
Abstract
Immunotherapies are rapidly growing and changing cancer care. Immune Checkpoint Inhibitors (ICIs) have the ability to block inhibitory checkpoints and restore the functions of the immune system. ICIs are used for the treatment of several types of cancer, and nowadays, many studies are ongoing in order to get approvals for newer indications. ICIs are known to induce immune-related adverse effects. The safety of ICIs and the most common immune-related adverse events are not yet well recognized for our population since this class of medications is lately introduced in our region, where only limited studies in our population are available in the literature. This research is intended to shed light on ICIs and describe our safety experience with these agents. This study is a retrospective cohort study aimed to determine the safety of ICIs and its related adverse events at a tertiary hospital in Saudi Arabia. The study was conducted in the oncology center at King Abdulaziz Medical City, Riyadh. Study participants were identified by using the electronic health care system (BestCare)® to include patients who were treated with ICIs during the study period from January 2016 up to December 2018. A total of 53 patients were included. Most of our patients were on nivolumab (37 patients) followed by atezolizumab (10 patients), and pembrolizumab (6 patients). The average number of emergency room visits after receiving ICIs was three visits per patient. Renal adverse events occurred following ICIs use in nine patients, and none of the reported cases experienced a grade ≥3 event. Moreover, 13 patients experienced a hepatic adverse event, of whom only 1 patient experienced a grade ≥3 event leading to treatment discontinuation. As for diarrhea, among all patients who received ICIs, 14 patients experienced diarrhea, and 5 of them had grade ≥3 events. Also, thyroxine abnormalities occurred in seven patients. While, pneumonitis occurred in four patients following ICIs use. In addition, we noticed other adverse events with ICIs, including (skin reaction, nausea, vomiting, thrombocytopenia, neutropenia, and neurological adverse events). Furthermore, 17 patients required steroids to manage ICIs adverse events. And, no patients in our study required additional management with other immunosuppressive agents. Patients treated with immune checkpoint inhibitors could have a variety of adverse drug events that might lead to treatment discontinuation and increase overall emergency room visits. This study highlights the most common adverse drug events associated with ICIs use at a tertiary care center in Saudi Arabia.
Immune Checkpoint Inhibitors (ICIs) are used to treat cancer by targeting immune checkpoints, which are an important regulator of the immune system that cancer cells use to protect from attacks by the immune system. 1 ICIs have the ability to block inhibitory checkpoints and restore the functions of the immune system. 1 The first ICI was ipilimumab, which is a cytotoxic T-lymphocyte-associated protein 4 (CTLA4) blocker approved in the United States in 2011. 2 This was followed by the anti-programed cell death protein-1 antibodies nivolumab and pembrolizumab. Furthermore, newer ICIs entered the market in the last 3 years and work by inhibiting programed cell death ligand-1, like atezolizumab, avelumab, and durvalumab. 3
ICIs are used for the treatment of several types of cancer, and nowadays, many studies are ongoing to get approval for newer indications. 4 Examples of indications we can use these agents for are melanoma, lung cancer, renal cell carcinoma, and urothelial carcinoma. Based on data, these agents have shown to improve the overall survival and prognosis. 3 ICIs are known to induce immune-related adverse effects, which are defined in the literature as any toxicity with a potential immune-mediated cause and has been associated with many adverse events leading to emergency room visits. 4
In recent years, there have been retrospective studies that showed high rates of adverse effects for patients receiving ICIs. 5 A recent retrospective cohort study at MD Anderson Cancer Center reported a high incidence of adverse effects in patients receiving ICIs. 5 They identified (25%) of patients who had adverse effects that were related to one or more immune-related Adverse Effects (irAEs). Diarrhea was the most common irAEs leading to an increased rate of ER visits. 5 The proportions of ER visits associated with diarrhea, hypophysitis, pancreatitis, thyroiditis or hepatitis varied significantly by which ICIs are used. 5 Colitis was associated with better prognosis, whereas pneumonitis was significantly associated with worse survival. 5 Another retrospective cohort study conducted at a single-center experience in the United Kingdom to evaluate the incidence of adverse effects with pembrolizumab toxicities in melanoma patients and found that the most common adverse effects were skin-related and gastrointestinal-related events. 6 Overall, 25% of patients required oral steroids to manage these adverse effects. 6
Furthermore, another study assessed the incidence of colitis and diarrhea with ICIs, found a high incidence of diarrhea and was recorded in (36%) of patients, and (24%) of them required immunosuppressive treatment. 7
Also, another retrospective study published recently evaluated the effectiveness and safety of ICIs using (ipilimumab, nivolumab, and pembrolizumab). 8 Fifty patients were included, the most common adverse events in this study were fatigue (42%), rashes (22%), nausea (20%), and fever (20%). Moreover, one patient developed severe deep venous thrombosis and tissue inflammation, which were not confirmed in previous clinical trials. 8
The safety of ICIs and irAEs are not yet well recognized for our population since this class of immunotherapy is recently introduced in our region, where only limited studies in our population are available. Besides, real-world safety studies are crucial since they can complement data from RCTs to fill current gaps in clinical knowledge. 9 Moreover, regulatory bodies started to recognize the importance of real-world data to support the assessment of marketed medications, monitor their safety, and help in decision-making. 9 This research is intended to shed light on ICIs most frequent adverse drug events. Also, to differentiate the adverse events among specific ICIs.
Methods
This is a retrospective cohort study conducted at a tertiary single center. The study involved adult patients who were treated in the oncology center at King Abdulaziz Medical City, Riyadh (KAMC). Study participants were identified by using the electronic health care system (BestCare)® to include all patients who were treated with ICIs during the study period from January 2016 up to December 2018. Inclusion criteria: patients with an age of 18 years or older and received ICIs therapy (including nivolumab, pembrolizumab, and atezolizumab). Exclusion criteria: Patients with an age of less than 18 years old or patients with missing physician notes or follow up after receiving the treatment.
Adult patients treated with ICIs in KAMC, who met the above-specified criteria were included. The following patient demographic and clinical data were collected: gender, age, weight, height, comorbidities, treatments rendered, and subsequent emergency room visits including the visits related to immune-related, date and dose of ICIs, laboratory data, data about irAEs in the literature search were collected from the patients’ records concentrating on visit notes and also all records.
Sample size calculations
One of the main objectives of the current study was to estimate the prevalence of immune-related adverse events with ICIs in our intuition. A previous systematic review has estimated the prevalence of immune-related adverse events with ICIs in 5744 patients with non-small cell lung cancer, from 23 studies treated with anti-PD-1 or anti-PD-L1 to be 64%. 10 For the purpose of our study, we assumed that the prevalence of immune-related adverse events was approximately 65%. Assuming the desired precision level of 5% and a confidence interval of 95%, the current study required the enrollment of 78 patients to achieve this target. However, this target could not be reached due to the limited accessibility of data from other hospitals, and we based our sample from all patients who received ICIs in our institution. Furthermore, we established our total population for patients who received ICIs based on nivolumab utilization data in the kingdom, which are around 100 patients in Saudi Arabia during the defined period. We used convenience sampling to identify the study participants from single-center, and we included all patients who received treatment with ICIs during the defined period in our center.
Statistical analysis
Descriptive statistical analyses were completed for the study participants. Continuous variables were summarized using mean ± SD, median, and range. Proportions used for categorical variables. ICIs were compared in terms of baseline demographic and clinical characteristics, as well as the incidence of adverse events and emergency room visits. Comparisons were made using a one-way ANOVA or Kruskal-Wallis test for continuous variables and the chi-square test for categorical variables. Statistical significance will be considered at p-value <0.05. All statistical analyses performed using SPSS 21.0 [Release 21.0.0.0, IBM, USA].
Raw data were processed per the finest practice for raw data management to identify any inaccuracies in advance to the statistical analysis. To achieve this task, all interval variables were checked and summarized in terms of minimum and maximum values and were compared against the possible minimum and maximum values; implausible values were flagged. A similar process was applied to categorical variables to identify any potential anomalies. All identified anomalies discussed with the biostatistician and corrected before statistical analysis. The original data were collected and safely stored in the principal investigator’s office. Data entered and saved in an appropriately designed Excel sheet.
Results
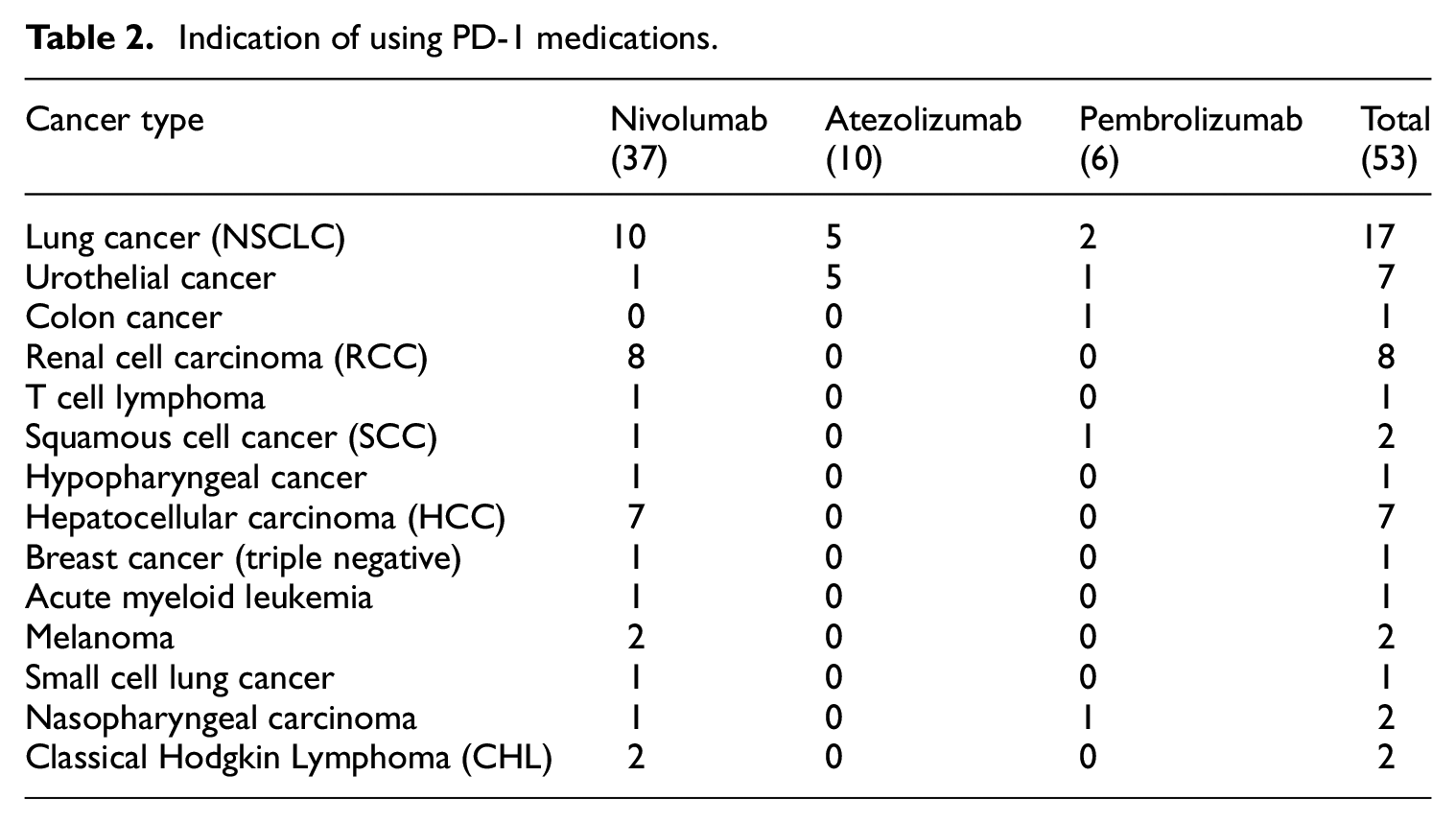
A total of 60 patients who received ICIs during the study period were screened for inclusion. A total of 53 met the specified inclusion criteria for our study. Descriptive data of the baseline and demographic of the patients are presented in Table 1. The number of patients in each treatment group was as follows: nivolumab 37 (70%), atezolizumab 10 (19%), and pembrolizumab 6 (11%). The average age was 59 years, with 70% males. Indications for treatment were documented to be Non-Small Cell Lung Cancer (NSCLC) 32%, Renal Cell Carcinoma (RCC) 15%, urothelial cancer 13%, Hepatocellular carcinoma (HCC) 13%, melanoma 3.7%, Classic Hodgkin lymphoma (CHL) 3.7%, nasopharyngeal cancer 3.7%, squamous cell cancer 3.7%, and 11% had other tumors. Underlying conditions of the patients were: hypertension 32%, 21% diabetes, 9% dyslipidemia, and 6% chronic kidney disease. Around 87% of the patients used analgesics medications. The average PD-1 cycles were nine cycles. Seventeen patients had (NSCLC); most of them treated with nivolumab. Table 2 shows an indication of using PD-1 medications. Table 3 shows prescribing patterns for ICIs (nivolumab, atezolizumab, pembrolizumab) dose and frequency. Descriptive statistics for adverse events are also provided in Table 4.
Profile of patients—baseline characteristics.

N = 53.
Other: Acute myeloid leukemia, hypopharyngeal cancer, small cell lung cancer, T cell lymphoma, breast cancer (triple-negative), colon cancer.
Indication of using PD-1 medications.
Prescribing patterns.

Safety of immunotherapies.
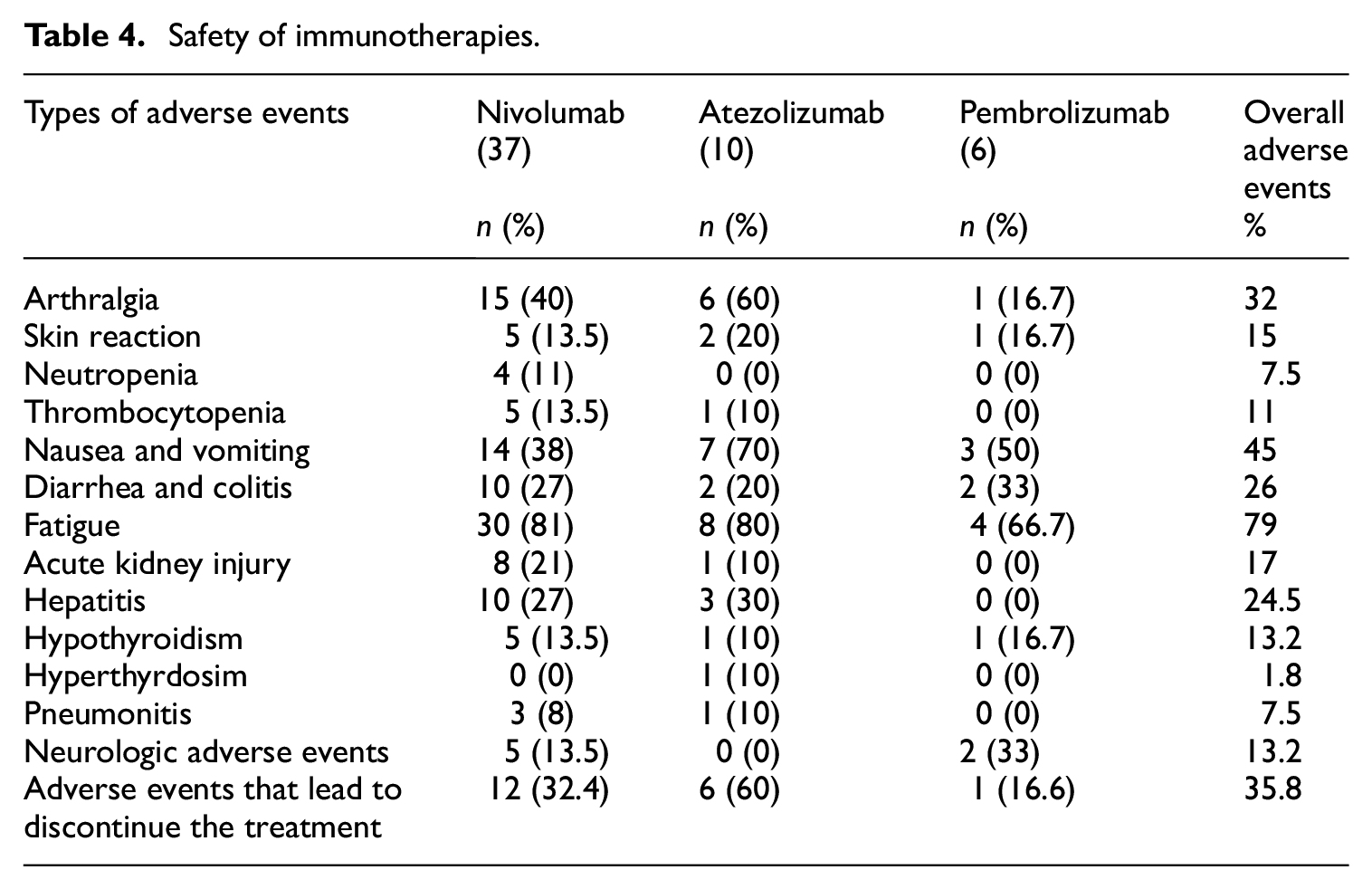
Safety of immunotherapies: Adverse events (as shown in Table 4)
Renal adverse events (acute kidney injury)
A total of 53 patients had normal baseline serum creatinine values. Following the drug use, nine patients (17%) (eight used nivolumab, one used atezolizumab) experienced an increase in serum creatinine with a moderate event, and none of the cases experienced a grade ≥3 event (severe or life-threatening event).
Hepatic adverse events (hepatitis)
The baseline LFT test values for a total of 53 patients were normal. After taking medications, nine patients (24%) (used nivolumab) experienced a grade 1–2 adverse event (mild event), only one patient experienced a grade ≥3 event that led to discontinuation of treatment and three patients (30%) (used atezolizumab) experienced a grade 1–2 adverse event.
Diarrhea and colitis
Among all patients who received the treatment, 10 (27%) (used nivolumab) experienced diarrhea, and 4 of them experienced a grade ≥3 event that led to discontinuation of treatment. While 2 (20%) (used atezolizumab) had a grade 1–2 diarrhea. Besides, two patients (33%) experienced diarrhea with Pembrolizumab; one of them had a grade ≥3 event.
Hypothyroidism and hyperthyrdosim
A total of five patients (13.5%) had thyroxine abnormalities that occurred after the use of nivolumab; also hypothyroidism occurred in one patient who used atezolizumab and one used pembrolizumab. There is only one case of a patient who had hyperthyrdosim with atezolizumab.
Fatigue and arthralgia
Many patients experienced these devastating adverse events. About 41% of patients who received immune therapies experienced arthralgia. While 79% of patients experienced general fatigue. Only one patient had severe fatigue with a grade ≥3 event that could not be tolerable and led to treatment discontinuation with atezolizumab.
Pneumonitis
Pneumonitis occurred in (7.5%) of patients who received ICIs. Three cases occurred with nivolumab and one case with atezolizumab. The only case with atezolizumab occurred after receiving four cycles of treatment, and the patient had pneumonitis that led to death. The first case with nivolumab occurred after receiving 33 cycles of treatment, pneumonitis was managed with antibiotics and steroids, and the patient recovered, but the treatment was held. The other two cases were suspected pneumonitis after three and two cycles of nivolumab; the patients died during an inpatient setting.
Skin reaction
The (15%) of patients who received PD-1 drugs had a skin reaction. Only one patient who received atezolizumab had a grade ≥3 event skin reaction that led to discontinuing the treatment by a dermatology consultant.
Other adverse events
Table 4 shows the other adverse events reported, like (thrombocytopenia, neutropenia, nausea, vomiting, and neurological adverse events). All the other adverse events reported in the table had grade 1–2 adverse events and did not lead to treatment discontinuation.
Adverse events that led to treatment discontinuation
As shown in Table 4, 12 (32%) patients who received nivolumab had adverse events that led to discontinuing the treatment. The following cases required discontinuation with nivolumab use: three pneumonitis cases, two AKI cases, two neurological symptoms cases, one autoimmune hepatitis case, one diarrhea case, and two cases where patients preferred to discontinue the treatment due to general intolerability.
Also, out of 10 patients who received atezolizumab, 4 patients had adverse events that led to discontinuation of treatment (first case: skin reaction, second case: increased liver function tests, third case: general fatigue and fourth case: pneumonitis). Moreover, two patients died after two cycles of atezolizumab with cardiac arrest, one at home, and the other case in the Emergency Room (ER). In comparison, one out of six patients who received pembrolizumab discontinued treatment due to the occurrence of colitis with grade ≥3 event.
Management of related adverse events
Of the 53 patients, 17 patients required steroids to manage (irAEs) (nivolumab, n = 15 [40%], atezolizumab n = 1 [10%], and pembrolizumab, n = 1 [16.6%]). Seventeen patients received steroids; eleven of them received oral steroids in the management of adverse events. In our study, no patients required further management with other immunosuppressive agents.
ER visits
The numbers and percentages of cancer patients presenting to the ER with various related adverse effects after beginning immune checkpoint therapy were tabulated for each immune checkpoint therapy alone in Table 5 with ER visits and the total length of stay (LOS). There were no statistically significant differences between the three treatment groups in terms of ER visits (p > 0.05).
ER Visits after beginning immune checkpoint therapy.

Patients who developed infections during treatment
A total of 33 (62.2%) patients had infections during immune checkpoint therapies. The most common type of infection was upper respiratory tract infection (35.5%) followed by urinary tract infection (20%), pneumonia (20%), and bacteremia (13.5%). For patients who had positive cultures, bacterial infection (62%) was the most common organism, followed by fungal infection (23.8%) and viral infection (14.2%).
Discussion
To the best of our knowledge, this is the first comprehensive study to assess real-world safety and tolerability of ICIs in the Middle East. ICIs are known to induce immune-related adverse effects. 4 A broad range of irAEs associated with ICIs can complicate the efficacy of immunotherapy and limit its use in cancer patients. 11 The specific pathophysiology underlying these types of adverse events is unknown, however it may be related to breaching the balance of immunologic homeostasis. 11 Immune-related adverse effects could involve any organ, most frequently involve the gastrointestinal tract, skin, and endocrine glands. 11 Most irAEs that occur during the ICIs are mild and manageable if the patients receive proper management with close monitoring; however, there are some cases that are reported with severe and life-threatening toxicities like myocarditis and pneumonitis.11,12 The reported adverse effects with ICIs include thyroxine abnormalities, fatigue, pneumonitis, hepatitis, colitis, etc. 13 The results from this chart review study report that thyroxine abnormalities occurred in five patients (13.5%) after using nivolumab; Moreover, hypothyroidism occurred in one patient (10%) who used atezolizumab and one used pembrolizumab. There is only one case of a patient who had hyperthyrdosim with atezolizumab. In a recent meta-analysis, the incidence of hypothyroidism in patients receiving ICIs was 6.6%. 14 While hyperthyroidism was reported in another meta-analysis with an incidence of 2.9% with ICIs use. 14
AKI following ICIs use occurred in nine patients (17%) (of whom eight used nivolumab, one used atezolizumab) where they experienced an increase in serum creatinine (moderate event), and none of the cases experienced a grade ≥3 event (severe or life-threatening event). Based on the current literature, in a recent meta-analysis that assessed AKI with PD-1 inhibitors, the incidence of all AKIs was 2.2%, of which 19% were of grade 3–4, and no cases of deaths occurred. 15
Hepatitis occurred in nine patients (24%) (used nivolumab) who experienced a grade 1–2 adverse event (mild event), only one patient experienced a grade ≥3 event that led to discontinuation of treatment and three patients (30%) (used atezolizumab) experienced a grade 1–2 adverse event. In a recent meta-analysis, the incidence of all-grade treatment-associated hepatic injury varied from 14 to 42% although the incidence of high grade ranged from 1% to 11%. 16
One of the most frequent irAEs is gastrointestinal disorders. 12 In our study, colitis occurred to some patients who received the treatment, where 10 (27%) (used nivolumab) experienced diarrhea. While 2 (20%) (used atezolizumab) had a grade 1–2 diarrhea. Besides, two patients (33%) experienced diarrhea with pembrolizumab. Based on the current literature, the incidence of colitis in general ranges from 1% to 25% depending on the type of ICIs and if used alone or in combination where the incidence increased. In addition, the incidence of colitis is higher in patients receiving anti-CTLA-4 agents, such as ipilimumab, compared to patients receiving anti-PD-1/PD-L1 agents, such as nivolumab, pembrolizumab or atezolizumab that were used in our study. 17
Furthermore, many patients experienced fatigue and arthralgia, which are devastating. Around 41% of patients who received ICIs experienced arthralgia. While 79% of patients experienced general fatigue. Only one patient had a grade ≥3 event (severe fatigue) that could not be tolerated and led to discontinuing the treatment with atezolizumab. In our study, the rate of fatigue seemed to be higher compared to the reported rates of fatigue in previous studies are around 32%. 13 Pneumonitis induced by ICIs are uncommon adverse events. However, the toxicity can be severe and lead to death. 12 Pneumonitis occurred in (7.5%) of our patients. In a meta-analysis, 2.7% of patients receiving anti-PD-1/PD-L1 agents as monotherapy developed pneumonitis for all-grade and 0.8% for grade 3 or higher. 18 The skin reaction is one of the common adverse effects seen with ICIs. 19 Pruritus and rash are among the top immune-related adverse events reported in clinical trials. 19 The incidence of skin reactions reported between 30% and 40%. 19 Only 2% of skin reactions reported as grade 3 or 4 events. 19 Skin reactions occurred in (15%) of our patients who received ICIs. Only one patient who received atezolizumab had a grade ≥3 event skin reaction that led to discontinue the treatment.
The majority of patients had ER visits, and some of them were admitted due to toxicities with these agents. Of the 53 patients, 17 patients required steroids to manage the adverse effects of immunotherapy. Although, out of those 17 patients who received steroids, 11 patients received oral steroids in the management of adverse events.
Several studies and case reports have raised concerns that ICIs are associated with increased risk of infections.20,21 Also, using immunosuppression to treat immune-related adverse events could increase susceptibility to infection. 22 In this study, 33 (62.2%) patients had infections following ICIs use. We found that the most common type of infection was upper respiratory tract infection (35.5%) followed by urinary tract infection (20%), pneumonia (20%), and bacteremia (13.5%). For patients who had positive cultures, bacterial infections (62%) were the most common organism followed by fungal infections (23.8%) then viral infections (14.2%).
There are several strengths to this study. There is a lack of data on the most frequent immune-related adverse events following the use of ICIs in the region as they are not yet well established for our population. This study helps to fill the gaps in current evidence by using real-world chart review data outside a controlled trial setting to describe our experience in our population and provides detailed clinical information and insights to health care providers. However, several limitations need to be identified. The design of the study is a retrospective medical chart review where the results are limited by the completeness of the information that was recorded in those charts. In addition to the small sample size and further investigations with larger sample size are needed to confirm our findings as additional novel immunotherapy is added.
Conclusion
Patients treated with ICIs may have a spectrum of adverse drug events that might lead to discontinue the treatment and increase ER visits. This study highlights the most common adverse drug events with ICIs use at a tertiary care center in Saudi Arabia.
Footnotes
Acknowledgements
Acknowledgment to King Abdullah International Medical Research Center (KAIMRC) and Medication Safety Research Chair.
Author’s Note
Mohammed Al Nuhait is currently affiliated with College of Pharmacy, Umm Al-Qura University, Makkah, Kingdom of Saudi Arabia
Author contributions
MN, EB, AS, AO, and YA have written the paper; YA has supervised the research; MN and EB have analyzed and interpreted the data; MN has worked on data collection and coordinated the study. Each author listed on the manuscript has seen and approved the submission of the present version of the manuscript and takes full responsibility for the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC), National Guard Health Affairs, Riyadh, Saudi Arabia, in December 2018. The informed consent was waived due to minimal risk associated with design of retrospective studies.
Availability of data and material
The data used to support the findings of this study are restricted by the KAIMRC in order to protect patient privacy. Data are available from KAIMRC for researchers who meet the criteria for access to confidential data.