
Abstract
Given that stroke is an indispensable health burden in Saudi Arabia and around the world, great importance has been attached on studies of social support and other factors that could improve the quality of life of stroke survivors. Perceptions of quality of life and social support may vary depending on patients’ cultural and societal background. This research assessed the quality of life and social support of community-dwelling Saudis who survived stroke. A quantitative study was performed among 123 Saudi stroke survivors. Questionnaire-guided interviews measuring social support and quality of life were performed, and the multivariate effects of predictor variables on the four domains of quality of life were determined through multivariate multiple regression analysis. Among the dimensions of social support, support from family members had the highest average, whereas support from friends had the lowest. The environmental domain of quality of life was perceived to be the best aspect, whereas physical health was perceived to be the poorest. Multivariate analysis revealed that age, gender, employment status, monthly family income, type of community, education, type of stroke, side of stroke and support from significant others had multivariate influences on the domains of quality of life. Several sociodemographic and disease-related variables and social support influence patients’ quality of life. The study adds critical knowledge as to how Arab stroke survivors perceive their quality of life and social support. Ensuring that stroke survivors receive adequate social support is imperative because it can improve their quality of life.
Introduction
Identified as a major health burden worldwide, stroke is one of the major chronic diseases that should be addressed by local and international healthcare organisations. In 2017, the number of new stroke cases reached 11.9 million globally. 1 In Saudi Arabia, stroke is growing in prevalence and has become a major contributing factor for mortality. 2 The Ministry of Health of Saudi Arabia reported that stroke in the country has a prevalence of 29 cases per 100,000 of the population annually. 3 Stroke survivors are highly likely to develop various complications related to ineffective neuromuscular functions. Among the neurologic problems associated with stroke are paralysis, reduced body balance and motor functions, dysphasia and slurred speech, visual problems, and bowel and bladder challenges.
In addition to the consequences of stroke as an initial disease, immense change in personality aspect and reduction in quality of life (QOL) can be expected. Physical and social crises caused by disability after a stroke episode have considerable effects. Therefore, evaluating the QOL of stroke survivors is important. 2 QOL is people’s ‘perceptions of position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’. 4 The measurement of QOL during stroke therapy is becoming a common practice. A comprehensive and holistic image of recovery can be assessed through the evaluation of QOL given a wide range of clinical manifestations related to stroke.
The overall QOL of a patient who experienced initial stroke is influenced by his or her independence in basic day-to-day functions, neurologic status and mental health problems. 5 The findings seem to be in agreement with a previous study that investigated patients who suffered stroke 6 months before their study. 6 In addition to the predictors of stroke patients’ QOL, advanced age, illiteracy, joblessness, low household income and increased severity of illnesses contribute to poor QOL. 7 This finding agreed with previous results that showed sociodemographic characteristics, severity of stroke, presence of disability and depression negatively influence the QOL of stroke survivors. 8 QOL in stroke patients is lower in Saudi Arabia than that in other developed nations. 2
In relation to the high incidence of stroke and its consequences, social support for stroke patients is of great importance to the extensive recovery of functional status as it positively affects QOL. 9 The concept of social support has been reflected in studies on health and well-being. It was defined as ‘the availability or provision of a relationship, information or assistance that empowers a person to manage his or her day-to-day life effectively in the presence or absence of a crisis’. 10 This information is evidenced by a specific finding that patients who received support from families and friends results had high QOL, specifically in the physical and mental domains. 11 Furthermore, social support mediates between a patient’s functionality and QOL. 9
An individual’s QOL is influenced by culture and societies. 12 QOL is dependent on an individual’s cultural background and the values of the society, which affects the specific goal, expectation and standards of a person. 4 Past studies have argued the significance of considering the cultural background of an individual in the study of QOL, given that perceptions of QOL differ among individuals and cultural backgrounds. 13 Similarly, the right kind of social support and motivation to seek social support are influenced by cultural background. 14 Social support provided or received is greatly influenced by the cultural and societal background and values of an individual. 15
Given that stroke is one of the most indispensable social and economic health burdens in Saudi Arabia, 16 great importance has been attached to studies on social support and other factors related to diseases and patients, especially studies addressing post-stroke functional limitations to improve the QOL of stroke survivors.
Aims
This research assessed the QOL and social support of community-dwelling Saudis who survived stroke and examined the effects of several sociodemographic and disease-related variables and social support on QOL.
Methods
A cross-sectional and correlational design was used in Riyadh Province, Saudi Arabia. The STROBE checklist for cross-sectional investigations was followed. The study was performed on two government hospitals that provide various healthcare services, such as emergency, outpatient, inpatient, acute care and home care services. The two acute care facilities provide services to stroke survivors through follow-up check-ups, rehabilitative care and home care services. A purposive sample of 123 Saudi patients who survived stroke were interviewed. Patients who satisfied the following criteria were selected: (1) Saudi national, (2) had been admitted in either of the two hospitals for ischaemic or haemorrhagic stroke in the last 12 months, (3) enrolled in the home care service of the two government hospitals when data collection took place, (4) with moderate functional deficits and (5) provided consent. Non-Saudis and those with severe functional deficits were excluded from the study. The power of the sample size was determined through a post hoc power analysis. With the G*Power, the sample achieved a 0.77 power in detecting small effect size at 0.05 margin of error.
The protocol was approved by the Institutional Review Board of the College of Medicine at King Saud University (research project no. E-19-3733). Informed consent was signed by each patient after a thorough explanation regarding the study, its purpose and importance, the potential risks of participating, expected participation, respondents’ right to refuse participation without any effects on them, services they will receive and their right to terminate their participation. Voluntary participation was emphasised during the recruitment period. The respondents were also told that they have the right to not answer any of the questions. Questions and clarifications about the study were answered accordingly by the researchers. During the interview, privacy and confidentiality were provided by conducting the interviews in a private room. No incentive was provided for participation.
Social support was assessed by the ‘Multidimensional Scale of Perceived Social Support’ (MSPSS). 17 The tool comprised 12 items regarding social support received by the respondents from their family members, friends and relatives, and three subscales with four items each. The MSPSS includes seven-point agree–disagree Likert-type scale items. The mean values were computed for the calculation of subscale scores and overall score. Improved social support is indicated by a high score. The scale has acceptable reliability (Cronbach’s alpha range of the three subscales = 0.85–0.91; Cronbach’s of the entire scale = 0.88; stability reliability = 0.72–0.85). 17 The scale has been utilised in previous research on stroke survivors and their primary caregivers. 18 The Arabic version, which was validated in a previous study, was utilised in the present investigation. 19
The QOL variable was assessed by the World Health Organization QOL-BREF (WHOQOL-BREF). This measure has been utilised in different studies and in measuring people’s perception about situations in life in consideration of cultural and value systems in their environments. This measure considers people’s goals, outlooks, principles and concerns in life. The WHOQOL-BREF is a 26-item scale with five-point Likert-type response options.1–5 It has four dimensions: ‘physical health, psychological health, social relationships and environment domain’. 4 Various studies have used this scale to measure differences in QOL among different cultures. According to the guideline for scoring, raw dimension scores were transformed from 4 to 20. The domain score was recorded by adding the transformed scores. The scores were then transmuted linearly from 0 to 100. A high score denotes excellent QOL. The Arabic version was used in this study. The WHOQOL-BREF has acceptable validity and reliability as evidenced by previous investigations. 20
Questions regarding age, sex, marital status, employment, family income, type of community, family structure, educational level, type of stroke and affected side were inquired.
The researcher trained four research assistants to recruit participants and collect data. The research assistants underwent a series of trainings regarding the study and the processes involved and how to explain the study to respondents, obtain informed consent and conduct interviews. The researcher coordinated with the home care centres of the two government hospitals for participant recruitment and data collection. The research assistants conducted recruitment during home visits to stroke survivors. Patients who gave their consent were subjected to a face-to-face and questionnaire-guided interview. The research assistants read each question twice to a patient before collecting his or her responses. The research assistants were instructed to read the questions as is, and they were not allowed to provide any explanation about each question. The research assistants recorded the responses of the patients in the questionnaires during the interviews, which were performed in private, calm and comfortable places. Recruitment and data collection were performed from June to November 2019.
Data analyses were accomplished through SPSS version 22. For the sociodemographic and disease-related variables, descriptive statistics were computed. Mean and standard deviation (SD) were calculated for social support and QOL. t-test, one-way analysis of variance with Tukey’s honestly significant difference (HSD) post hoc test and Pearson’s product moment correlation were used in testing relationships and sociodemographic, disease-related variables and social support, respectively. Multivariate multiple regression analysis using the Wilks’ lambda test was performed for determining the multivariate effects of the predictor variables (sociodemographic, disease-related variables and social support domains) on the four domains of QOL. The individual effect of the predictors on each QOL domain was examined through multiple regression analyses.
Results
Of the 165 surveys, only 123 were completed and included in the analyses, and thus the response rate was 74.5%. The average age was 75.59 years (SD = 10.90), and age ranged from 60 to 97 years. The interviewed survivors were mostly male (65.9%), married (66.7%), unemployed (74.0%) and living in urban areas (70.7%), belonged to nuclear families (82.9%) and had not attended formal education (56.1%). The highest percentage (38.2%) had a family income of below 10,000 SAR (Saudi Arabian Riyal) per month, whereas the least proportion had 30,000 SAR and above (15.4%). With regard to the disease-related variables, 80 (65.0%) of the respondents had ischaemic stroke, whereas 43 (35.0%) had haemorrhagic stroke. A total of 55 respondents (44.7%) had left-side body weakness, 53 (43.1%) had right-side body weakness and 15 (12.2%) had weakness on both sides (see Table 1).
Demographic and disease-related variables (n = 123).
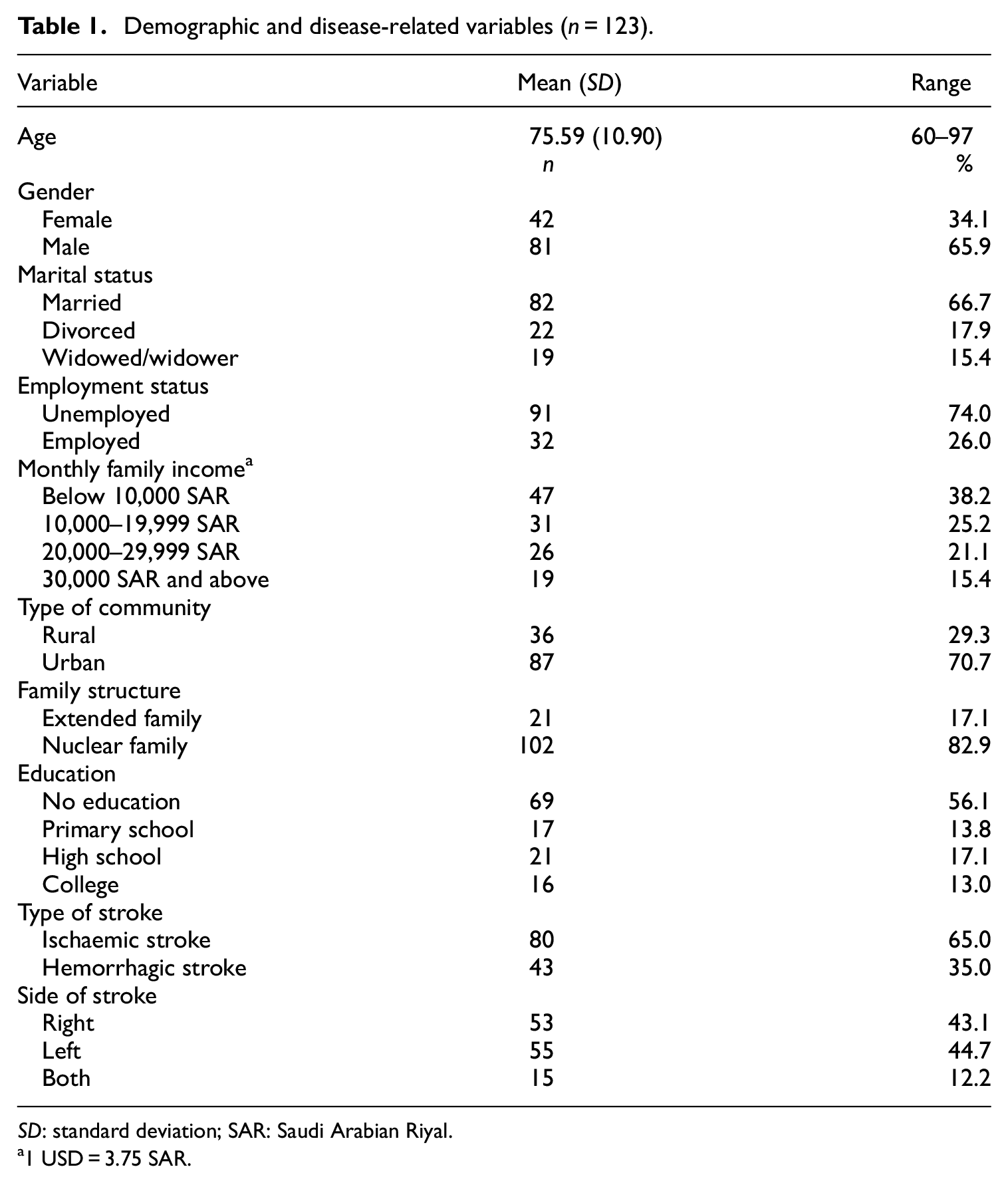
SD: standard deviation; SAR: Saudi Arabian Riyal.
1 USD = 3.75 SAR.
Social support and associated factors
As shown in Table 2, the overall mean in the MSPSS was 4.81 (SD = 0.96). Among the three dimensions of MSPSS, support from family members had the highest average (M = 5.53, SD = 0.88), followed by support from significant others (M = 5.27, SD = 1.26). Support from friends was rated as the lowest by the respondents (M = 3.63, SD = 1.52). The results of the tests for association and differences in perceived social support by demographic and disease-related variables are presented in Table 3. Only family income (F = 2.81, p = .042) and family structure (t = 2.61, p = .015) were significantly associated with the respondents’ perceived social support. Specifically, respondents belonging to families with monthly incomes of 30,000 SAR and above (M = 5.18, SD = 0.88) perceived their social support better than those belonging to families with monthly incomes of 10,000–19,999 SAR (M = 4.44, SD = 0.94, p = .039). Moreover, respondents belonging to extended families (M = 5.41, SD = 1.20) perceived their social support better than those belonging to nuclear families (M = 4.69, SD = 0.85, p = .015).
Descriptive analyses results on the social support and quality of life (n = 123).

SD: standard deviation.
Results of tests of association between and difference on social support and demographic and disease-related variable (n = 123).

SD: standard deviation; SAR: Saudi Arabian Riyal.
Significant at .05 level.
QOL and associated factors
The respondents rated the environmental domain of the WHOQOL-BREF as the highest among the domains, with an overall mean score of 53.23 (SD = 13.25). Social and psychological domains received an overall mean score of 46.68 (SD = 21.94) and 43.19 (SD = 16.82), respectively. Physical domain was perceived as the poorest domain by the respondents, with an overall mean score of 28.57 (SD = 16.08, see Table 2).
Multivariate analysis revealed that age (Λ = 0.90, p = .025), gender (Λ = 0.91, p = .032), employment status (Λ = 0.91, p = .048), monthly family income (Λ = 0.88, p = .007), type of community (Λ = 0.90, p = .028), education (Λ = 0.91, p = .042), type of stroke (Λ = 0.88, p = .009), side of stroke (Λ = 0.80, p < .001) and support from significant others (Λ = 0.87, p = .006) had multivariate influences on the domains of QOL (see Table 4).
Results of the multivariate multiple regression analysis on quality of life dimensions using Wilks’ lambda test (n = 123).

df: degrees of freedom.
Significant at .05 level; **Significant at .01 level; ***Significant at .001 level.
As indicated in Table 5, the four regression models were statistically significant explaining 25.5%, 26.5%, 18.6% and 24.3% of the variance in physical, psychological, social and environmental domains, respectively. Specifically, male respondents reported better physical health (ß = 6.75, p = .026, 95% confidence interval (CI) = 0.81, 12.69) and social relationships (ß = 10.39, p = .017, 95% CI = 1.92, 18.86) than female respondents. Patients who were divorced reported better physical (ß = 9.29, p = .016, 95% CI = 1.78, 16.80) and psychological (ß = 8.83, p = .027, 95% CI = 1.03, 16.63) domains than patients who were married. Widowed/widower had lower social domain scores than married patients (ß = −14.55, p = .029, 95% CI = −27.58, −1.52). Unemployed patients had poorer physical domain scores than employed patients (ß = −14.81, p = .007, 95% CI = −25.39, −4.23). The respondents with family monthly incomes below 10,000 SAR had poorer environmental domain than the patients with higher monthly family incomes. Moreover, patients living in rural areas had better social domain than those from urban areas (ß = −12.46, p = .004, 95% CI = −20.94, −3.97). Patients who received no education had poorer environmental domain compared with those who finished primary school (ß = 7.51, p = .032, 95% CI = 0.67, 14.35) and those who had college degree (ß = 11.06, p = .037, 95% CI = 0.66, 21.47) and had poorer physical domain than college graduates (ß = 18.27, p = .005, 95% CI = 5.74, 30.81).
Results of the multiple regression analyses conducted on each quality of life domain (n = 123).

95% CI: confidence interval; SAR: Saudi Arabian Riyal.
The quality of life domains were the dependent variables. β is the unstandardised coefficients. SE-b is the standard error. Beta is the standardised coefficients.
Significant at 0.05; **Significant at 0.01; ***Significant at 0.001.
Patients who survived haemorrhagic stroke perceived their physical domain better than those who survived an ischaemic stroke (ß = 6.63, p = .041, 95% CI = 0.28, 12.98). Patients with either right-side weakness (ß = 17.16, p = .001, 95% CI = 7.12, 27.21) or left-side weakness (ß = 12.44, p = .014, 95% CI = 2.57, 22.30) reported better psychological domain than those suffering from both. Similarly, patients with weakness on both sides of the body reported poorer physical domain (ß = 15.6, p = .001, 95% CI = 6.14, 25.13) than those with left-sided weakness and poorer environmental domain (ß = 10.84, p = .009, 95% CI = 2.82, 18.87) than those with right-side weakness.
On the influence of social support, good support from significant others was associated with good psychological domain (ß = 4.30, p = .003, 95% CI = 1.53, 7.07), whereas good support from family members was associated with good social (ß = 3.60, p = .011, 95% CI = 0.85, 6.35) and environmental (ß = 1.94, p = .018, 95% CI = 0.34, 3.54) domains.
Discussion
The findings revealed that Saudi stroke survivors perceived their social support in general as moderate with higher perceived support reported from family and relatives than from friends. This scenario seems to be a common experience in patients who had stroke. A previous systematic review on social support post-stroke revealed that a common theme is difficulty in maintaining friends and acquaintances after a stroke attack. Decrease in participation in community activities and interactions with friends were also reported. 21 Difficulty in maintaining good relationship with friends after a stroke attack is associated with decreased physical functioning, decreased cognitive ability, fatigue, change of residence due to rehabilitation care needs, financial difficulties, activity limitations and social stigma. 21 The same systematic review reported that relationships with family and close relatives remain strong and stable post-stroke. Several challenges, such as disruptions in family affairs, changes in familial roles and usual activities and communication problems, often cause problem within families but are often overcome and solved. 21 This situation holds true in Saudi families, which prioritise family cohesiveness during a family member’s illness to maintain a positive image in the society. Saudi family values close family ties, even during illnesses. Family members are highly involved in the care of their family members with illness. Decisions regarding healthcare are often performed within the family level. 22 Furthermore, respect increases as a person ages in the Saudi society. Thus, old people in the family and in the society are given the highest respect. 22 Old Saudi adults prefer to receive care from a family member and receive social support from family than from other sources of support and placing old adults in long-term care facilities is an uncommon practice in the Saudi society and considered a dishonour. 23 Nonetheless, social support has consistently shown positive influence on patients’ overall well-being after stroke.
Survivors belonging to an extended family have better perception of social support than those belonging to a nuclear family. Traditionally, Saudi families are usually extended and comprise a husband, wife, unmarried children, and married children and spouses. 23 This type of family structure creates a strong bond among family members and prioritises caring for old members of the family. 23 Having family members during stroke recovery provides an immediate source of support. Intergenerational support and solidarity within families are extremely common in the Saudi society and reduce isolation in the late stages of life. 24 High monthly family income seems to be more associated with social support than low family monthly income. A similar finding was reported by a previous study, which reported that old adults who do not experience financial constraints perceive their social support more positively than those experiencing financial constraints. 24
The findings suggest that Saudi stroke survivors perceive their QOL poorly, with only environmental domain receiving a mean that is higher than the median of the possible score range. The patients perceived their physical health as the poorest QOL domain. Moreover, psychological health and social relationships were also perceived poorly by the respondents. Similar findings were reported among stroke survivors in South Korea 25 and observed in Saudi Stroke survivors with physical health states that are inferior to those of the general population. 2 The environmental domain of the WHOQOL-BREF encompasses the various facets of QOL, such as financial sources, liberty, feeling safety and security, quality health and social care and home environment. Hence, these factors may have contributed to the better perception of this domain as compared with perceptions of the other domains. The perceived low physical health among the patients is not surprising given that physical challenges are experienced by these patients because of diminished physical functioning and muscle weakness, which cause limited activity. 26 Moreover, stroke impairs cognitive functions, triggering emotional changes and negative feelings. These factors contributed to the low psychological health of the respondents.
Several sociodemographic factors were identified as the predictors of the different domains of QOL. The findings revealed that male patients had better physical health and social relationships than females. An examination of the gender differences on QOL after ischaemic stroke showed that woman had lower QOL than man 3 and 12 months post-stroke. 27 Furthermore, women had greater difficulties in performing everyday activities and had lower chances of recovering from these impairments and gaining independence after an attack. 27 Regarding social relationship, Saudi Arabia is known for strict rules in terms of the mobility of women. Despite the social changes that the country is currently experiencing, women remain to be less socially free. This situation may explain the better social relationships of Saudi men as compared with those of Saudi women. Patients who are employed, have received higher education and have higher monthly family incomes have better QOL than those who are unemployed, receive no education and have lower family incomes, respectively. Previous studies have supported the negative effect of low socioeconomic status on the QOL of stroke patients. 28 Poor socioeconomic status may be a risk to a stroke patient owing to its possible negative effect on health. 29 Poor financial resources may lead to challenges with regard to access to various factors essential to excellent health and well-being, such as quality healthcare, healthy environmental conditions, quality health education and nutritious food.
Haemorrhagic stroke survivors reported better physical health than ischaemic stroke survivors in this study. Several studies have reported a better prognosis and faster functional rehabilitation in haemorrhagic stroke survivors than in ischaemic stroke survivors, although these findings are still inconclusive. A previous investigation found that haemorrhagic stroke patients manifested improved neurological and functional prognosis in contrast to ischaemic stroke patients. 30 Furthermore, haemorrhagic stroke survivors have positive health–related QOL compared with ischaemic stroke survivors. 31 Moreover, haemorrhagic stroke survivors have faster functional ability recovery than ischaemic stroke patients. 32 Bhalla et al. 32 explained that the earlier recovery of functions may be due to the types of cells and tissues in the brain affected by each type of stroke. Bleeding and vasogenic oedema may dislocate tissues inside the white matter, whereas neuronal cells that are affected by ischaemia caused by decreased blood perfusion suffer direct cellular metabolic injury. Tissue functional restoration occurs when haematoma and vasogenic oedema are resolved post-haemorrhagic stroke, accelerating functional recovery in these patients. 32 The findings also support the differences in certain QOL domains based on the part affected by the stroke. Specifically, the study showed that QOL is poorer when both sides of the body are affected than when only either the right or left side of the body is affected. Most of the previous related studies comparing differences in QOL based on which part is affected by stroke compared only the left versus right sides. For example, a study found stroke as a strong predictor of the emotional health of stroke patients undergoing inpatient rehabilitation; furthermore, patients with right-sided stroke have poorer emotional health than left-sided stroke survivors. 33 Similarly, having a right hemisphere stroke is a predictor of poor QOL in stroke survivors from Thailand. 8 In Saudi Arabia, results are contrasting. Stroke survivors with bilateral hemiparesis exhibited more positive functional recovery post-stroke than those having right- or left-sided hemiparesis. 34 Hence, investigations comparing the QOL of unilateral and bilateral stroke are needed.
Social support was found to positively influence the QOL of old Saudi adult stroke survivors. The findings revealed that receiving social support from relatives may improve psychological health. Support coming from family was found to be a predictor of improved social relationships and environmental domain. These findings corroborate previous findings reported in a systematic review, which stated that social support positively influences health-related QOL. 11 Emotional help received as a form of social support enables stroke survivors to achieve high levels of QOL in all four domains, whereas functional support is linked to the improved psychological and social facets of QOL. 35 The present findings imply that old Saudi adults suffering from stroke value their families and relatives in their recovery from the disease, Saudi families give importance to their old family members suffering from chronic diseases and family members contribute to recovery. Although how social support specifically affects the QOL of stroke survivors is still not fully understood, some possible explanation can be offered regarding the present findings. Social support may provide behavioural influences, such as providing motivation by family and significant others on health-promoting activities and compliance to prescribed therapy. This situation can lead to health behavioural changes. Social support may also provide psychological influences, that is, significant others can be a source of positivity and provide assistance to coping, thereby preventing negative emotions among stroke survivors. 11 Another possible explanation is the stress-buffering model. Indirectly, various types of social support from family, friends and relatives may serve as a buffer to facilitate the patient’s adaptation from stress, thereby decreasing the risk of developing complications and facilitating speedy recovery during the rehabilitative stage. 11
Limitations of the study
The study’s design was cross-sectional, and thus causal relationships between variables were not established. The disease-related data were limited only to the type of stroke and the side affected by stroke. Other information related to the disease – such as duration of the disease, time from the attack and functional outcomes – was not considered in this investigation. The study was only performed in two hospitals situated in the same geographical location in Saudi Arabia (Riyadh Province). This situation limits the generalisability of the findings; hence, future studies should consider including other hospitals from the different regions of the country. Another limitation was the low sample size due to the limited number of stroke survivors in the research settings. Hence, future studies must consider surveying larger sample to improve the statistical power of the study.
Conclusion
The study provided evidence of the influence of social support on the QOL of stroke survivors in Saudi Arabia. The study is a valuable addition to existing literature regarding the well-being and health of stroke survivors, adding critical knowledge on how old adults recovering from a stroke attack perceive their QOL and support from family, relatives and friends. The findings of the study provide several implications to the medical field in general. The results can guide the planning of care for stroke survivors in Saudi Arabia and other Arab nations given the cultural and societal similarities. Interventions for enhancing their physical, psychological and social health must be implemented and must be culturally appropriate. Social support, especially from family members and relatives, must be advocated in order that the highest level of QOL is ensured. Social participation among these patients must be encouraged. Community- and hospital-based activities aimed at improving stroke survivors’ physical activities and social interactions can be developed and executed.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of the College of Medicine at King Saud University (approval no. E-19-3733).
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.