
Abstract
Background:
Vaccination against COVID-19 is considered one of the most effective strategies to control this global public health crisis. However, vaccine hesitancy is one of the main threats to mitigating the pandemic. The present study aimed to identify predictors of intention to vaccinate against COVID-19 in 3 geographical regions of Peru.
Methods:
An online analytical cross-sectional study was conducted. Participants were selected by non-probability convenience sampling and size was estimated using the online statistical calculator proposed by Soper. A total of 529 Peruvian nationals completed the questionnaires. Student’s t-test and Fisher’s F test (ANOVA) were used. A significance level of .05 was considered.
Results:
Face-to-face work (β = 2.037, P < .001), fear of COVID-19 (β = .461, P < .001), vaccine confidence (β = 2.881, P < .001) and trust in health care institutions (β = .432, P < .01) predict a higher intention to receive the vaccine. However, the variables perception of a worldwide conspiracy (β = −1.900, P < .001), and practice Protestant religion (β = −2.274, P < .001) predict negatively their acceptance.
Conclusion:
Several positive predictors of intention to vaccinate against COVID-19 have been identified. However, having a perception of a global conspiracy and practice Protestant religion are shown to be risk variables for vaccine acceptance. Therefore, there is a need to develop strategies to ensure high uptake and success of COVID-19 vaccination campaigns.
Introduction
COVID-19 infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused enormous disruption to societies and the loss of millions human lives.1,2 In addition, COVID-19 has instilled fear in the population due to the dead consequences and negative impacts on the health and economic systems.1,2 On the other hand, several high- and middle-income countries compete unequally with low-income countries for vaccine procurement. Additionally, high-income countries retain their intellectual property for COVID-19 vaccines and other technologies, sparking outrage over vaccine inequities as global access to the vaccine enables diverse immunization strategies. and thus face the imminent epidemic waves caused by the new variants of COVID-19.3,4 As of January 28, 2022, 33 vaccines have regulatory approval in at least 1 country, based on the results of interim Phase III clinical trials, with published data reporting efficacies between 50% and 95% and, in some cases, no published results. 5 All of these vaccines, in addition to providing direct immunity, can help reduce infections, even among unvaccinated people, through herd immunity. 6 It is therefore crucial to convince populations that doubt vaccines of their vital importance in the fight against this virus and in the prevention of the appearance of new variants. 7
In Latin America, low-income countries such as Peru have reported the highest per capita deaths globally and an increasing number of cases 8 ; it is therefore necessary to promote vaccination against COVID-19 to reduce the number of infected and dead people and to reactivate the economy to achieve a better quality of life and equal opportunities for the population. 9 Different studies indicate the influence of various factors on confidence acceptance or risk attitudes when receiving a vaccine.10,11 These factors differ according to ideological, regional, social, and cultural factors.10,11 Therefore, understanding the factors that influence vaccination in developing countries, with scarce economic resources, low levels of education, health systems on the verge of collapse, distrust toward manufacturing countries, fear of side effects, and serious misinformation problems such as Peru, is of vital importance to develop solid public health policies. 12
Vaccine hesitancy is a globally common phenomenon and is characterized by the acceptance or refusal of vaccination despite its availability and active service. 13 Confidence in the vaccine provides assurance of its efficacy, but by resorting to a wide range of false information about vaccination, it leads to the formation of beliefs contrary to scientific evidence about the importance of vaccination, which, in turn, leads to risky and fearful behaviors. 14 These aspects become potential agents based, generally, on conspiracy theories. 15 In Peru, scandals related to the misuse of vaccines by senior government officials, authorities, and staff in the Ministry of Health, including research team members and university administrators where clinical trials of Sinopharm’s SARS-CoV-2 vaccine were being conducted in the midst of a health, political, and economic crisis, influence risk behavior toward vaccination. 16 Indeed, trust in government and health professionals plays a key role in people’s decision to vaccinate against COVID-19. 17
Public health institutions around the world have developed vaccination strategies to control the pandemic, and surveys show that participants are reluctant to vaccinate or to receive any particular vaccine. 18 The exact proportion of the population that must be vaccinated against COVID-19 to begin to observe effective herd immunity is unknown, however, it is estimated to be between 70% and 80%. 19 In Peru, despite increasing vaccination levels every day, only 29% of the population has been immunized by September 18, 2021. 20 The main groups immunized so far are older adults and people with certain comorbidities. The large margin of the population that has not yet been vaccinated has a high risk of becoming infected with any variant, especially the young or those who have not accepted vaccination for different reasons. In addition, the country presents a remarkable socioeconomic inequality due to the quarantine. The scarcity of resources caused poverty to increase considerably. The intrinsic limitations of the health system due to lack of infrastructure and trained personnel throughout the country and lack of access to social programs have made the poorest regions vulnerable. 21 In view of this, socio-demographic factors such as sex, age, education, employment status, among others, are important determinants when in regard to vaccination.22,23 Other reasons against the intention to be vaccinated that cause a decrease in acceptance are certain religious beliefs. Catholics oppose the use of vaccines derived from aborted human fetuses, they suggest that these vaccines should be avoided and proposes a search for alternatives. In the case where no alternative vaccine is available, the use of the existing vaccine is morally acceptable in order to avoid serious risks for the population. By the other hand, Protestants highlight individual freedom, the Orthodox reject the vaccine because it is an act of interfering with divine providence, while the pro-vaccine Protestants believe vaccination to be a gift of God. 24 These circumstances threaten pandemic control strategies and aggravate the health crisis in which the country finds itself, so there is concern about the imminent arrival of the third wave, similar to the cases documented in European countries. 25
Thus far, there is little evidence on the intention to vaccinate against COVID-19 in Latin American regions such as Peru, a country that presents major socioeconomic, logistical systems, and infrastructure barriers to vaccination coverage. 26 Consequently, it is critical to understand the predictors of vaccine hesitancy in the country. The objective of this work is to identify predictors of intention to be vaccinated against COVID-19 in a Peruvian sample from 3 geographical regions of the country to help improve vaccination strategies and coverage.
Materials and Methods
The present study has a quantitative approach and was conducted with a cross-sectional analytical design.
Participants
The non-probabilistic convenience sampling method was used for the selection of participants. The sample size was estimated using a statistical calculator proposed by Soper. 27 A minimum recommended sample size of 293 participants was estimated, considering 15 possible predictor variables, an anticipated effect of 0.1, a significance level of .05, and a statistical power of 0.95. However, 529 Peruvian nationals completed the questionnaires.
Instruments
Registration form for sociodemographic data and other variables of interest
Sociodemographic data were collected, such as age (<45 and >45 years), sex (women and men), region of origin (coast, highlands, and jungle), level of education (basic, technical, and university), religion (Catholic, Protestant, other, and non-professional), and type of work (not working, teleworking, and on-site). Moreover, the following data were collected: personal history of COVID-19, family history of COVID-19, presence of disease, and perception of a global conspiracy. Responses to these items were dichotomized (yes or no). On the other hand, the following information related to fear of COVID-19 was collected: “Is COVID-19 dangerous?,” considering the following response categories (1) moderately dangerous, (2) very dangerous, and (3) not dangerous; “I am very afraid of COVID-19”; “I trust in the efficacy of the vaccine”; “I am afraid of losing my life due to COVID-19”; “the Peruvian government is interested in the welfare of citizens”; “health professionals will do whatever it takes to give me the medical care I need”; “when they treat my medical problems”; and “health institutions prioritize my medical needs.” The response options were (1) strongly disagree, (2) strongly disagree, (3) somewhat disagree, (4) neither agree nor disagree, and (5) somewhat agree.
Brief scale of intention to vaccinate against COVID-19: This questionnaire consists of 6 ordinal items that measure people’s intention to be vaccinated against COVID-19 through 7 items (1 = total disagreement and 7 = total agreement) allowing participants to choose the alternative with which they most identify. It is divided into 2 subscales: acceptance and attitude toward risk. The internal consistency was α = .91, as well as for its dimensions: acceptance α = .88 and risk attitude α = .83. The instrument has been validated in a Peruvian sample and has adequate psychometric properties.
Procedure
The study was evaluated and approved for execution by the ethics committee of the Universidad Peruana Unión. An online questionnaire was developed using a Microsoft Forms form, which was disseminated through social networks, such as Facebook and WhatsApp Messenger. The participants agreed to the questionnaire where they were presented with information on the aims and objectives of the study. The privacy of the participants was respected and it was explained to them that the data would be used only for research purposes. In addition, they were informed of their voluntary withdrawal at any time during the data collection process. Through this questionnaire, electronic informed consent was obtained from the participants. Only those who agreed to participate voluntarily and signed the informed consent form were included. The administration time of the questionnaire was approximately 10 min. Data submitted for analysis were collected during the months of May and June 2021 and were processed in a Microsoft Excel template.
Data Analysis
First, a descriptive analysis was made of the sociodemographic characteristics according to the sex of the participants and which were considered as possible predictors of the intention to be vaccinated against COVID-19. Second, a bivariate statistical analysis was performed, using Student’s t test to compare 2 groups and Fisher’s F test (ANOVA) to compare more than 2 groups and identify variables related to the intention to vaccinate, with a level of significance of .05 for these analyses. To identify predictors of intention to be vaccinated against COVID-19, a multivariate analysis was performed, where the factors that were significantly associated (P < .05) were included in a multiple regression model and the backward stepwise elimination method was applied, considering a significance level of .10. Statistical analyses were performed with R program version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org) and IBM SPSS statistical program, version 24 (SPSS Inc., Chicago, IL, USA).
Results
Results were obtained from 529 participants who completed online questionnaires and reported their sociodemographic characteristics and intention to vaccinate against COVID-19 (Table 1). The mean age was 38.48 years (±11.35) and there was greater participation of the female sex (69.8%). Information was also obtained from participants from the coast (51.8%) and sierra (40.8%). The participation of citizens with university (49.7%) and postgraduate (25.3%) levels of education was observed. Regarding the religion, they profess, there is a greater presence of Catholics (55.6%) and Protestants (30.4%). Most of the participants worked in person (55.6%). There was a lower proportion of people who had COVID-19 (31.4%), and a greater presence of those who had a family member who had contracted the disease (58.8%). Only one-third of the participants reported having a chronic disease (24.4%).
Sociodemographic Characteristics of the Study Sample.

Abbreviations: n, absolute frequency; %, relative frequency.
Comparative analyses (Table 2) showed that the intention to vaccinate against COVID-19 was significantly higher in those coming from the coast of the country compared to those coming from the highlands or jungle (P < .01). Similarly, higher scores were observed in those with graduate level education compared to those with university, technical or basic education (P < .001). Regarding religion, those who reported being Catholic or not professing any religion reported a higher intention to be vaccinated compared to those who were Protestant (P < .001). Moreover, those who worked face-to-face had higher intention to vaccinate compared to those who worked remotely or virtually and those who did not work (P < .001). No significant differences were found in those who had a history of having been ill with COVID-19 and those who did not acquire the disease, nor in those who did or did not have a family member with this history (P > .05). Similarly, there were no significant differences between those who did or did not have any chronic pathology (P > .05). However, the intention to be vaccinated was lower in those with a perception of a global conspiracy (P < .001).
Differences in Vaccine Intention Means According to Sociodemographic Factors.
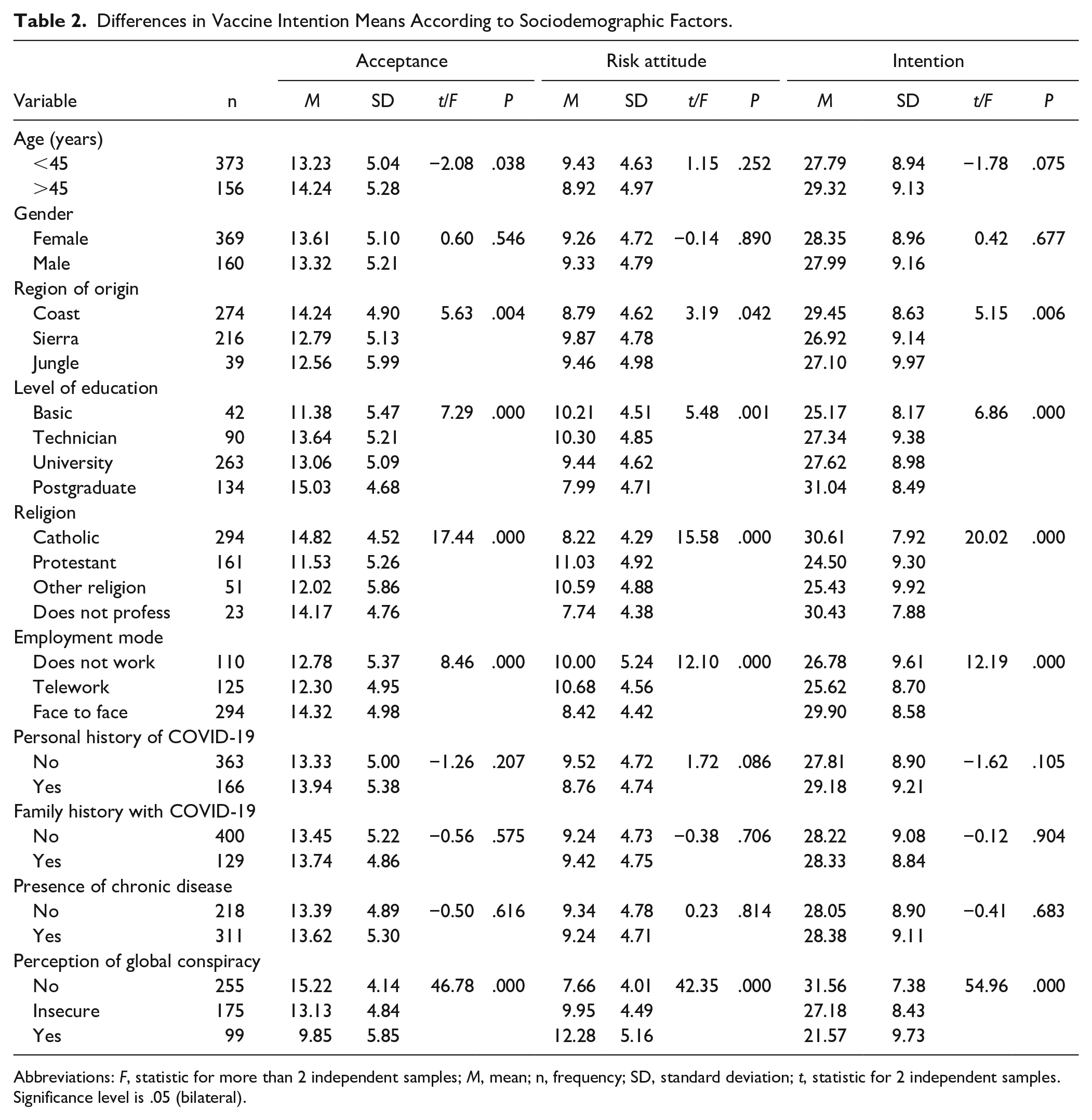
Abbreviations: F, statistic for more than 2 independent samples; M, mean; n, frequency; SD, standard deviation; t, statistic for 2 independent samples.
Significance level is .05 (bilateral).
Because the intention to vaccinate against COVID-19 scale is made up of 2 factors: acceptance and risk attitude and together they yield an overall score, a correlation analysis was performed (Table 3) and it was found that the variables fear of COVID-19, confidence in the vaccine, confidence in the government, confidence in health professionals, and confidence in health institutions correlated significantly (P < .01) positively with intention to be vaccinated against COVID-19 and with the acceptance factor and correlated negatively with the risk attitude factor.
Correlation Analysis Between Predictors and Vaccine Intention.

Abbreviations: DE, Standard deviation; g1, Skewness; g2, kurtosis; M, Mean.
Correlation is significant at the .01 level (bilateral).
In the linear regression analysis (Table 4), all variables that were significantly related were considered as predictors. Thus, variables such as: region of origin (0 = No coast, 1 = Coast), level of education (0 = no postgraduate degree, 1 = postgraduate degree), religion (0 = Catholic/non-professing, 1 = Protestant), work mode (0 = telework/not working, 1 = face-to-face), perception of a global conspiracy (0 = No, 1 = Yes), fear of COVID 19, confidence in the vaccine, confidence in the government, and confidence in health institutions were included in the model. The results show that there are variables that negatively predict vaccine intention against COVID-19 (R2 = .594; F-test = 127.539; P = .000). Being a Protestant (β = −2.274, P < .001) and perception of a global conspiracy (β = −1.900, P < .001) are related to lower vaccine intention. Likewise, face-to-face work mode (β = 2.037, P < .001), fear of COVID-19 (β = .461, P < .001), confidence in the vaccine (β = 2.881, P < .001) and confidence in health institutions (β = .432, P < .01) are related to higher intention to vaccinate against COVID-19.
Predictors of Intention to Vaccinate Against COVID-19.
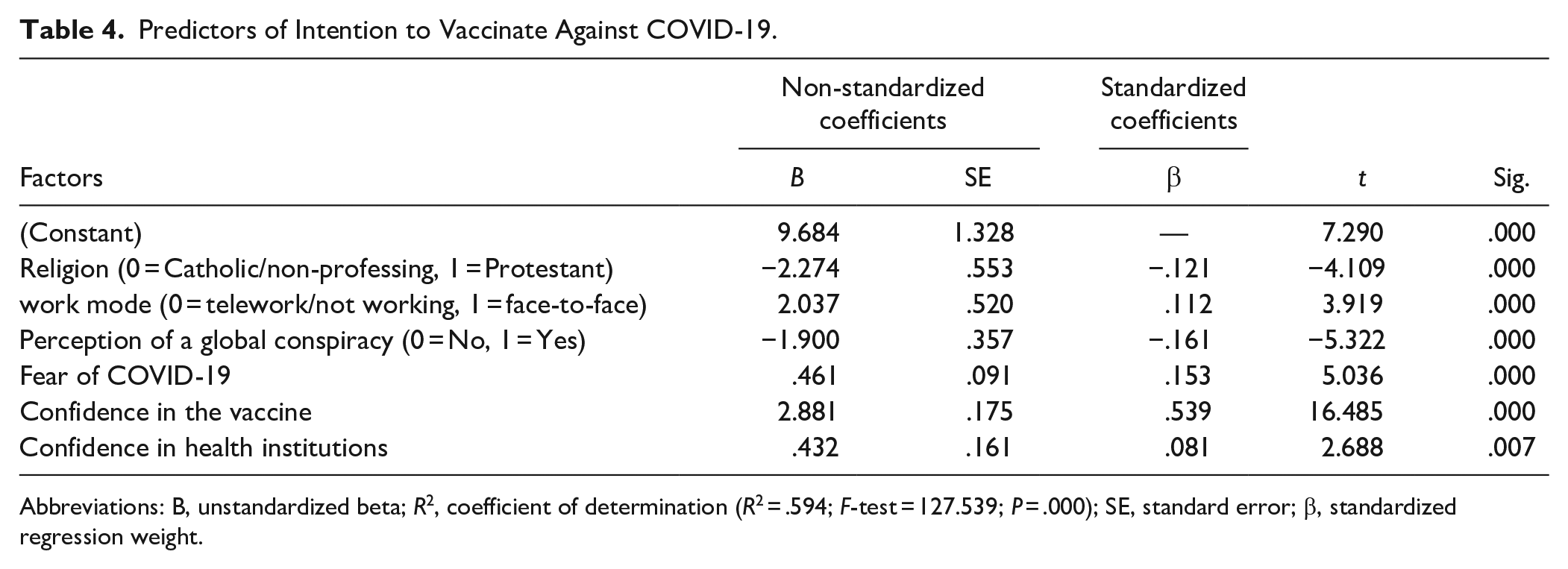
Abbreviations: B, unstandardized beta; R2, coefficient of determination (R2 = .594; F-test = 127.539; P = .000); SE, standard error; β, standardized regression weight.
Discussion
There is evidence that vaccines against COVID-19 are effective in preventing death, as well as having an inverse relationship with disease severity. 28 Therefore, ensuring the acceptance of the COVID-19 vaccine is a relevant issue. To this end, it is necessary to know the factors that predict the intention to receive COVID-19 vaccines. In this study conducted in the Peruvian population, it was found that the modality of face-to-face work, fear of COVID-19, confidence in the vaccine and trust in health institutions predict a greater intention to receive the vaccine; while the perception of a world conspiracy and being a Protestant are shown as variables that negatively predict its acceptance.
Confidence in vaccine efficacy has a positive correlation and a significant effect on the intention to be vaccinated against COVID-19. This can be explained by comparing to other countries such as France and Italy, which indicate that beliefs in vaccine efficacy have emphasized the importance of severity, susceptibility, benefits, perceived barriers, and trust or distrust in biomedical research associated with the vaccine.7,29 In sum, potential vaccine efficacy conveyed through professional information sources that address vaccine concerns, clarify misinformation, and disseminate evidence-based information increase confidence and safety in the population, 30 raising the likelihood of vaccinating and protecting others as a collective responsibility, and including children. 31 In view of this, the authorities must effectively convey public health messages so that the population voluntarily accepts a vaccine against severe COVID-19 disease. 32 While the government plays an important role in addressing the COVID-19 pandemic, the Peruvian government’s communication was initially poor as it promoted anti-scientific approaches in the media and published COVID-19 guidelines that included incomplete descriptions of its methodology and drugs without scientific support for their efficacy. 33
In addition, structural weaknesses in the Peruvian health system were the fragmentation and inequality of the population that undermined the government’s delayed response and led to a decline in vaccination coverage. The collapse of the health systems in the poorest and weakest cities was evident, as they lacked infrastructure and human resources, in addition to the increased risk of other diseases, the shortage of medicines, and poor follow-up of patients hospitalized for COVID-19 indicated a minimal mitigation response,34,35 and the reluctance of the population and companies to comply with prevention measures. 36 This parallels our results showing a significant negative correlation between trust in government and risk-taking behavior. On the contrary, the vaccination plan in Peru has received adjustments according to the situation and progress of the pandemic, showing a substantial decrease in mortality in medical and elderly populations by generating protective immunity. 37 This can be reflected in the results because confidence in the government showed a significant relationship with acceptance. Therefore, more effective communication by government authorities about the individual and collective benefits of immunization would be an appropriate strategy to make the majority of the population intend to vaccinate against COVID-19.
On the other hand, confidence in health institutions also has a positive correlation and behaves as a significant positive predictor of the intention to vaccinate. Similar studies show that trust in institutions is a strong predictor of vaccine acceptance, while lack of scientific knowledge increases distrust in medical institutions.38,39 The discrepancies and inconsistencies in different official sources from national and international health institutions, as well as the lack of clarity in health advice on preventive measures such as social distancing, and above all vaccination, only serve to sow the seeds of confusion. Therefore, vaccination campaigns provided by health institutions should highlight the benefits of vaccination, maintaining a high level of transparency regarding the safety and efficacy of vaccines. 18
Fear of COVID-19 has a significant effect and a positive correlation was also found with the intention to vaccinate. Other studies in the same population also suggest that perceived risk of becoming infected, fear of the severity of the disease, or knowing an infected friend or relative were predictors of intention to receive the vaccine. 40 Fear of becoming seriously ill and its adverse effects is an important predictor of vaccine acceptance,41,42 this is probably because awareness of a threat activates proximal defenses and reduces the sense of vulnerability or eliminates the dangerous stimulus causing people to make decisions and adopt healthy behaviors. 43 On the contrary, an excessively pronounced fear generates panic, an attitude charged with negative emotions toward the pandemic that chronically leads to an inability to adopt preventive measures in an adequate and adaptive manner. 44 Consequently, sound scientific advice on COVID-19 is essential for managing fear and avoiding panic, especially in the most vulnerable groups in society: the elderly, the sick, and those with mental health problems prone to anxiety and panic.
With respect to the mode of face-to-face work, this has a positive correlation with the intention to vaccinate, which is why it behaves as a positive predictor. These findings are consistent with studies of intention to vaccinate among young adults and older adults at increased risk for COVID-19 due to their employment status. 45 It is likely that the gradual return to work in person after the confinement ordered by the government is generating in workers the intention to receive the vaccine to feel more protected against possible exposure. On the other hand, differences in vaccine acceptance have been found among different occupational occupations, which may be attributed to differences in knowledge about COVID-19 and vaccines. 46 For this reason, it is necessary for companies and workplaces to follow the guidelines for the surveillance, prevention, and control of their workers’ health.
Interestingly, Protestant religious affiliation was associated with a lower intention to accept the vaccine, studies in the South American context such as Venezuela presented similar results. 47 This may be attributed to a lower perceived risk by members of these churches, due to religious values or media influence and social ties that form personalized attitudes toward science, the risks associated with vaccines, and trust in the health care system.48,49 In comparison with Catholics, Peru presents a model of Church-State relations that coordinates and promotes the relations between the executive branch and the church, supporting the measures taken by the government, providing a better response despite the freedom of worship. 50 It is estimated that there are around 4 million Protestants in Peru, 51 the design of vaccination strategies and promotion of vaccination should involve religious leaders and their communities.
The use of words such as “plague” and “apocalypse” has intensified during the current pandemic, in which a great deal of false or inaccurate information about the origin, forms of infection, treatment, and vaccination has been disseminated by the press and social networks, 52 and even considered the pandemic as a global conspiracy. 53 In the current study, the perception of a global conspiracy was found to be a negative predictor of vaccine acceptance. There is evidence indicating an inverse relationship between conspiracy belief and adherence to basic health guidelines. 54 In addition, COVID-19 conspiracy believers showed less likelihood of adopting health behaviors that cannot be performed independently, such as being screened and vaccinated against COVID-19. This negative link between conspiracy beliefs and health-protective behaviors appears to be driven by the perception that they are less beneficial and more risky. 53 It is urgent to promote objectivity and belief based on scientific evidence to avoid misinformation and the proliferation of conspiracy theories in the population and thus reduce the risk of non-acceptance of the vaccine.
This is a cross-sectional study conducted in a non-probabilistic convenience sample over a restricted period of time, which implies certain specific limitations. The lack of representativeness and the different number of samples for each region of the country is the main limitation, there is very little participation of inhabitants of the jungle region (about 7%), so it is not possible to generalize the results to the population of the country. Additionally, there is an over-representation of female individuals and all data collected are self-reported and this could make them not completely reliable.
Conclusion
The findings of the current study have shown that there are different positive predictors of intention to vaccinate against COVID-19, among them are trust in the vaccine and health institutions, face-to-face work mode, and fear of COVID-19. On the other hand, having a Protestant religious affiliation and the perception of a global conspiracy are shown to be risk variables for vaccine acceptance. Therefore, there is a need to develop strategies to achieve high uptake and ensure the success of COVID-19 vaccination campaigns.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.