
Abstract
Objectives:
During the height of the COVID-19 pandemic, vaccine hesitancy in the United States was a key driver of continued COVID-19 transmission and the emergence of new variants. We examined the effect of a mandate that required patrons at nonessential venues (eg, restaurants, bars) in New Orleans, Louisiana, to be vaccinated to enter these establishments from August 2021 through March 2022.
Methods:
We implemented a parish-level synthetic control model that compared vaccination trends in Orleans Parish (county) (the boundaries of Orleans Parish are equivalent to the city of New Orleans) with a synthetic composite of other parishes in Louisiana that had similar vaccination trends before the mandate. We used permutation testing (ie, shuffle testing) to determine the significance of differences in vaccination rates between Orleans Parish and other parishes.
Results:
Individuals in Orleans Parish initiated an average of 760 more vaccines weekly during the 31 weeks in which the mandate was in place, which was significantly higher than expected based on the synthetic control (P = .03).
Conclusions:
The rate of vaccine initiation increased during the vaccine mandate for nonessential venues. Implementing such mandates may be an effective intervention in overcoming COVID-19 vaccine hesitancy during a future pandemic.
The rapid creation, authorization, and distribution of vaccines during the COVID-19 pandemic has been important for the prevention of morbidity and mortality. Vaccination against COVID-19 in the first year of rollout is estimated to have averted 14.4 million deaths globally and 1.1 million deaths in the United States in 2021.1,2 However, as of May 2023, vaccine hesitancy was a substantial concern in the United States, where roughly one-fifth of the population had yet to receive a single COVID-19 vaccine dose. 3 As the United States moved from nonpharmaceutical interventions, such as face masks and physical distancing, the need for an increase in vaccine uptake became even more important for the protection of health care capacity and the prevention of morbidity and mortality among people in the United States.
Vaccine hesitancy can be understood through the model of complacency, confidence, and convenience.4,5 Complacency refers to the lack of perceived importance of vaccination, where individuals do not feel that there is a particular risk to themselves if they remain unvaccinated. Complacency can be overcome by appealing to individuals’ desires to protect their families or communities or by offering them incentives to get vaccinated.6-8 Confidence refers to the trust that people have in the medical system and the vaccines that are being offered to them. Historic medical mistrust was a key driver of lower vaccination rates among Black, Indigenous, and Hispanic people, as in the past unethical experiments were conducted among these groups.9,10 In addition, misinformation and disinformation undermine confidence in vaccines, where people are told that the vaccines are unsafe or that statistics are grossly distorted to call into question safety and/or efficacy claims made by health officials.11,12 Several approaches can be used to overcome a lack of confidence, including community engagement, having those who are vaccinated explain their decision to those who are not vaccinated, considering anxieties and emotions in discussions of vaccine hesitancy, and the labeling of misinformation and disinformation clearly in online resources.13-16 The final pillar of this model, convenience, refers to barriers and facilitators to the act of getting a vaccine. Barriers include the cost of transportation, the need for time off work, the need for computer literacy to book an appointment, and the challenge of competing interests such as childcare. Hence, overcoming issues of convenience would require structural approaches, such as ride-share rebates for vaccine appointments, multiple options for booking vaccine appointments, community vaccine pop-up sites, and childcare options.9,16
One strategy that has been used to overcome complacency is the mandating of vaccines for nonessential indoor venues, generally defined as venues providing services that are not essential to health care, human services, the sale of groceries and food, logistics, transportation, and infrastructure. Such venues include restaurants, bars, gyms, and sports or concert arenas. These mandates promote vaccine uptake but inconvenience those who choose to remain unvaccinated but wish to frequent these spaces. New Orleans, Louisiana, used such a strategy, implementing a vaccine mandate to access restaurants, bars, gyms, and other high-occupancy, nonessential public venues. To be able to attend these venues, the city mandated either 1 COVID-19 vaccine dose or a negative polymerase chain reaction test within 72 hours on August 16, 2021. 17 To be compliant, prior to entering these establishments individuals had to show digital or physical proof of their vaccination (eg, Centers for Disease Control and Prevention COVID-19 vaccine card, state-issued vaccine confirmation) or a negative test result to venue staff. This mandate was then removed on March 21, 2022. 18 We used a synthetic control model to compare the rate of vaccine uptake in New Orleans after implementation of this mandate with a control based on weighted data from other Louisiana parishes (counties). We hypothesized that compared with residents in the control parishes, residents in Orleans Parish would have a significantly higher rate of vaccination.
Methods
We used publicly available datasets from the Louisiana Department of Health that contained daily vaccination counts from each parish. The Tulane University Institutional Review Board determined that this research was exempt from institutional review board oversight because of the use of deidentified data. We used data on first doses and limited the date range from the onset of the COVID-19 vaccination program, December 14, 2020, through March 21, 2022, when the mandate was lifted. We obtained parish-level demographic data for 2021 from the American Community Survey. 19 Given that the boundaries of the city of New Orleans and Orleans Parish are coterminous, we considered Orleans Parish data to be equivalent to New Orleans city data.
We used a synthetic control model to determine the effectiveness of COVID-19 vaccine mandates in Orleans Parish in increasing the rates of vaccine initiation. We used the remaining 63 parishes in Louisiana, where no mandates were in place, to create a synthetic control, to estimate the effect of mandates on vaccine uptake. Using covariates measured prior to implementation of the mandates to generate weights for the extent to which each control parish contributed to the synthetic control, we investigated multiple sets of covariates to determine which set yielded as close a control to the actual vaccine rates of Orleans Parish, before implementation of the mandate. We tested the following covariates based on availability in the American Community Survey 18 : racial distribution, age distribution, educational attainment, income information, housing information, rurality, and sex distribution. We ultimately selected the following factors: the percentage of vacant houses, the percentage of urban areas in the parish, the median annual household income of the parish, and the percentage of individuals living at or below the federal poverty level. These covariates achieved the best match between vaccination rates in Orleans Parish and the synthetic control as compared with the preintervention period (ie, the smallest root mean squared predicted error [RMSPE] was observed preintervention between Orleans Parish and the control parishes). We then compared vaccination rates between Orleans Parish and the synthetic control parish. We conducted all analyses in Stata version 15 (StataCorp LLC) using the “synth” package by Hainmueller et al. 20 We calculated the number of excess vaccinations by determining the difference between the control and the actual vaccination rates during the postintervention period. When minimizing the differences between Orleans parish and the control parish, the model selected the following parishes for inclusion in the synthetic control: East Baton Rouge, East Carroll, and Pointe Coupe. The remaining parishes were weighted at zero, per the model, as this selection of parishes was determined to produce the best comparable control population.
We conducted permutation testing (ie, shuffle testing) to evaluate the significance of the model. 21 To do so, we generated a synthetic control for each parish in Louisiana and computed the difference in vaccine initiation between the actual parish and its synthetic control. We then ranked parishes by the ratio of the posttreatment period to the pretreatment period RMSPE. We defined 2-tailed significance as (2 × rank) divided by the number of parishes, in which “rank” was the rank order of the ratio of post-RMSPE to pre-RMSPE in the treated parish. For example, if Orleans Parish had the highest computed gap in a sample of 64 parishes, it was significant at the (2 × 1)/64, or the 3% significance level.
Results
When comparing Orleans Parish and the synthetic control parish, Orleans Parish had fewer vacant properties (14.8% vs 18.9%), was more urban (99.5% vs 54.5%), had a lower median annual household income ($45 594 vs $49 987), had slightly more people living in poverty (23.8% vs 21.0%), and had a higher vaccination rate before the mandate (65.5% vs 55.2%).
Before implementation of the vaccine mandate on August 16, 2021, 243 503 people had initiated COVID-19 vaccination (65.5% of the population vs 55.2% of the synthetic control parish). During the period in which the mandate was in place, 52 720 people initiated a COVID-19 vaccine (14.0% of the population vs 10.6% in the synthetic control).
In Orleans Parish, vaccine initiation was sustained throughout most of the mandate period, although the rate of new vaccinations declined around February 2022 (Figure 1). In this model, Orleans Parish saw an average of 760 more vaccinations initiated in the mandate period compared with the synthetic control parish. This increase corresponded to 0.7% more unvaccinated people initiating vaccination in Orleans Parish compared with people in other parishes. During the 31 weeks in which the vaccine mandate was in place, 23 560 more people initiated vaccination than would have been expected in the absence of a vaccine mandate. The ratio of the posttreatment period to the pretreatment period RMSPE between Orleans Parish and the synthetic Orleans Parish was the largest among parishes contributing to the synthetic control (Orleans: 0.90; Pointe Coupe: 0.36; East Carroll: 0.46; East Baton Rouge: 0.47) (all significant at P = .03) (Figure 2).
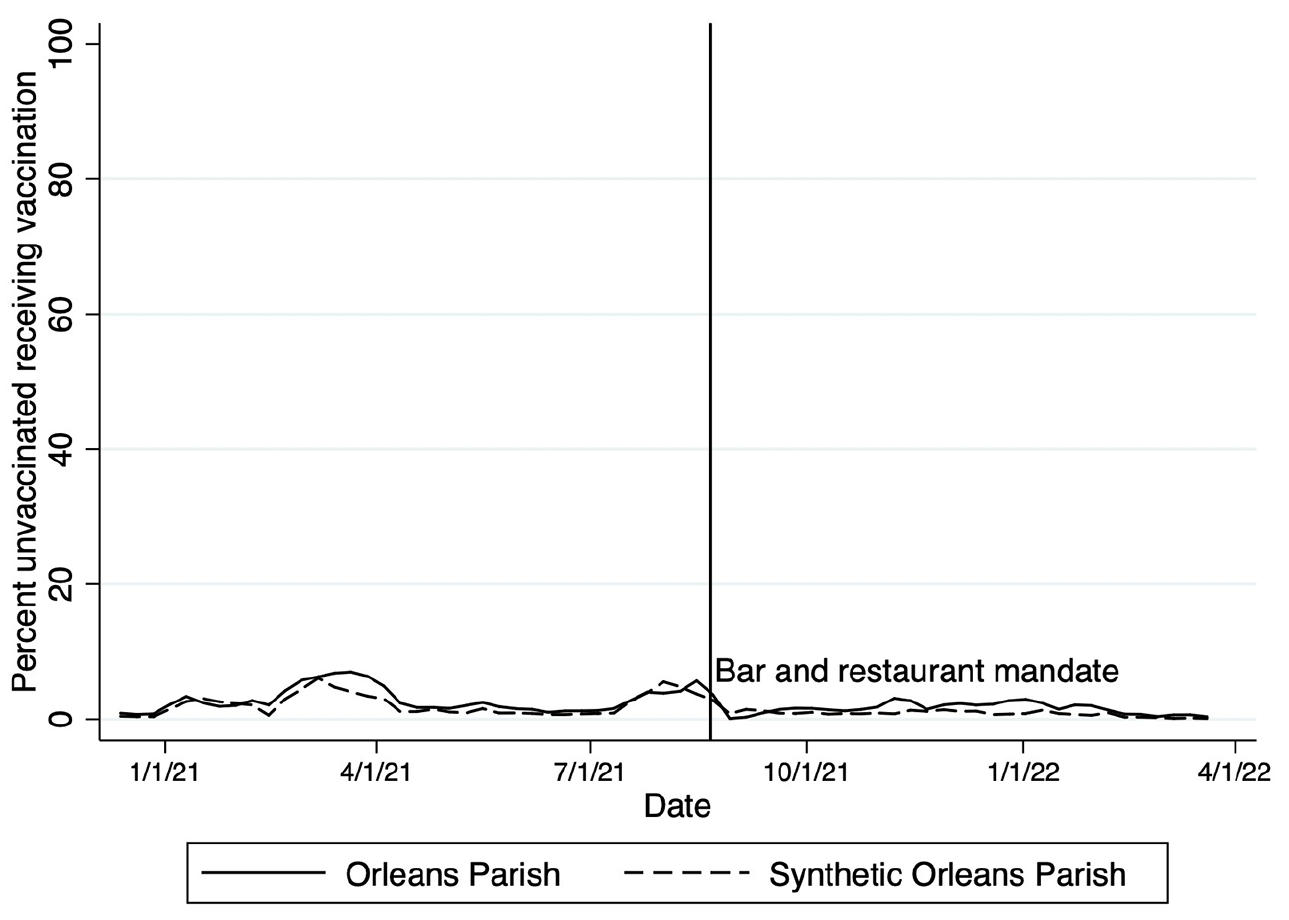
Vaccination rates in Orleans Parish compared with a synthetic control parish before and during a COVID-19 vaccine mandate to enter nonessential venues (eg, bars, restaurants) in New Orleans, Louisiana, 2021-2022. The figure compares actual rates of vaccination in Orleans Parish (solid line) with those modeled under the synthetic control (dashed line). The date of the mandate is indicated by the solid vertical line.
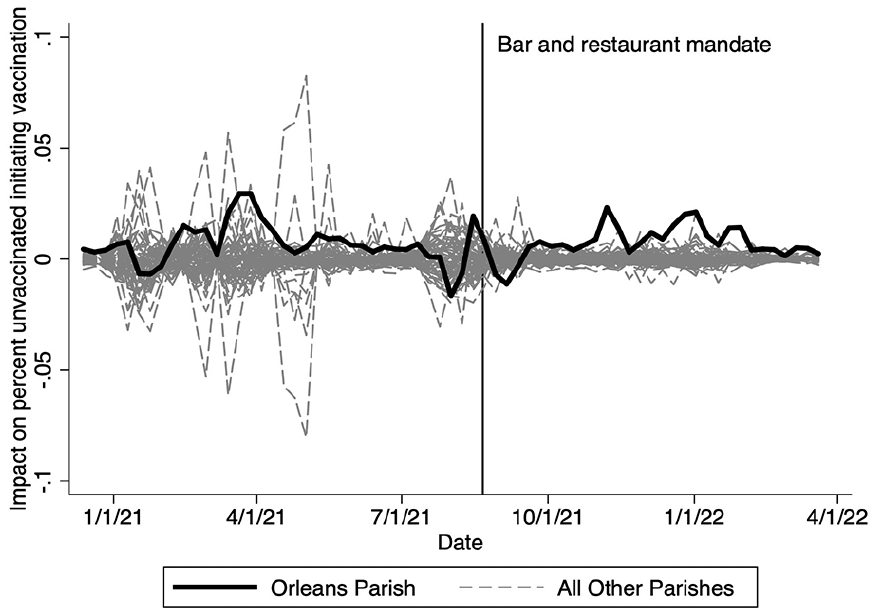
Plot of weighted COVID-19 vaccine rates before and during a vaccine mandate to enter nonessential venues (eg, bars, restaurants) in Orleans Parish (solid black line) compared with all other parishes (gray lines), Louisiana, 2021-2022. The figure shows the difference in the effects of the mandate on vaccination in Orleans Parish (solid line) with all other parishes (dashed line). The date of the mandate is indicated by the solid vertical line.
Discussion
The August 2021 vaccine mandate had a significant effect on the uptake of vaccines in Orleans Parish compared with a synthetic control parish. This mandate was associated with 760 additional vaccines being initiated weekly, higher than what would have been expected in the absence of a vaccine mandate. This mandate was associated with 23 560 additional people receiving their first COVID-19 vaccine dose.
Before implementation of the mandate, 2 periods of elevated vaccine uptake occurred: one in March 2021 and another in late July 2021. These increases in vaccination corresponded to the initiation of universal vaccine availability and the Delta variant, respectively. Although the synthetic control parish revealed a gradual decline in vaccination after the Delta variant, vaccine initiation was sustained at a higher level, even after the Delta wave was in decline in Orleans Parish.
These findings suggest that at a community level, vaccine mandates to enter nonessential establishments can lead to an increase in the number of people who initiate vaccination. Vaccines are important at a population level, both to reduce transmission and to ensure that hospital capacity is maintained. A major push to vaccinate people occurred during the Delta surge, given that most people who were hospitalized were unvaccinated. 22 These findings support the population-level effect of a vaccine mandate for entering nonessential venues during a public health emergency. Moreover, these findings are aligned with research in the European context that demonstrated an increase in COVID-19 vaccination after implementation of a mandate to enter nonessential venues and a study in New York City that showed the effect of a proof-of-vaccination requirement, incentive payments, and employer-based vaccine mandates on vaccine uptake.23,24
Strengths and Limitations
This study had several limitations. First, this analysis was ecological in nature, meaning that we did not examine whether individuals decided to get vaccinated because of the mandate. Some people may have received the vaccine during the intervention period but were unaware of the mandate; as such, causality cannot be inferred at the individual level. Second, we selected the best set of data to minimize the difference between the actual parish and the synthetic control parish in the preintervention period; however, our data selection was limited to variables that were available. Further model refinement may be possible through additional, unmeasured covariates. Third, we were unable to determine whether subpopulations in New Orleans (such as specific age groups or sexes) benefited disproportionately from these mandates, because the publicly available vaccine registry did not contain demographic information. Fourth, the generalizability of this study to similar mandates in other areas may be limited. New Orleans is considered a destination for cuisine and is one of the most bar-dense cities in the United States.25,26 Other cities with fewer similar public venues may not benefit from similar mandates.
This analysis also had several strengths. First, given that vaccination data were based on state records, it is expected that this measurement is precise and there is little misclassification, as this form of measurement is considered the gold standard of measurement of vaccine receipt. 27 Any misclassification would be nondifferential, given that individuals were not asked about their status but, rather, records were pulled for the entire study period. Moreover, the exact timing of mandates was documented and is known. Third, because American Community Survey data were used for demographic variables and to generate model weights, we expected a similarly high level of precision in these variables.
Conclusions
Future research is needed to corroborate these findings at the individual level. Further studies on vaccine hesitancy should consider asking people about the effect of these mandates on their decision to receive the vaccine. This research is especially important moving forward, given that the US Food and Drug Administration indicated that annual COVID-19 boosters will be needed to manage the effects of the SARS-CoV-2 virus. 28 Hence, understanding the effect of structural drivers on vaccine uptake will be critical to maintaining a strong response to COVID-19 and preventing COVID-19–related morbidity and mortality. Moreover, understanding this relationship will be important in the context of a similar health emergency, such as an influenza outbreak.
Vaccine mandates in nonessential venues in Orleans Parish helped overcome the decline in vaccine initiation seen in summer 2021. Public health officials and policy makers should consider adopting similar interventions in the face of further COVID-19 surges if booster uptake is insufficient to reach population-level protection or during future outbreaks of vaccine-preventable diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.