
Abstract
The COVID-19 pandemic may cause psychological distress, changes in numbers and distributions of patients in spine surgery patients, which all affect the strategies of spine surgery treatment. These changes may be related to the number of new COVID-19 cases per day since they are visual indicators of the changes in the epidemic and are of interest to the public. This descriptive research took the spine surgery department as an example in a Grade-A tertiary hospital in Anhui province, China. The number and distribution of patients from January 24 to April 2, 2020 was collected and compared with the past 5 years. A psychological scale was constructed to assess the psychological distress of patients and the number of new COVID-19 cases per day in Anhui, China was collected each day from January 24 to April 2, 2020. Also, this research compared these variables with the emergency response or the number of new COVID-19 cases per day. All distributions dropped dramatically during first-level emergency response and then back to normal. The psychological distress of patients was relatively higher at the beginning of the outbreak and then gradually returned to normal. The trends between the psychological distress of patients and the number of new COVID-19 cases per day were similar. The number of new COVID-19 cases per day could be used to predict psychological distress, changes in patient numbers and distributions, which was beneficial for the department of spine surgery to adjust its treatment strategy during the epidemic.
Introduction
The emergence of Coronavirus Disease 2019 (COVID-19) and its subsequent spread have lived up to many warnings and caused an evolving global public health crisis. 1 According to the data of Chinese Center for Disease Control and Prevention, Anhui declared first-level emergency response (ER) on January 24, 2020 and down-regulated the level on February 25 and March 15, 2020. The ER means that during the epidemic the movement, transportation, and business were restricted and during the first-level ER, only emergency patients were allowed to go into the hospital. 2 And the number of new COVID-19 cases per day are the basis for the government to adjust the emergency response (ER).
For patients in spine surgery, they experience the double whammy of the epidemic and spine trauma. Current studies reported that the epidemic and trauma brought multiple new stresses, including physical and psychological health risks, isolation and loneliness, the closure of many schools and businesses, economic vulnerability and job losses, and even domestic violence.3–6 Hence, we collected the data of patient’s psychological distress in a Grade-A tertiary hospital in Anhui province, China from January 24 to April 2, 2020. During the epidemic, the official’s daily reports of new COVID-19 cases, which gained great attention, indirectly reflected the severity of the epidemic. These daily reports might have some potential psychological impacts on patients. On the other hand, with the decrease of new cases and the down-regulation of ER, the hospital began to treat patients with chronic diseases, causing the type of patients to change considerably and the number of patients increased rapidly. Meanwhile, patients’ psychological distress about the epidemic may also affect their decisions of seeing doctors (e.g. they are reluctant to go to the hospital for fear of cross-infection). Current literatures solely studied the coping strategies of spine surgery department or patients’ psychological distress during the epidemic. Considering the development trends of the epidemic, the strategies of spine surgery department and patients’ psychological distress were varying. This paper focused on whether the intuitive index, such as the number of new COVID-19 cases per day, can indirectly reflect patients’ psychological distress and the distribution and number of patients. The purpose of this research is to allow the department of spine surgery to develop a more reasonable and flexible guideline to cope with the change and treat patients while identifying their psychological distress during the epidemic based on the number of new COVID-19 cases per day. 7
Methods
A total of 505 patients with spinal diseases were included in the study from January 24 to April 2, 2020. Most patients were middle-aged (mean age 45.2 years), and the number of male patients were slightly more (273:232). The spine diseases were classified into acute (traumatic spine injuries) and chronic (spine degeneration, spine tumor, spine deformity) diseases. We then divided the data into four groups according to year: number of acute diseases in 2020 (acute 2020), number of chronic diseases in 2020 (chronic 2020), the mean number of acute diseases in 2015–2019 (acute) and the mean number of chronic diseases in 2015–2019 (chronic). The authors confirm that the ethical policies of the journal, as noted on the journal’s author guidelines page, have been adhered to. The ethical approval for this study was obtained from The Committee on Medical Ethics of the First Affiliated Hospital of Anhui Medical University. Written informed consent was obtained from all subjects before the study. The inclusion criteria followed the PICOS principle: (i) patients diagnosed with one of them: traumatic spine injuries, spine degeneration, spine tumor, spine deformity; (ii) patients who were admitted by the spine surgery department in a Grade-A tertiary hospital in Anhui province, China from January 24 to April 2, 2020; Exclusion criterion was: (iii) patients were unconscious to finish the scale. The distribution of patients were collected and they were asked to finish a psychological scale on the day of admission (Table 1) and the number of new COVID-19 cases per day in Anhui, China was collected from January 24 to April 2,2020. The trends between psychological scores and the number of new COVID-19 cases per day were compared according to the date. The study design was a descriptive research. Since the patients’ psychological distress was affected by both the epidemic and trauma and the patients’ quality of life varies according to ER, the existing scales cannot assessed the patients’ psychological distress comprehensively. Hence, a new scale was developed in this paper based on previous studies. In this new scale, the main indicators included the impact of the epidemic on life, the impact of trauma, and the history of psychiatric illness.3,8 The psychological scale (Table 1) was constructed and included items from previous studies, such as: fear of contagion and infecting family, 9 depression, 10 stress, 11 loneliness, 9 irritability, 12 insomnia, 12 stigmatization, 9 uncertainty, 9 post-traumatic stress symptoms, 13 inadequately treated mental disease, 14 and family history of psychiatric illness. 15 The total scores were ranged from 0 to 12. All statistical analyses were performed with GraphPad Prism v6.02 (GraphPad Software, Inc., La Jolla, CA, USA) and SPSS 19.0 software (SPSS, Inc., Chicago, IL, USA). The results were analyzed by Pearson correlation coefficient and the blank points were deleted before analyzed. p Values < 0.05 of the two-sided tests was defined as a statistically significant. The scores of the psychological distress were presented as mean ± deviation (SD). There were no patients for a few days and the mean ± SD value were blank on that day and the SD was blank if there were only one patient on that day.
The specific contents of the psychological scale.

Results
Distribution change
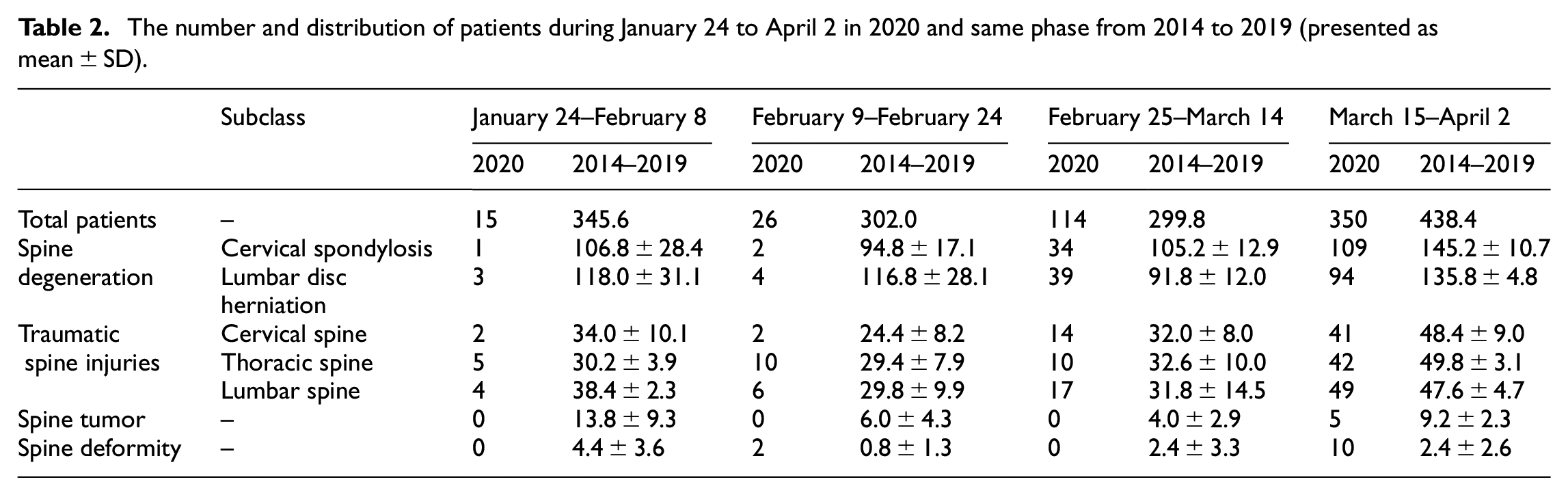
All distributions of patients dropped dramatically from January 24 to February 24 compared to the last 5 years in spine surgery department and then increased sharply (Table 2). The major turning point was noted from February 25 to March 14, which nearly increased fivefold. Until March 15 to April 2, the number of patients were 350, which was close to previous years (438.4). The variation of each subclass was small. It was notable that the chronic diseases changed in a wide range, which plunged to four from January 24 to February 8, 2020 and then boosted (Figure 1). The Pearson correlation coefficient between acute and chronic was 0.924 and p value < 0.01. The Pearson correlation coefficient between chronic 2020 and chronic was 0.754 and p value = 0.246. The Pearson correlation coefficient between acute 2020 and chronic 2020 was 0.995 and p value < 0.01. The Pearson correlation coefficient between acute and acute 2020 was 0.929 and p value = 0.071.
The number and distribution of patients during January 24 to April 2 in 2020 and same phase from 2014 to 2019 (presented as mean ± SD).

The comparison of acute and chronic diseases between 2020 and same phase from 2014 to 2019 (presented as mean ± SD).
The trends between the psychological scores and the numberof new COVID-19 cases per day
A total of 505 patients in spine surgery department were assessed using the psychological scale from January 24 to April 2, 2020. The results showed that the psychological scores of patients increased at first and then decreased, which means their psychological distress was higher at the early stage of the outbreak and then returned to normal gradually, but the scores were still above 2 (Figure 2). Similarly, the number of new COVID-19 cases per day first increased and then decreased in Anhui (Figure 2). The Pearson correlation coefficient between the psychological distress and the number of new COVID-19 cases per day was 0.752 and p value < 0.01. The psychological scores between female and male were analyzed and included a total of 232 females and 273 males. The trends between female and male were similar (Figure 3). The Pearson correlation coefficient between them was 0.965 and p value < 0.01. Similarly, subgroup of age and diseases classification showed little difference.
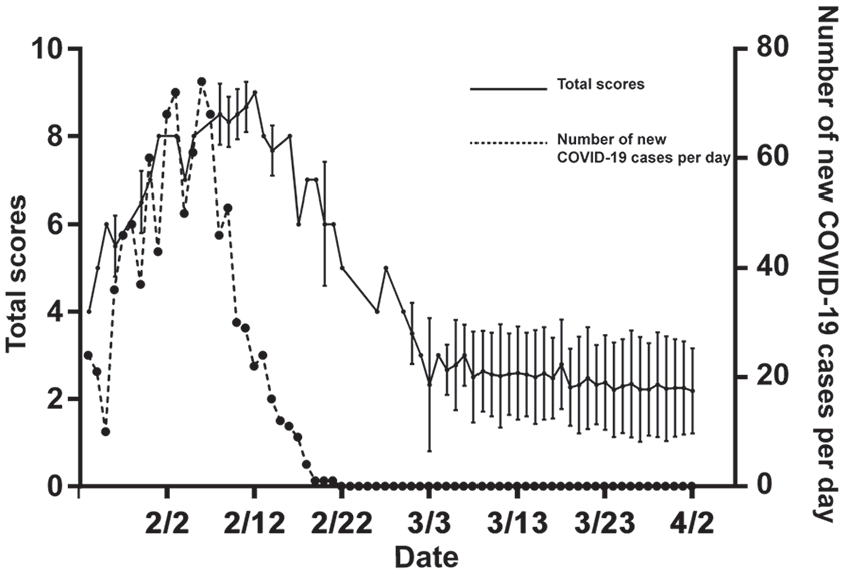
The average total points and the number of new COVID-19 cases per day varied with the date (presented as mean ± SD).

The average total points between female and male varied with the date (presented as mean ± SD).
Discussion
The epidemic of COVID-19 has turned the practice of spine surgery department upside down in just a few weeks. During first-level ER, all distributions of patients dropped significantly, since the movement, transportation and business were restricted, and only emergency patients were received in hospital. 2 Another reason may due to that patients’ fear of the cross-infection in hospital. Therefore, elective surgery for non-urgent/emergent conditions decreased worldwide.16,17 However, loss of employment due to the epidemic may be a confounding factor for limited inflow of the patients who had difficulty affording treatment. Patients whose elective surgery was postponed due to the epidemic, specifically older patients with medical comorbidities, may be at increased risk of progressing to a severe and potentially fatal stage because the hospital could not treat them further during this special time. 17 Additionally, at the beginning of the outbreak, the number of medical workers was drastically reduced since many medical resources and staff were transferred to Wuhan, Hubei Province, China. Also, it is because some staff was required to quarantine in the field after returning to their hometowns during Chinese New Year. Simultaneously, the number of patients was greatly declined and the distribution was acute diseases. The staff remaining in the hospital had different clinical experience, so these factors should be taken into account and planned for when redeploying, in order to maximize patients’ outcomes and safety and minimize the use of medical resources.17,18 When the number of new COVID-19 cases per day gradually decreased to zero, the ER was regulated downward and the department of spine surgery began to receive patients with chronic diseases. The number of patients with chronic spinal diseases increased dramatically because the previous epidemic led to the delayed treatment, causing more pressure on the spine surgery department. Besides, people’s daily activities increased gradually, which resulted in the growth of the number of patients with accidental acute spinal injuries (previously, there were fewer cases due to quarantine). Moreover, medical resources and staff supporting the Wuhan returned to the department of spine surgery, during which time spine surgery will need to treat more chronic patients. Notably, the figures of psychological scores and the number of new COVID-19 cases per day showed similar trends, which was a trend of rapid increase, followed by a gradual decrease and finally stabilization. This change might result from patients’ moderate-to-severe psychological distress during the initial phase of the COVID-19 outbreak, 19 and they became less afraid after implemented the strict and effective epidemic containment measures. However, their scores of psychological distress did not decrease to zero, which might be due to some patients’ fear of resurgence of the COVID-19 or due to worried about their spinal disease. Nevertheless, the relationship between these two elements required further research to verify.
Recent studies reported that the quarantine and trauma related psychological distress should not be ignored, which may adversely affect the course of the disease, the treatment process, and reduce quality of life.8,20,21 These factors may have significant and deleterious effects on the mental health of individuals at risk of psychological illness as well as healthy individuals with no previous history of psychological illness in spine surgery department, and it was extremely important to identify and intervene early.19,22 The number of new COVID-19 cases per day was a potential predictor for detecting psychological distress, and it was easily available. However, when the epidemic lasted longer, its predictive value may decrease even if the number of new cases is large as patients may adapt to the epidemic. After identifying their psychological distress, more humanistic approaches are required, including solving their problems in life, sending positive and optimistic attitude towards life and reducing their fear on COVID-19 as well as cognitive behavior therapy.19,23
In the present study, we took the spine surgery department as an example to investigate the psychological distress of patients, the number and distribution of patients, yet patients in other departments may encounter a similar situation. Similar to the spine surgery department, many departments, such as general surgery and cardiac surgery, have clear distinctions between patients with acute and chronic conditions, and all of them only treated emergency patients during the first-level ER. They began to accept all types of patients as the outbreak subsides. Meanwhile, China has got the virus fully under control while the epidemic in many other countries were becoming much worse. In contrast to the trend that the gradual decrease in new COVID-19 cases and the gradual increase in spinal surgery patients mentioned in this study, new cases had been continually rising in most countries before the advent of the vaccine. Take the United States as an example, American College of Surgeons advised to halt elective surgery on March 13, 2020 and New York State suspended all elective surgery on March 23, 2020. However, the continual exacerbation of the epidemic resulted the patients of elective surgery accumulate, Syosset Hospital (dedicated primarily to elective surgery) decided to resume the elective surgery on May 13, 2020. Also, they adopted some new strategies to prevent infections in hospitals, such as the education and evaluation for admission, unaccompanied hospitalization, and the postoperative prescriptions before discharging. 24 In addition, virtual medicine practices were being rapidly applied and it could become part of the “new normal” for surgeons in the post-pandemic. 25 It is because it increases access to care for rural/long distance patients, provides societal cost savings, reduces chances of interactions, and increases patient convenience. 26 However, the exacerbation of the epidemic, elective surgical hospitalizations without family members accompany, 24 or the difficulty of reimbursement for telemedicine 26 can negatively influence the mental health.
Our study had some limitations. First, only spine surgery department in a Grade A tertiary hospital in Anhui, China was studied, which means the representativeness was poor, and there might be some bias and limitations in the research population. The applicability of the findings to patients diagnosed in other regions needs to be further explored. Second, the methods used in this study did not provide strong evidence, which made it hard to support the conclusion. Third, the study did not focus on the impact of secondary outbreak. Forth, this paper did not adopt the existing scale, such as Event Scale-Revised (IES-R), which has been well-validated in the Chinese population, to evaluate patients’ psychological distress after exposure to the public health issues for a week. 27 Because of this, the result of this research might be less comparable with other studies. Fifth, this paper only studied patients who met the inclusion criteria during the epidemic and did not calculate a minimum sample size, limiting the credibility of the conclusions.
Conclusion
The number, distribution and psychological distress of spine patients were affected by the outbreak, which showed a similar trend with the number of new COVID-19 cases per day. This was the trend of rapid increase, followed by a gradual decrease and finally stabilization. Based on this trend, the department of spine surgery could develop a flexible approach to respond to changes in the number and distribution of patients and identify patients at risk for psychological distress in a timely manner. Except for the department of spine surgery, this phenomenon might occur in other departments, such as the general surgery and cardiac surgery. However, these points required further study to identify.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from The Committee on Medical Ethics of the First Affiliated Hospital of Anhui Medical University (APPROVAL NUMBER/ID: Quick-PJ 2021-02-11)*.
Informed consent
Written informed consent was obtained from all subjects before the study.