required to wear masks, monitor the temperature twice a day and their diet were restricted to order in the hospital. What’s more, the Spring Festival and traffic control led to staff shortage, and some medical staff were selected to support the Wuhan in China. As a result, the hospital canceled the Spring Festival holiday, and workers returning from other cities were isolated for 14 days before returning to posts. Medical staff on duty wore surgical masks, disposable caps, and disposable latex gloves. When performing invasive operations or when there was a possibly contacting with the body fluids, they wore isolation gown and goggles and temperatures of all staff were taken twice a day. Medical resources were managed by administrative staff and distributed to critically ill patients first. The hospital also received medical resources and funds from the community.

Wards management. The wards ran from east to west and various zone were separated. As a provincial hospital, each department can normally treat 48 patients, but during outbreaks, the upper limit was only 22 patients (color should be used for this figures in print).
Additionally, quarantine and trauma are often associated with a negative psychological effects.10,11 We addressed the patients’ life issues, sent optimistic attitude towards life, and reducing their fears on COVID-19. In addition, the prevalence of psychological distress in quarantined healthcare workers was high and support from managers was essential to facilitating their return to work. 10 Therefore, it is important to rationalize their work content, workload, and rest time reasonably. Increasing their wages and improving educational resources for their children were another methods in China. For example, the salary of the medical staff supporting the Hubei have been tripled, and the children of medical staff who have made significant contributions or sacrifices will get extra points in college entrance exams or high school entrance exams.
Discussion
As the China’s existing cases have fallen below 3,000, China’s experience and efforts deserve the attention of other countries. In this paper, we categorized departments within hospitals into two main groups: high-risk and low-risk departments. They were categorized on the basis of whether the inpatient doctor was directly responsible for treating confirmed COVID-19 patients (including asymptomatic infected patients) or suspected patients, of which the directly responsible high-risk departments such as respiratory department, ICU, etc. Departments such as general surgery and orthopedics that may encounter COVID-19 as a result of emergency surgery or related invasive procedures are defined as low-risk departments because they are not directly responsible for the treatment of COVID-19, consultations in high-risk departments are often required, and only a small percentage of patients are in urgent need of surgery and are at risk of COVID-19 infection. Some of the auxiliary departments without in-patient were not considered, and some of them had high exposure risks: laboratory, radiology department, Doppler ultrasonic department, anesthesiology department, etc. We discuss coping strategies in a low-risk department using spine surgery as an example. In order to deal with the epidemic situation accurately and promptly, the epidemic prevention and control leading group has been set up, which was responsible for the overall implementation of plans and coordination of resources.
Meanwhile, in order to improve the treatment and prevent cross-infection between patients and medical staff, the hospital has improved treatment procedures. During the pandemic, hospital set up a separate fever clinic with physicians from the high-risk departments for patients with respiratory symptoms. For low-risk departments, there were two things that need to pay attention when receiving a patient: (1) whether the vital signs were stable; and (2) which department the patient should go. The vital signs were the most important thing that should focus on because it was directly related to patients’ lives and treatment procedures. If the vital signs were unstable, patients would be assigned to undergo the emergency surgery first and then they would need chest CT scan and laboratory tests, otherwise, the chest CT and laboratory tests were done first to rule out the COVID-19 infection. The emergency surgery was performed in the separated operating room, recovery room and even the access to the two rooms was separated, negatively pressurized, and disinfected timely. This step could avoid patients to be treated as suspected COVID-19 and live in the isolation ward once they came to the hospital, because these resources were limited. The second point allowed patients to receive specialist examination and treatment in time. Considering that many diseases require CT to aid in diagnosis, patients could receive CT of other body parts while doing chest CT, such as abdominal CT for general surgery department, avoiding multiple tests. Meanwhile, COVID-19-infected patients might first present with other symptoms, such as gastrointestinal symptoms, rather than respiratory symptoms. 12 Accordingly, prompt CT examination of the chest and other body parts in patients with other symptoms could both detect the disease and exclude COVID-19 (like chest and abdominal CT for acute abdomen). 13 The protective function of PPE for medical staff was irreplaceable, though it might lead to uncomforted feeling and difficulties for visibility and communications, resulting in the physician fatigue and decreased procedure completion. 9 Therefore, user-friendly equipment should be developed to solve these questions. Compared with before, minimally invasive surgery was chosen less often since aerosolization resulted from pneumoperitoneum and vapor caused by heat-generating cautery devices might increase the possibilities of spreading virus.14,15 Although this risk could be reduced through managing pneumoperitoneum and surgical smoke filtering systems, 16 the procedure was complicate and might increase healthcare system’s financial stress. 17 Therefore, it is essential to avoid diagnostic laparoscopies or laparoscopic approach with high chances of conversion to open procedures. 17 However, the minimally invasive surgery has the advantage of less trauma and faster recovery. Furthermore, given that there was no clear evidence indicating the risks of COVID-19 transmission, the minimally invasive surgery should not be discarded for this reason. 18
In addition, the hospital also provided health education to medical staff and patients for the purpose of raising their awareness of prevention and treatment and mastering correct protective skills on COVID-19. If there is a high percentage of COVID-19 infection in the population, the number of isolation wards can be increased and the layout of wards can be adjusted according to the situation of each hospital, and reduce the chance of cross-contamination. Psychological intervention played a significant role in reducing their distress during outbreaks and helped them to keep a positive mind. No patients or health workers were infected so far while ensuring the safety of the patients. Similar to the experience and practical recommendations from colorectal surgery in Italian, which can be categorized as low-risk department, they also reduced the risk of virus transmission by standardizing treatment procedures and strengthening the management of wards and operating rooms, which further increases the persuasiveness of this paper. 19 Since most of cities in China have controlled the virus, high-risk departments may take our measures as reference instead of the previous strict measures. To avoid cross infection in hospital, more infection prevention, and control measures that are based on sound scientific principles are needed. 20
Conclusion
A leading group, modification of treatment procedures, personnel education on COVID-19, wards rearrangement and psychological interventions for COVID-19 effectively have reduced the risk of nosocomial transmission between health workers and patients while providing optimum care. This was a feasible management approach for most low-risk departments, even in high-risk departments.
Footnotes
Acknowledgements
The authors thank all the participants and the nursing team of The First Affiliated Hospital of Anhui Medical University who helped to collect and organize the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.