
Abstract
Objectives:
Child sex trafficking (CST) is the involvement of minors in the commercial exchange of sex for goods, services, drugs, or money. The COVID-19 pandemic negatively affected many risk factors associated with CST victimization and the availability of CST services. We examined service providers’ perspectives on how the pandemic affected trajectories of CST victimization among young people in the United States.
Methods:
We collected qualitative data from 80 law enforcement professionals and service providers working with young people affected by CST from 11 US cities. Semistructured interviews lasted approximately 1 hour and were digitally recorded, transcribed verbatim, and coded via a grounded theory approach.
Results:
We found 3 overarching themes related to the pandemic’s effect on CST victimization trajectories: grooming, perpetration, and service provision. Participants described how increased online activity may have increased the risk of CST, even among children without traditional risk factors. However, technology also facilitated young people’s agency in seeking help and receiving services. In addition, participants reported increases in virtual service provision that facilitated access to, and availability of, CST services more generally.
Conclusions:
Technology use among young people increased during the pandemic, leading to increases in the risks of experiencing technology-facilitated CST. Technology use among young people who experience CST victimization—and how it may differ from young people more generally—is underexplored and may provide insights into prevention and treatment. Collectively, results highlight the need for epidemiologic research to help identify how global and national events affect trajectories of victimization among young people.
Child sex trafficking (CST) is the involvement of a minor in the commercial exchange of sex or sexual acts for goods, services, drugs, or money. CST represents a range of victimization scenarios: survival sex (wherein a child exchanges sex or sexual acts for necessities such as food or shelter), exchanges facilitated by a third party (eg, a family member, intimate partner, pimp, friend), or a minor acting alone. The effects of the COVID-19 pandemic on CST victimization have yet to be established. 1
The pandemic’s effect on CST victimization (inclusive of revictimization) warrants special consideration because of young people’s developmental stage, their relative lack of freedom to leave dangerous home environments, and their reliance on adults for basic needs. 2 The pandemic increased exposure of young people to many known risk factors for CST, such as interpersonal violence, social isolation, and increased economic strain.3,4 In addition, the pandemic had negative effects on the mental health of young people, 5 which is widely associated with CST victimization. 4 The psychosocial effects of the pandemic coupled with the unique risks that young people experience from victimization warrant a deeper understanding to prevent CST victimization of young people.
Even before the pandemic, CST profiles of victimization were changing in ways related to developments in technology and communication. Recent research highlights the growing issue of sexual abuse images produced by young people, made more widespread by the use of smartphones. 6 Furthermore, the use of social media has been almost ubiquitous among young people across the United States, and data suggest that such use is poorly monitored by caregivers because of a lack of understanding and awareness of online risks. 7 The onset of the COVID-19 pandemic may have exacerbated these dynamics. The pandemic also resulted in increased online activities by unsupervised minors. 3
Taken together, it seems likely that the pandemic increased several known risks for CST 8 ; the same challenges simultaneously changed service options for young people at risk for CST or the victims thereof. Many community services either disappeared or transitioned online, limiting positive interpersonal and psychological supports, including mental health services. 9 Such services are a key component of extant CST prevention and intervention strategies.10,11 Accordingly, the changes to service provision during and since the pandemic may have reduced the availability of and access to CST prevention and intervention services for many young people at risk for CST victimization, including those enduring ongoing victimization. 12
More research is needed to understand how the pandemic affected trajectories of CST victimization, including pre- to postexploitation experiences. Shifts that occurred during the pandemic may be here to stay. Thus, it is important to understand the changes so that prevention interventions can be directed accordingly. Professionals who work with CST survivors are in a unique position to describe these changes, particularly those who have worked with young people affected by CST victimization before, during, and after the pandemic. We collected qualitative data from 80 professionals about their perspectives on how the pandemic may have affected trajectories of CST victimization.
Methods
Study Sample
Participants
We collected qualitative data from 18 law enforcement professionals and 62 social service providers from 11 US cities. Cities were purposively drawn from communities with varying geographic regions, sizes, and scores on Shared Hope International’s 2018 Protected Innocence Challenge. 13 The Protected Innocence Challenge creates state report cards in which 41 components of state law are evaluated by their intention to create a safer environment for young people. States are then given a letter grade of A, B, C, D, or F. An “A” indicates the greatest intention to create safety for young people, while an “F” indicates the least intention to create safety for young people. Middle scores (B, C, D) can reflect 1 of 2 evaluations: first, that some components of state law have great intentions to create safety for young people while other components do not; second, that intentions to create safety for young people are moderate to low across all components. To capture variability in response in a state, we differentially sampled rural areas in states that received higher grades so that we could capture service provision and legal response in areas that may traditionally have access to fewer medical and social service resources, such as those operating outside of urban areas.
Participant recruitment began with local police departments. Study personnel called law enforcement agencies in the identified cities, provided an oral prospectus of the study, and asked for a suitable person at the agency to participate in a 1-hour interview. Study details were also provided via email. Before interview took place, the interviewer received the participant’s oral consent to conduct and digitally record the interview. Upon completion of the interview, police were thanked for their time and asked to provide the name and contact information of individuals with whom they had worked or were familiar from the community who served CST victims. All individuals working at agencies identified in this way were contacted via telephone or email, invited to participate, and asked to nominate others in the community who were suitable for study participation. This process continued in each community until saturation was met, as evidenced by the same names being referenced more than twice. The final sample of 80 professionals reflects this process. All participants were provided a $25 Amazon gift card in appreciation of their time. Each community in the study had a mean of 7 (range, 4-11) participants per community. Interviews lasted approximately 1 hour, with an average length of 44.3 minutes. The University of New Hampshire Institutional Review Board reviewed and approved all protocols.
Data collection and analysis occurred concurrently so that analyzed data could guide subsequent data collection efforts. 14 Semistructured interview guides included questions such as “What has been the impact of COVID on CST in your community?” The interviewer took detailed case notes capturing nonverbal cues for each interview. The first author (J.E.O.) completed all interviews. Probes elucidated answers and prompted depth of response.
Demographic surveys
The research team collected demographic information from participants: age, race, sex/gender, employment, length of time in current position, and education. Completion of the demographic survey was not mandatory for study participation. Of 80 individuals, 69 (86.3%) completed the demographic form. These data were collected via online survey.
Data Analysis
A transcription service transcribed all digital recordings of interviews verbatim, and research team members subsequently reviewed transcripts for accuracy while integrating case notes. Interviews were coded via an iterative coding process wherein the first author (J.E.O.) and the fourth author (G.Z.K.) used a grounded theory approach. Both individuals had training in grounded theory analysis and familiarity with research in the topic area, and the first author had experience as a CST service provider. Participants’ references to the pandemic were coded holistically as “COVID.” Subsequently, all qualitative data initially coded as “COVID” were reviewed and recoded by the first author (J.E.O.) and a master-level research associate for variations and themes related to the pandemic. These 2 coders (1) reviewed all code phrases developed during the first round of coding with interview transcripts, (2) reduced code phrases by subsuming overlapping categories, (3) created higher-level conceptual clusters of codes, and (4) ultimately abstracted major themes from these categories. During this round of coding, coders implemented constant comparison procedures by comparing existing themes with the themes generated from each analysis. 15 The first author (J.E.O.) determined levels of themes within and across interview transcripts by applying systematic review strategies. 16
Methods to enhance the rigor of the research were as follows: regular debriefing; consultation on the semistructured interview guide from 6 researchers with experience in CST service and service provision and/or community response to CST; the use of detailed case notes capturing nonverbal participant cues; and data triangulation by using more than 1 method to collect similar data (ie, surveys and interviews 16 ). Throughout the Results section, we use the terms most (>75%), many (>50% to ≤75%), some (>25% to ≤50%), and a few (≤25%) to denote participant agreement with the described sentiment. We did not provide exact numbers of participants expressing a given sentiment because such numbers may be misleading and/or not representative of participants’ true feelings. For example, should a sentiment not be expressed in an interview, its absence may not necessarily indicate disagreement by the participant; rather, it may have simply failed to occur organically in the semistructured interview format. Participant quotes facilitate understanding of author voice. Quotes were chosen because of their representativeness of themes and participant perspectives.
Results
We collected data from 80 law enforcement professionals, advocates, lawyers, mental health professionals, and direct care staff who had been working in their fields for an average of 2 to 6 years (Table). We found 3 overarching themes related to the pandemic’s effect on CST victimization trajectories: grooming, perpetration, and service provision.
Characteristics of the law enforcement professionals and service providers participating in qualitative interviews on the effect of COVID-19 on child sex trafficking, United States, June 2021–April 2023
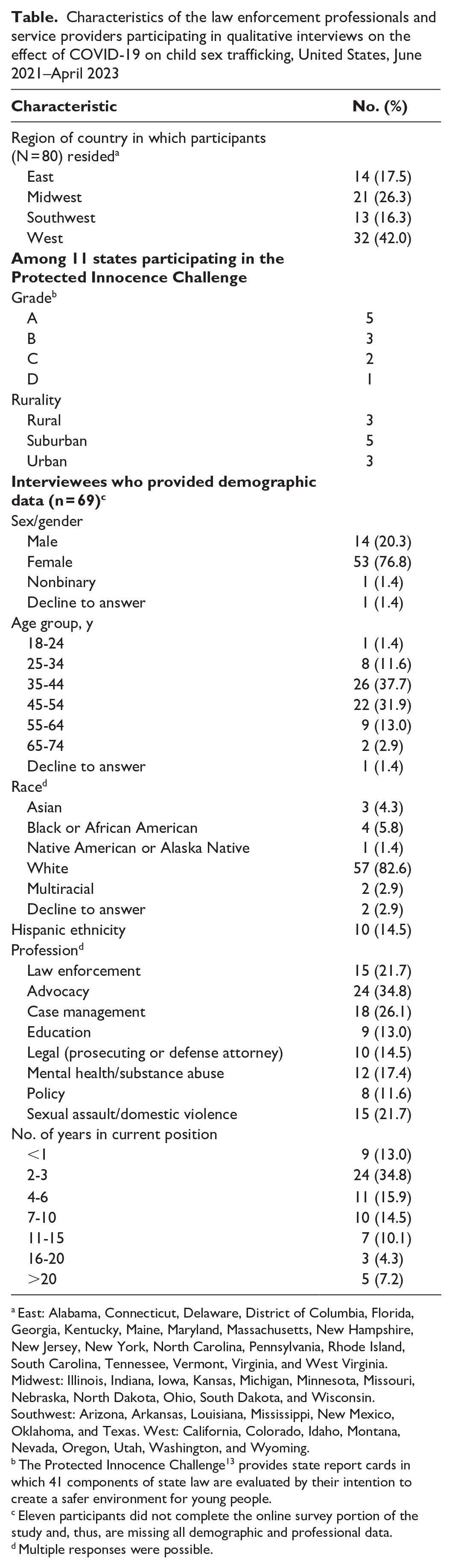
East: Alabama, Connecticut, Delaware, District of Columbia, Florida, Georgia, Kentucky, Maine, Maryland, Massachusetts, New Hampshire, New Jersey, New York, North Carolina, Pennsylvania, Rhode Island, South Carolina, Tennessee, Vermont, Virginia, and West Virginia. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. Southwest: Arizona, Arkansas, Louisiana, Mississippi, New Mexico, Oklahoma, and Texas. West: California, Colorado, Idaho, Montana, Nevada, Oregon, Utah, Washington, and Wyoming.
The Protected Innocence Challenge 13 provides state report cards in which 41 components of state law are evaluated by their intention to create a safer environment for young people.
Eleven participants did not complete the online survey portion of the study and, thus, are missing all demographic and professional data.
Multiple responses were possible.
Grooming
The term grooming refers to the gradual initiation and maintenance of a relationship between a perpetrator and a victim. Subjection to grooming behaviors is a risk factor for childhood victimization, including CST. This theme is characterized by participants’ descriptions of how grooming was affected or changed by the pandemic. Most participants indicated that grooming moved online during the pandemic: Unfortunately, we are all spending a lot of time on computers and with technology, and that really is increasing the risk for human trafficking. Traffickers aren’t able to pick [potential victims] up or identify them more in the community setting. So, they also are turning online to identify these kids. (service provider, West)
Grooming occurred online for varied reasons. Many participants noted that grooming changed because young people were online more frequently during the pandemic than before it; therefore, perpetrators had more access to them: When COVID-19 hit and remote learning started occurring, students were given iPads through the district . . . they were using that to access their social media, so recruitment was occurring in that way. (service provider, Midwest)
Others noted that online grooming was likely easier for perpetrators; as such, the pandemic merely accelerated a trend that was already starting: A perpetrator’s ability to access young people is so much easier and so much faster online versus, you know, showing up at a mall or all the places they might have before. That honestly would have taken more effort on their part. (service provider, East)
Most participants reported that while the methods of grooming and recruitment changed during the pandemic, they saw equal—if not more—reports of grooming and CST recruitment throughout the pandemic: I think there was this thought that with [COVID-19], trafficking would actually decrease because people would be worried about getting infected. That was not the case because you can connect with kids online. (service provider, Midwest)
Perpetration
Perpetration refers to acts that constitute CST, including any exchange of sex or sexual acts for goods, services, drugs, or money. This theme captures participants’ reflections on how the pandemic affected the ways that traffickers and buyers perpetrated CST. As with grooming, most participants noted an increase in the perpetration of CST online: Before, when I was looking for these kids, I would just go down to the track [area of high prostitution within city or urban area]. But now I don’t even bother to leave my desk. I just go online and, once you know how to search, you can find all the same kids. (service provider, South)
Most participants mentioned specific sites that traffickers and young people used to facilitate sexual exchanges—especially through sugaring, where young individuals exchange sexual images or services for goods such as designer clothes, cars, or housing: I know that there have been a lot of conversations surrounding “sugaring” . . . and there’s an additional layer of OnlyFans really kicking into gear during [COVID-19] and it being glamorized and sensationalized. (police, West)
Additional sites mentioned by a few participants included SugarBabies, Facebook, and Snapchat. Notably, some participants reported that sometimes young people are not aware that perpetration is occurring, decreasing the likelihood for help-seeking and adult intervention. A service provider in the West said, “What we see is confusion. Sometimes the kiddos didn’t even know what they were engaged in, but they were being preyed upon.” Finally, some participants noted that perpetrators were luring victims to distant cities with promises of a relationship or romance, heightening the risk of ongoing victimization: During [COVID-19], a lot of the girls that we got in were catfished, groomed, given a bus ticket, came to [interviewee’s city] because some guy was going to take her out for a big dinner, . . . and then turned out [prostituted] within 24 hours. We didn’t used to. That’s a dramatic shift from the girls that we got before [the pandemic]. (service provider, East)
Service Provision
Service provision refers to services meant to stop CST victimization or revictimization. This theme encompasses the effect of COVID-19 on CST prevention. Participants universally acknowledged the difficulty in providing and referring young people to services during the pandemic. Most participants noted that over time, police and service agencies were able to shift their outreach and service model to meet increasingly online demands: We were only in person, and then when [COVID-19] hit, everything went telehealth. And we’ve actually seen a lot of success with that. I think it was a difficult transition at first. (service provider, Southwest)
Ultimately, many participants reported that these programmatic shifts increased participation and ensured a more diverse client pool, including parents/caregivers, siblings, and those with limited English proficiency: We had much more progressive participation and more parent participation and also it allows [clients and/or their families] to keep their camera off. So, for those who I think didn’t feel comfortable being face-to-face with all these providers, they’ll participate—we keep their camera off. Whereas before [COVID-19] we didn’t get as much, just, patient variance. So, it’s been an interesting side effect if you will. (service provider, East)
Some participants noted that the shift to online service provision was unlikely to return to its prepandemic structure. Reasons for this included ease of delivery, diversity of clientele, and program acceptability: When we came out of [COVID-19], we were back in presentations, but the sustainability of that is very challenging financially, certainly, but also the dynamics of the schools changed dramatically after [COVID-19] . . . and so what we realized was we needed to have a pretty extensive training for them to have the curriculum, both in person or via Zoom, depending on the size. (service provider, Midwest)
Discussion
In the current study, a diverse group of professionals from 11 US cities discussed the effect of the pandemic on CST victimization trajectories. Respondents reported changes that they had seen in 3 categories: grooming, perpetration, and shifts in service provision. Generally, respondents highlighted a shift to online perpetration of CST in the United States and the use of online methods to lure victims to an in-person setting where perpetration would occur. In many ways, results suggest that the pandemic accelerated changes that were already in process. Respondents reflected on the simultaneous move of therapeutic and victim services to online structures. This change disrupted the provision of needed supports, but respondents also uniquely emphasized that there were ways in which the move to online services expanded options for young people, provided services in environments that reduced the need for travel, and were more comfortable for young people. The interrelationships for young people related to technology’s benefits, challenges, and COVID-19–specific interventions in the context of CST victimization are represented visually in the Figure.
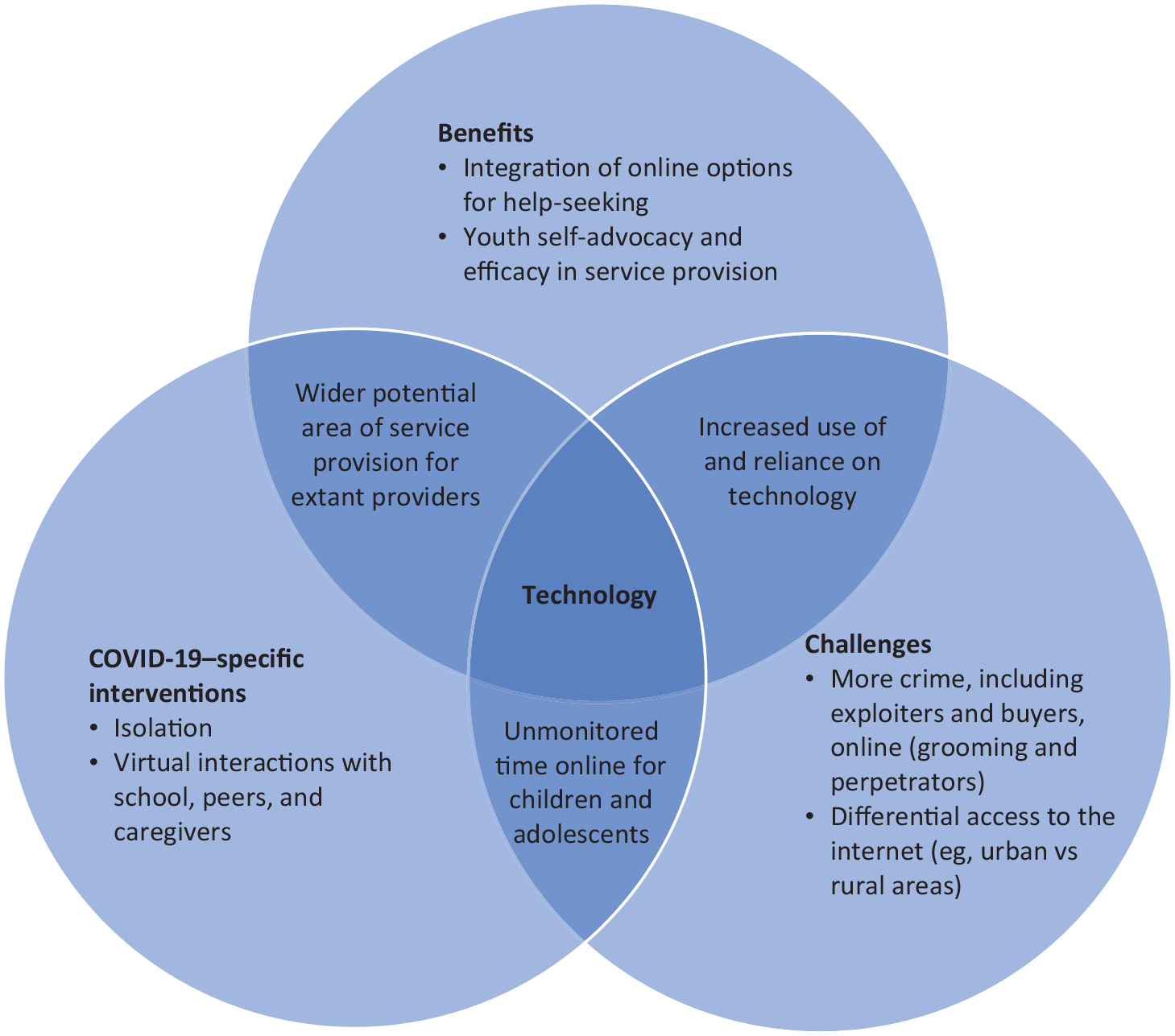
Interrelated findings related to COVID-19 and child sex trafficking victimization trajectories.
Online CST Grooming and Victimization
Before the pandemic, concerns were growing as online opportunities for CST grooming and perpetration were expanding. 17 However, our results indicate that the pandemic increased the immediacy for law enforcement, CST prevention agencies, child advocacy centers, and service agencies to ensure that their identification protocols and assistance reflected current victimization trajectories. This result is consistent with what is known about online activities more broadly throughout the COVID-19 pandemic. 18 Stay-at-home recommendations or requirements of varying lengths and intensities affected up to 88.6% of the country. 19 Many individuals were laid off or moved to remote work, expanding free time and time for potential groomers and exploiters to explore online. Young people also were kept out of school, with few options for social connection or entertainment other than being online and few opportunities to escape familial offenders.7,18
As a result, the pandemic may have expanded the potential for exploiters and perpetrators of CST to connect with young people at risk for CST victimization. Although information on rates and trends in CST victimization is still limited, thereby restricting our ability to analyze trends, available data suggest that rates of CST may have increased during the pandemic. 20 A particular concern is that as the effects of the pandemic lessen and activities continue to return to a prepandemic status, the markets and opportunities that developed online for CST victimization may remain.
Expansion of Online Treatment and Services
Assessing the effect of the pandemic on CST services is complex. On one hand, the pandemic restricted many services and made them harder for victims to access. For example, the movement of services to online forums may have created difficulties for young people without technology or online access. Additionally, evidence suggests that for young people—particularly those at risk for CST victimization—the pandemic exacerbated mental health concerns, placing a strain on mental health and support service networks and resources for them. 5
On the other hand, study participants suggested that there were benefits to the creation of remote or online services. Given that young people may not have access to transportation, the expansion of online services allowed service providers an opportunity to engage with young people to whom they may not have previously had access, including those in remote locations or with limited family supports. Furthermore, telehealth services allow young people to engage with service providers in ways that facilitate help-seeking while providing options for intensity (eg, audio only vs audio and video, text help lines, individual and family therapy). Data suggest that most young people (97%) have access to smartphones. 21 Accordingly, remote and online services provide young people with the opportunity to advocate for their own needs and actively choose their own paths to recovery.
Strengths and Limitations
A strength of the current study is that it provides in-depth information from a diverse group of professionals working with young people affected by CST from across the United States. The study also had several limitations. First, it was limited in generalizability and may not accurately represent all professional experiences of those working with young people affected by CST in the United States. Second, the current study provides cross-sectional data that preclude causal or time-ordered analyses. Participants were asked to reflect on their experiences from pre- to postpandemic, which may have been inaccurate or otherwise biased. Given the semistructured nature of the interview guide, some viewpoints may have been underrepresented.
Conclusions
Our findings underscore the reality that professionals working with young people affected by CST are still working to fully understand and respond to changes in CST victimization trajectories related to the COVID-19 pandemic. Technology’s role in CST victim trajectories is a doubled-edged sword. Given the rapidity of technology’s growth, perpetrators will find ways to use technology to hide their behaviors and evade detection from authorities. However, technology also provides ways to capture evidence that can support the prosecution of offenders and facilitate help-seeking for young people who are experiencing CST victimization/revictimization.
Our findings support the provision of training for law enforcement and those who interact with young people regularly (eg, teachers, school personnel) about online grooming, victimization, and services for CST. Such training may provide an opportunity to increase awareness of CST involving children, including children who do not fit traditional profiles of risk, such as those without histories of maltreatment, violence victimization, or housing insecurity. The flexibility showcased by service agencies during the pandemic suggests that their increased experience in providing online and remote services may increase providers’ ability to work with young populations who may be inadvertently encountering online risks. Service disruptions associated with the pandemic highlight the need for epidemiologic research so that we may definitively identify how global and national events affect young people.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241267721 – Supplemental material for COVID-19 and Child Sex Trafficking: Qualitative Insights on the Effect of the Pandemic on Victimization and Service Provision
Supplemental material, sj-docx-1-phr-10.1177_00333549241267721 for COVID-19 and Child Sex Trafficking: Qualitative Insights on the Effect of the Pandemic on Victimization and Service Provision by Jennifer E. O’Brien, Lisa M. Jones, Kimberly J. Mitchell and Gina Zwerling Kahn in Public Health Reports
Footnotes
Acknowledgements
The authors thank all of the study participants for their time and willingness to share their experiences with us, as well as the service providers and law enforcement across the United States who engage in this difficult work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Justice (grant 2020-MU-CX-0041).
Disclaimer
The research presented in this article is that of the authors and does not reflect the official policy of the US Department of Justice.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.