
Abstract
Background:
There are few randomised prospective data or guidelines for the treatment of neuroendocrine cervical cancer (NECC). In addition, the role of radiotherapy (RT) in NECC remains controversial. We used the Surveillance Epidemiology and End Results (SEER) database to investigate the role of RT for the treatment of NECC. Particular attention was paid to the different role of RT in patients with or without a metastasis (M1 or M0).
Methods:
The SEER database was queried for studies on NECC. We limited the year of diagnosis to the years 2000 to 2015. A Pearson’s two-sided Chi-squared test, the Kaplan–Meier method and Cox regression analysis models were used for statistical analyses. The overall survival (OS) was studied for the overall group and between-subgroup groups.
Results:
NECC was an aggressive disease with a mean OS of only 46.3 months (range of 0–196 months, median of 23 months). No significant differences were shown between the surgery (S) and S + RT groups (p = 0.146) in the M0 (without metastasis) arm. However, there was a statistically significant difference in OS between the S and S + RT groups in the M1 (with metastasis) arm (median of 44.6 months for the S group and 80.9 months for the S + RT group), p = 0.004. The mean survival was significantly longer for M0 patients than for M1 patients when treated with S only (S arm), that is, 82.1 months versus 44.6 months, respectively (log-rank p = 0.000). We also noted that when patients received adjuvant RT (S + RT arm), there were no significant differences between the M0 and M1 groups (median of 90.6 and 81.0 months, p = 0.704, respectively). Age at diagnosis, chemotherapy, T stage and N stage were significant factors for OS in the M0 arm. Interestingly, radiotherapy was the only significant factor for OS with a multivariate HR for death of 0.502 (95% CI 0.206–0.750, p = 0.006) in the M1 arm.
Conclusions:
RT may be carefully used in patients who are negative for metastases. Using SEER data, we identified a significant survival advantage with the combination of radiotherapy and surgery in NECC with metastases. This suggests that active local treatment should be conducted and has a significant impact on OS, even if a distant metastasis has occurred.
Introduction
Neuroendocrine cervical cancer (NECC), accounts for less than 3% of all cervical cancers,1,2 but is highly aggressive, with lymph node metastasis and distant metastasis occurring at early stages. 3 Small cell neuroendocrine carcinoma is the most common type and is highly aggressive. Moreover, poorly differentiated neuroendocrine tumours occur in more than half of NECC cases. 4 Moreover, no clear recommendations were currently available for the treatment strategy. 5 In the SEER study, 5-year OS for NECC was worse compared to that of squamous cell carcinoma and adenocarcinoma. 6 NECC was indeed a therapeutic challenge for the gynecologic oncologist.
Based on the pathological and biological behaviours of NECC, and many clinical research results,5,7 chemotherapy is the preferred treatment. However, the role of radiotherapy (RT) in NECC remains controversial.1,8 One study reported that during the early stage of NECC with a negative lymph node metastasis, radiotherapy should be carefully selected. 1 However, Stecklein et al. 2 discovered that concurrent chemoradiotherapy was better than surgery for the early stage of NECC with a negative lymph node metastasis. Cohen et al. 9 reported that the use of adjuvant chemotherapy or chemoradiation was associated with a higher survival in small cell cervical cancer patients. Although studies have analysed both early and late stages, they have focused on chemotherapy and have not independently analysed the effects of RT. In addition, all of the above studies had a limited number of patients. The role of RT remains a subject of debate; moreover, there have been even fewer published studies regarding whether distant metastases occur. Given the scarcity of the literature and the rare incidence of NECC, we conducted a surveillance, epidemiology and end results (SEER) database analysis to understand the potential role of RT in the treatment of this malignancy. Moreover, the focus of this study was on the role of RT for OS in patients with or without a distal metastasis.
Materials and methods
Patient and public involvement
We explored the National Cancer Institute’s SEER program to identify NECC upon diagnosis. The SEER program is the largest publicly available cancer dataset in the world. Because SEER is a public database without identified information, our study was exempt from approval by the ethics commission of the First Affiliated Hospital of Zhengzhou University. This research was conducted without patient involvement. Patients were not invited to comment on the study design and were not consulted in the development of the patient-relevant outcomes or the interpretation of the results. Patients were also not invited to contribute to the writing or editing of this document for readability or accuracy.
Data collection
The study data and related clinical information on NECC were obtained from the SEER program. The database (Incidence – SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975–2016 varying)) from SEER*Stat (version 8.3.5) was used to identify patients with NECC diagnosed between 2000 and 2015. The following were selected: (1) C53.0-Endocervix, C53.1-Exocervix, C53.8-Overlapping lesion of cervix and C53.9-Cervix uteri as the primary sites; (2) 2000 to 2015 for the year of diagnosis and (3) International Classification of Diseases for Oncology (ICD-O-03) histology codes of carcinoid (8240/3), atypical carcinoid (8249/3), large-cell neuroendocrine carcinoma (8013/3) and small cell carcinoma NOS (8041/3). The clinical and pathological factors, including age, differentiation degree, race, marital status at diagnosis, stage, year of diagnosis, vital status recode and SEER cause-specific death classification were screened.
Neuroendocrine cancer arises from neural and endocrine cell types and can occur throughout the body, and varies widely in its clinical presentation and characteristics. In this study, we set the research time between 2000 and 2015. In addition, the ICD-O-03 classification criteria refer to the 2014 WHO classification of tumours of female reproductive organs with neuroendocrine tumours (NETs). The carcinoid-type was generally considered to be well-differentiated. Albeit, it was found to be rare in NECC. As we found in this research, there were only there cases of carcinoid in 759 NECC. Small cell neuroendocrine carcinoma and large cell neuroendocrine carcinoma are the most common types of NECC. Therefore, we studied only the two aggressive and poorly differentiated NECC.
Statistics
All statistical calculations were conducted using SPSS (version 25.0). We used a Pearson’s two-sided Chi-squared test to compare each parameter between surgery only (S) and radiation with surgery (RT + S). The Kaplan-Meier method was used for a single-factor correlation analysis of survival and to compare the survival rates between subgroups. A cox regression analysis was used for univariate and multivariate survival analyses to evaluate the effects of various parameters on the overall survival (OS). The OS was defined as the time from diagnosis to death from any cause. Using cut-off values of the Kaplan–Meier survival analysis, the survival probability was compared between the matched population. Differences were considered statistically significant at p < 0.05.
Results
Patient characteristics
Of the 759 patients with NECC identified in the database, excluding ‘multi-source carcinoma’, and ‘carcinoid’, as well as patients for whom the RT status, differentiation grade and TNM stage were unknown, a total of 494 patients remained. The mean age at diagnosis was 49.7 years (range, 21–92). More white patients were diagnosed compared to non-whites (white/nonwhite = 2.57). Of the 494 cases, 16 (3.2%) were well or moderately differentiated, 478 (96.8%) were poorly differentiated or undifferentiated. Poorly differentiated and undifferentiated cells accounted for more than half of the number. The majority of the patients extracted from the database had an early tumor stage (T stage) of the disease, 362 (73.3%) patients were characterised as T1 or T2 and 132 (26.7%) were characterised as T3 and T4. Compared with the lower distant metastasis rate (26.3%), the lymph node metastasis rate was higher (46.2%). More interestingly, patients with a distant metastasis tended to have a higher T stage (46.9% vs 53.1%, p = 0.000) and N stage (26.2% vs 73.8%, p = 0.000), as shown in Table 1. NECC in the uterine cervix was an aggressive disease with a mean OS of only 46.3 months (range of 0–196 months, median of 23 months). There was a slight increase in the annual number of cases (p < 0.001). Moreover, as the time passed, an increasing number of patients had metastasised at the time of diagnosis (59.2 vs 41.8, p = 0.001) (Table 1).
Patient demographics.
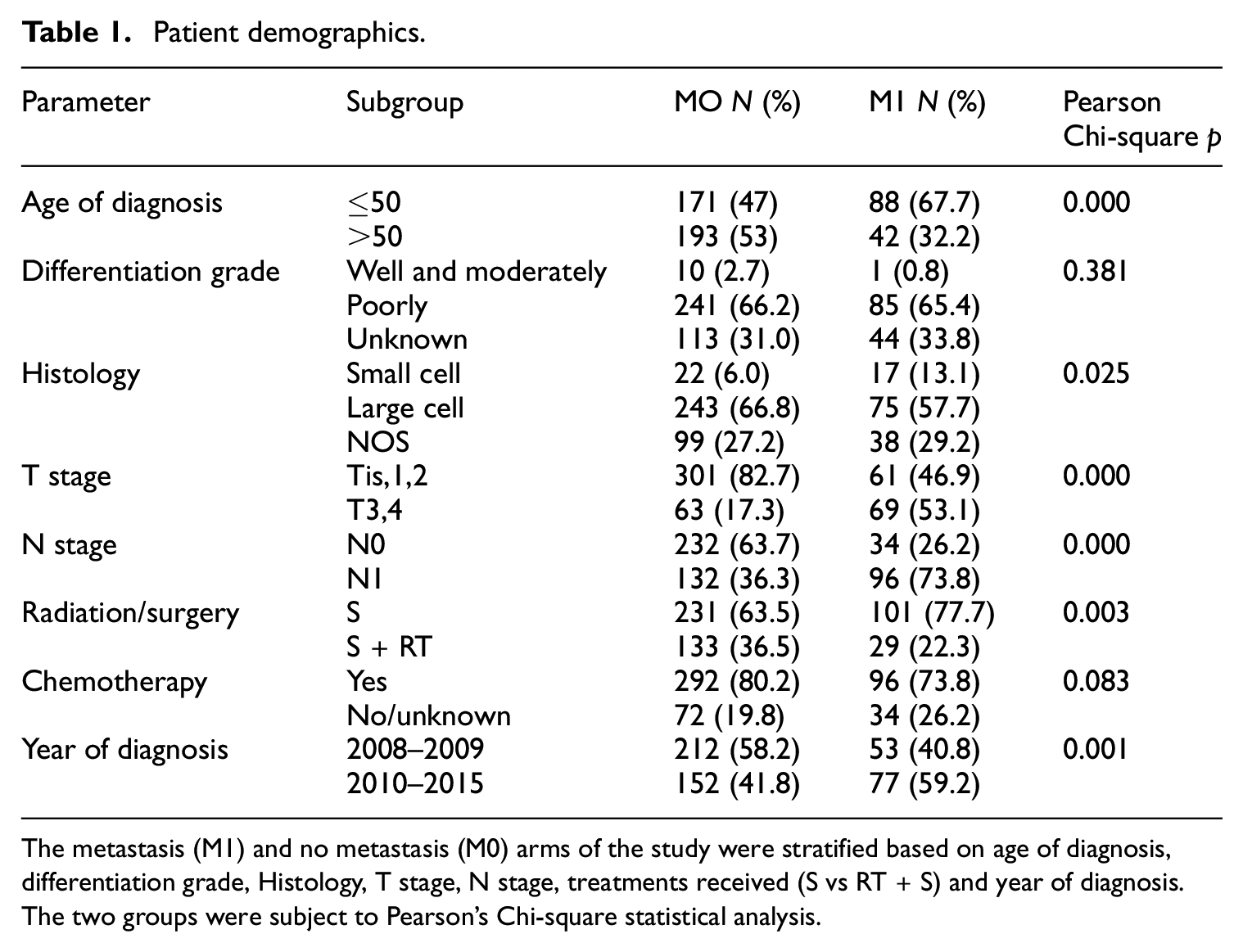
The metastasis (M1) and no metastasis (M0) arms of the study were stratified based on age of diagnosis, differentiation grade, Histology, T stage, N stage, treatments received (S vs RT + S) and year of diagnosis. The two groups were subject to Pearson’s Chi-square statistical analysis.
Although it was not known whether the patients were voluntary or passive, none opted for radiotherapy alone, most patients, that is, 332 (67.2%), chose to undergo surgery alone, and 162 (32.8%) were chosen for surgery combined with radiotherapy. In particular, when distant metastases occurred, fewer patients chose radiotherapy (22.3% vs 36.5%, p = 0.003).
Effects of RT on patients with NECC
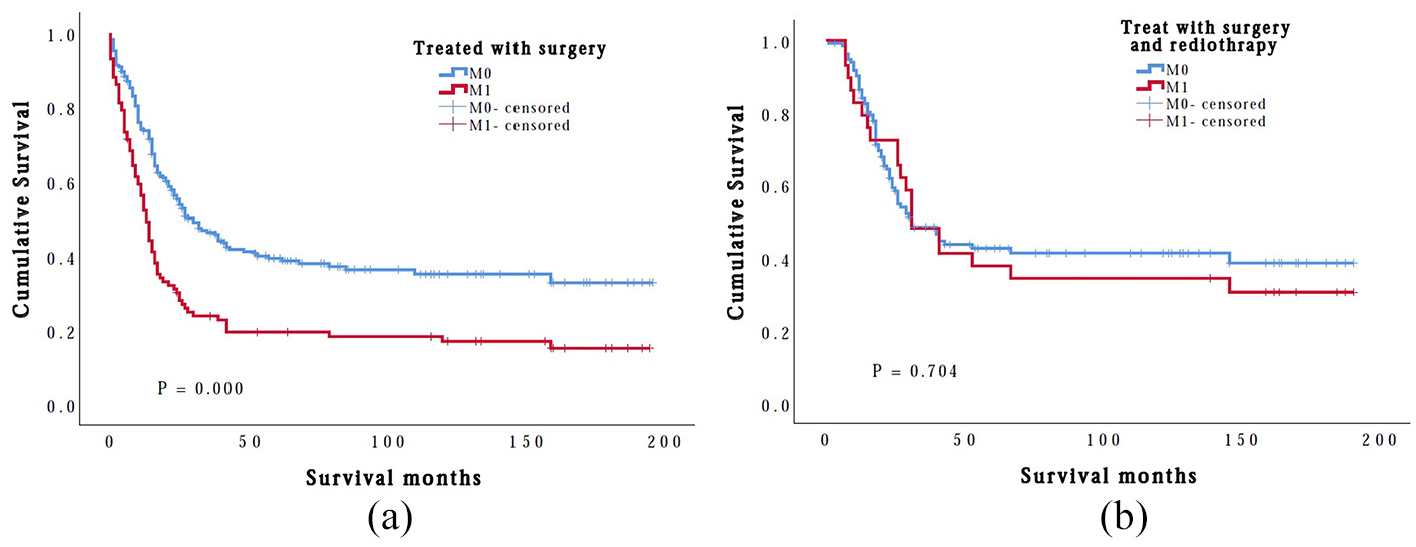
The OS between the two groups differed significantly, with a median survival of 86 months for the M0 group versus 53 months for the M1 group (p = 0.000) (Figure 1). Because we were interested in analysing the therapeutic effects of RT on patients with NECC, we chose to divide the patients according to the type of treatment (S vs S + RT) in the two arms (M0 and M1), respectively. The patient cohort had 231 patients treated with surgery (S group) and 133 patients who underwent surgery with radiotherapy (S + RT group) in the M0 arm. There were no significant differences between the S and S + RT groups (p = 0.146), as shown in Figure 2(a). Patients who were treated with RT had a 1 year OS rate of 86.4% compared to 73.7% for patients who were not treated with RT. Interestingly, in the M1 arm, there were 101 patients treated with S (S group) and 29 patients underwent S with RT only (S + RT group). There was a statistically significant difference in OS between the two groups (median of 44.6 months for the S group vs 80.9 months for the S + RT group, p = 0.004). Patients who were treated with RT had a 1 year OS rate of 79.3% compared to 52.2% for patients who were not treated with RT (Figure 2(b)). To further illustrate the effect of RT, using cut-off values of the Kaplan–Meier survival analysis, the survival probability was compared between the M0 and M1 groups when receiving the same treatment (S or S + RT), respectively. When patients were not treated with RT (S arm), the OS between M0 and M1 groups differed significantly, with a median survival of 82.1 months for the M0 group versus 44.6 months for the M1 group (p = 0.000), as shown in Figure 3(a). When patients received RT (S + RT arm), there was no significant difference between the M0 and M1 groups (median of 90.6 months vs 81.0 months, p = 0.704) (Figure 3(b)).

Kaplan–Meier plot of NECC cases with (M1) or without (M0) metastasis. OS between the two groups differed significantly, with median survival of 86 months for the M0 group versus 53 months for the M1 group (p = 0.000).

The patient cohort had 231 patients treated with surgery (S group) and 133 patients who underwent surgery with radiation (S + RT group) in the M0 arm. There were no significant differences between the S and RT + S groups (p = 0.146) (a). There was a statistically significant difference in OS between the two groups (median 44.6 for the S group vs 80.9 months for RT + S group, p = 0.004) in the M1 arm (b).
When patients were not treated with radiation (S arm), OS of the M0 group was significantly longer than that of M1 group (a). When patients received radiation (S + RT arm), there was no significant difference between the M0 and M1 groups (p = 0.704) (b).
Independent prognostic factors for NECC
Based on the above results, to further illustrate the influence of RT on OS and to identify more independent prognostic factors for high-risk patients, we conducted a multivariate Cox regression analysis, as shown in Table 2. Potential prognostic parameters such as age at diagnosis, T stage, N stage, M stage, race, marital status, differentiation grade, histology, surgery, radiotherapy, chemotherapy and year of diagnosis were evaluated. A multivariate Cox regression analysis showed that age at diagnosis, chemotherapy, T stage and N stage were significant risk factors for OS in the M0 arm. Interestingly, among surgery, radiotherapy, chemotherapy, age at diagnosis, year of diagnosis, histology type, grade, race, N stage and T stage, radiotherapy was the only significant factor for OS with a multivariate HR for death of 0.502 (95% CI 0.206–0.750, p = 0.006) in the M1 arm.
Multivariate Cox regression analysis of prognostic factors for OS in the matched population.
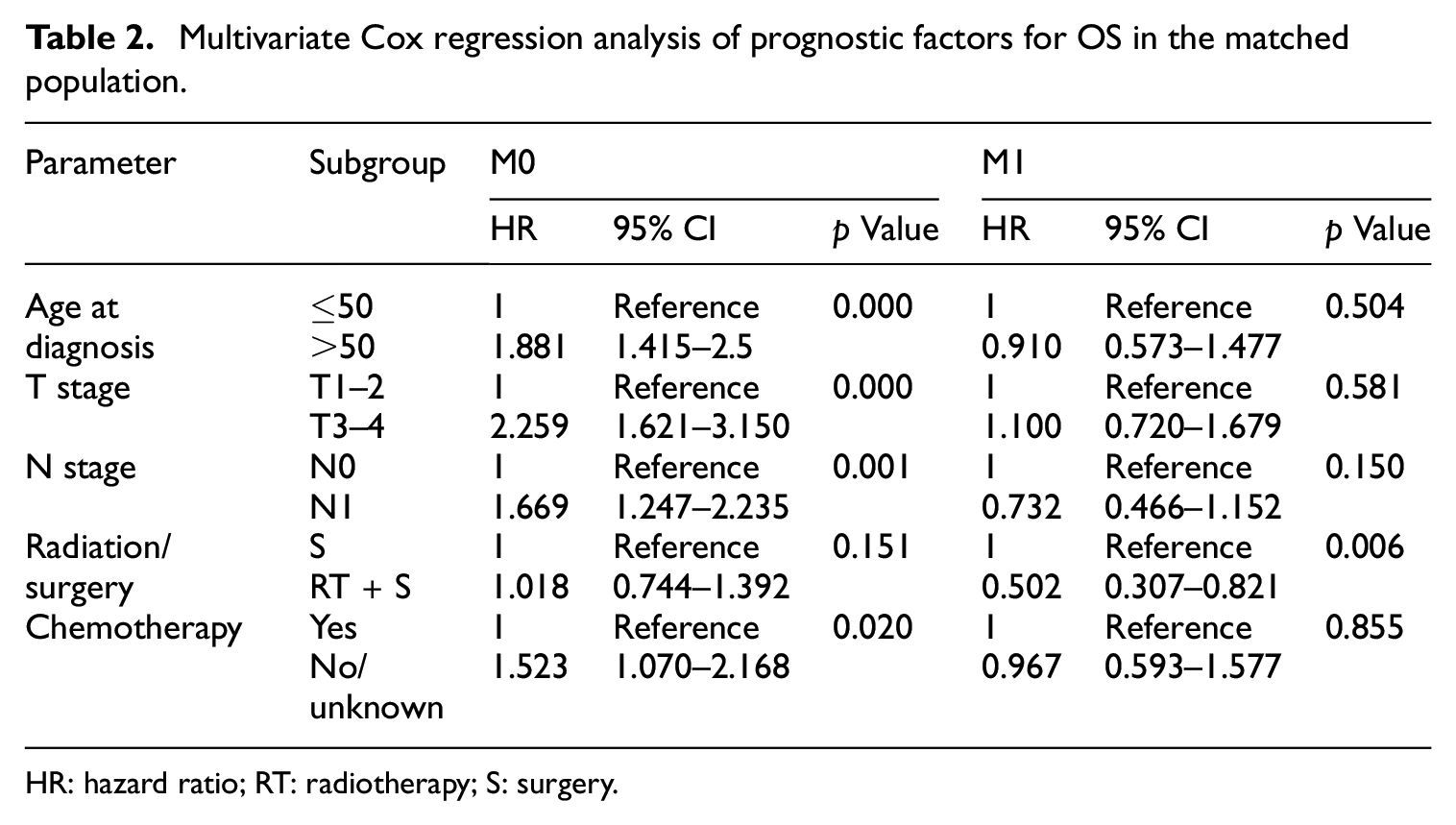
HR: hazard ratio; RT: radiotherapy; S: surgery.
The role of surgical types
There were four main types of surgery: local tumour destruction or excision (55/494), total hysterectomy (simple, pan-) without removal of tubes and ovaries (91/494), total hysterectomy (simple, pan-) with removal of tubes or ovary (116/494), modified radical or extended hysterectomy (232/494). In general, there was no significant difference in survival among the various surgical methods (Supplemental Figure), p = 0.769.
Discussion
NETs derive from neuroendocrine cells, and typically locate in the gastrointestinal tract, pancreas and lungs. NECC is rare, and various studies have shown rates of approximately 0.9% to 3%, although the incidence rate has an upward trend.1,2,10 As noted, there was a slight increase in the annual number of cases (p < 0.001). Moreover, with the passage of time, an increasing number of patients have metastasised at the time of diagnosis (59.2% vs 41.8%, p = 0.001), as shown in Table 1. Therefore, researches on NECC have gradually increased in recent years. This was not the first paper to look at the clinical-pathology and survival data to NECC. However, to the best of our knowledge, this was the first study to focus on the role of radiotherapy for OS in NECC patients with or without distal metastasis using a large population-derived database of the SEER system.
NECC was a relatively rare pathological type of cervical malignant tumour, which was highly invasive and could rapidly lead to metastasis. As shown in Table 1, although the majority of patients extracted from the database had an early T stage of disease, poorly differentiated and undifferentiated patients accounted for more than half of the number. When diagnosed, 26.3% led to a distant metastasis, and 46.2% led to a positive lymphatic metastasis. Distant and lymphatic metastasis could occur during the early T stage, with a poor prognosis, which was consistent with previous reports. 11 We also discovered that the histology type was not a prognostic factor regardless of whether the patient had a distant metastasis or not, with a multivariate HR of 0.971 (95% CI 0.871–1.083, p = 0.599) and 0.942 (95% CI 0.821–1.812, p = 0.399). The differentiated grade was also not a prognostic risk factor, with a multivariate HR of 0.978 (95% CI 0.742–1.288, p = 0.872) and 0.843 (95% CI 0.542–1.304, p = 0.442) in patients with or without a distant metastasis, respectively. As a reason for this, a large number of cases were high-grade NETs. High-grade NETs, whether small- or large-cell type, were the most and second-most common and aggressive subtypes of NECC. 11 They displayed an extremely aggressive biological behaviour, with an extremely high propensity for metastasis and positive lymph nodes, 12 which was consistent with previous reports in the literature.3,13
Our study confirmed the aggressive nature of NECC. Because of its rarity, there was no prospective data or only limited retrospective data to guide its treatment. The benefit of adding adjuvant RT after radical hysterectomy is controversial at present, as the Society of Gynecologic Oncology (SGO) and Gynecologic Cancer Intergroup (GCIG) have reported.7,12 As shown in Table 1, radical surgery was recommended for 332 (67.2%) patients, and only 162 (32.8%) patients were administered adjuvant radiotherapy. Many studies have demonstrated that radical hysterectomy was an effective therapeutic option in NECC, but experience with adjuvant RT had been limited and had shown mixed results. 14 One study reported that during the early stage of NECC with a negative lymph node metastasis, RT should be carefully selected. 1 However, Stecklein et al. 2 discovered that concurrent chemoradiotherapy was better than surgery during the early stage of NECC with a negative lymph node metastasis. Cohen et al. 9 reported that the use of adjuvant chemotherapy or chemoradiation was associated with higher survival in small cell cervical cancer patients. In addition, the above studies had limited patients. Using SEER data, 759 patients with NECC were identified in the database, and a total of 494 patients with a clear TNM stage and clinical features remained. The mean OS of NECC was only 46.3 months (range of 0–196 months, median of 23 months). There were no significant differences between the S and S + RT groups (p = 0.146) in the M0 arm. Interestingly, we noted a statistically significant higher OS for those who received RT in the M1 arm (median of 44.6 for the S group vs 80.9 months for the S + RT group, p = 0.004). The mean survival was significantly longer for patients without metastases than for patients with metastases when the patients were treated with S only (S arm), at 82.1 months versus 44.6 months, respectively (log-rank p = 0.000). However, when patients received RT (S + RT arm), there was no significant difference between the M0 and M1 groups (median 90.6 months vs 81.0 months, p = 0.704). Given these facts, in the early and locally advanced stages of the disease, RT did not provide survival benefits. However, RT may bring about survival benefits to NECC patients with a distant metastasis, which differed from the results of adenocarcinoma of the uterine cervix. 15 This suggested that an active local treatment should be applied and may have a significant impact on the OS even if a distant metastasis had occurred. As P.J. Hoskins reported, a combined-modality regimen of involved-field irradiation with concurrent chemotherapy could successfully treated small-cell carcinoma of the cervix in approximately 55% of patients. 16 The centre for personalised cancer therapy at UC San Diego Moores Cancer Center reported a patient with metastatic, chemotherapy-refractory neuroendocrine carcinoma manifested near-complete systemic resolution of disease, ongoing at 10+ months, when she was prompted treatment with stereotactic body radiation therapy (SBRT) combined with anti-programmed cell death protein 1 antibody. 17 In our study, palliative RT might affect the long term prognosis for patients with M1 disease. In addition, radiotherapy was the only significant factor for OS in the M1 arm. However, The SEER database did not provide the information of the dose of radiation or the size of the radiation fields. Whether the addition of radiotherapy could improve OS for NECC patients with M1 disease remained controversial. Large database studies with detailed information were required to answer these questions.
Many authors had investigated or supported the use of chemotherapy as a part of a multimodality treatment approach for NECC over the last 20 years.4,5,9,18,19 In the multivariate analysis of our study, the chemotherapy was a significant risk factor for OS in the M0 arm, but not in the M1 arm. However, the information about chemotherapy regimens and combination with radiation were unclearly in the SEER database. So, the analysis about treatment regimens including chemotherapy will have big bias and led to poor credibility. And, we did not analyse the effect of different chemotherapy regimens on the survival of NECC patients in our study.
Age at diagnosis, chemotherapy, T stage, N stage were significant factors for OS in the M0 arm, among S, RT, chemotherapy, age at diagnosis, year of diagnosis, histology type, differentiation grade, race, N stage and T stage, which was consistent with previous studies.10,14,18 Interestingly, RT was the only significant factor for OS with a multivariate HR for death at 0.502 (95% CI 0.206–0.750, p = 0.006) in the M1 arm. Active local RT may provide survival benefits to patients with distant metastasis, with no previous studies reported. Notably, there was non-significant difference on the survival rate among patients receiving various surgical treatments, which needs to be further validated in prospective studies.
It is also important to consider the limitations of using this retrospective SEER analysis to draw strong correlative conclusions. We have no way to know the exact radiation dose, dose fractionation or radiation location. We do have faith that aggressive local treatment should not be abandoned, however. Therefore, the most important aspect is to conduct a randomised trial for patients with NECC. Our study has other limitations that should be noted. The tumour size, parametrial extension, lymph-vascular space invasion, smoking and human papillomavirus (HPV) infections were clearly interrelated with treatment effects, such as squamous cell carcinoma of the cervix.10,14,18 Although associated-data were unavailable from the SEER database, our findings are consistent with many clinical findings, that is, T stage, N stage and distant metastasis are independent prognostic factors.
Conclusions
Given the scarcity of studies conducted on the treatment of NECC, we analysed patients with NECC from the SEER database in the United States for the years 2000 to 2015. We were interested in the effects of RT on OS in patients with NECC. Chemotherapy has been shown to be beneficial in NECC. However, the role of RT in NECC remains controversial. Our analysis results revealed a significant survival benefit to patients with a metastasis who received RT. RT was the strongest prognostic for OS of NECC patients with a metastasis. This suggested that an active local treatment should be applied even if distant metastasis occurs. Although this SEER analysis had certain limitations, such as a lack of chemotherapy regimens information, it provided guidance on how to manage this rare and aggressive form of cancer. We hope that these findings may influence future prospective studies in establishing a standard treatment regimen and optimal local management for NECC.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504211009336 – Supplemental material for The role of radiotherapy in neuroendocrine cervical cancer: SEER-based study
Supplemental material, sj-pdf-1-sci-10.1177_00368504211009336 for The role of radiotherapy in neuroendocrine cervical cancer: SEER-based study by Meilian Dong, Xiaobin Gu, Taoran Ma, Yin Mi, Yonggang Shi and Ruitai Fan in Science Progress
Footnotes
Author contributions
MD and RF collected and analysed the data, and wrote the paper; MD, XG and MT analysed the data; YM, YS and RF conceived and designed this study, and analysed the data, and all authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Key Scientific Research Projects of the Universities in Henan Province (No. 19A320036).
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.