
Abstract
Objective:
People who inject drugs are a population who are often unengaged with health care services. The objective of this study was to characterize COVID-19 vaccine hesitancy and uptake in a community-based sample of people who inject drugs in Baltimore, Maryland.
Methods:
The ALIVE study (AIDS Linked to the IntraVenous Experience) in Baltimore is a community-based cohort study of people with a history of injection drug use. From March 2 through June 28, 2021, 346 ALIVE participants completed a survey on substance use, structural determinants of health, and COVID-19 vaccine hesitancy. The exposure of interest was COVID-19 vaccine hesitancy, and the primary outcome was vaccination status as of June 30, 2021. We extracted data on the dates of vaccination from electronic medical records linked to study participants.
Results:
The median age of the sample was 60 years; most participants were male (66%) and non-Hispanic Black (87%). Most (55%) trusted the COVID-19 vaccine, and 68% had received ≥1 dose. After age standardization, survey participants were more likely than the Maryland general population to be unvaccinated (prevalence ratio = 1.20; 95% CI, 0.97-1.49; P = .10). Participants who somewhat trusted or did not trust the COVID-19 vaccine had 6-fold higher odds of being unvaccinated than participants who trusted the vaccine (odds ratio = 6.30; 95% CI, 3.74-10.60).
Conclusion:
Uptake of COVID-19 vaccine among people with a history of injection drug use was high. Attitudes and knowledge about vaccination were important predictors of vaccine uptake. Education and outreach efforts could be effective in reducing hesitancy and increasing vaccination in substance-using populations.
The COVID-19 pandemic has brought unprecedented challenges to the US health care system and, as of May 13, 2022, has resulted in >1 million deaths. 1 The pandemic and responses to it have exacerbated socioeconomic and health disparities experienced by some communities, such as people who inject drugs (PWID). Harm reduction programs have been shown to prevent HIV transmission, hepatitis C virus transmission, and overdose.2-4 These programs have been restricted during the pandemic, which may have reduced access to services, including receiving tailored and credible vaccine information. 5 Finally, PWID often have numerous chronic comorbidities, 6 which are risk factors for developing severe COVID-19. 7
As of February 2022, the US Food and Drug Administration had granted Emergency Use Authorization for 1 COVID-19 vaccine and approved 2 COVID-19 vaccines for people aged ≥16 years and ≥18 years (depending on the vaccine). 8 Despite availability of these vaccines, as of May 2022, approximately one-third of adults in the United States had not yet been fully vaccinated, and nearly 20% indicated that they would “probably or definitely not” receive the COVID-19 vaccine. 9 Additionally, people who use illicit drugs in the United States reported high rates of unwillingness to receive a COVID-19 vaccine.10,11 Approximately one-third of PWID in San Diego, California, and Tijuana, Mexico, were hesitant to receive the vaccine, with most endorsing ≥1 COVID-19–related conspiracy theory. 12 Despite the high prevalence of comorbidities and elevated risk for severe illness and death from COVID-19 among PWID, to our knowledge, no studies have investigated attitudes about vaccination and vaccine uptake in this population after vaccines became widely available in the United States.
Our primary objective was to characterize COVID-19 vaccine uptake and hesitancy in a cohort of former and current PWID and examine which sociodemographic factors were associated with these outcomes. A secondary objective was to examine the association between vaccine hesitancy and vaccination status and evaluate which sociodemographic factors were associated with remaining unvaccinated among those with a high level of hesitancy.
Methods
Study Population and Data Collection
We collected data from participants enrolled in the ALIVE study (AIDS Linked to the IntraVenous Experience), a community-recruited cohort of former and current PWID living in or near Baltimore, Maryland. 13 Study eligibility criteria included age ≥18 years and a history of injecting drugs in the past 5 years. Enrollment began in 1988, with additional recruitment occurring in 1994-1995, 1998, and 2000 and during 2005-2008 and 2015-2018. Prior to the COVID-19 pandemic, study participants twice annually visited a research clinic with individual interview rooms, a blood draw station, and an area to perform functional assessments and measure vital statistics. Study participants completed an interview on substance use behaviors, comorbidities, and health care use and provided blood samples for laboratory testing. We also obtained consent for release and review of their medical records.
Of 1240 participants in active follow-up since January 1, 2018, the study interviewers contacted 532 and reached 443 by telephone. Because of the COVID-19 pandemic, in-person visits at the clinic were suspended on March 13, 2020, thereby requiring staff to contact participants by telephone. People who were reached were more likely than those not reached to be older (vs younger), non-Hispanic Black (vs non-Hispanic White), and living with HIV (vs not) and less likely to have experienced homelessness (vs not). 5 From March 2 through June 28, 2021, 367 participants completed an interviewer-administered rapid assessment on COVID-19 vaccine hesitancy by telephone. Of these, 346 (94%) provided data on all relevant covariates and were included in this analysis. The Johns Hopkins Bloomberg School of Public Health Institutional Review Board approved all study procedures, and all participants consented to both in-person and telephone-based surveys.
Measures
Vaccination status
We manually extracted data on dates of vaccination from participants’ medical records in the Chesapeake Regional Information System for Our Patients (CRISP). 14 CRISP is a health information exchange that shares electronic medical record data across Maryland and documents all clinical encounters with participating health care providers. We located all 346 (100%) participants who had complete covariate data and completed the COVID-19 survey in CRISP by using that platform’s probabilistic matching algorithm based on name and date of birth. COVID-19 vaccination status was indicated for each patient in CRISP based on data from the Maryland Department of Health’s vaccine surveillance system. Therefore, we regarded CRISP as the gold standard source for vaccination status in Maryland. We collected data on vaccination status (none vs ≥1 dose) as of June 30, 2021. On April 27, 2021, vaccines became available for all people aged ≥16 years in Maryland. 15 The COVID-19 incidence rate in Baltimore City on that date was 27.79 cases per 100 000 population, a decline from 2 weeks earlier (44.68 cases per 100 000 population). 16 COVID-19 incidence further declined by the end of the observation period (June 30, 2021) to 0.64 cases per 100 000 population.
Vaccine hesitancy
We adapted Quinn and colleagues’ measures for influenza vaccine hesitancy, confidence, and trust to measures for COVID-19. 17 The scale consisted of 7 items. The first question asked, “Overall, how much do you trust the COVID-19 vaccine?” and was measured on a 5-point Likert scale (1 = completely, 2 = moderate, 3 = somewhat/neutral, 4 = slightly, 5 = not at all). Six additional questions were measured on a 4-point Likert scale (1 = very much, 2 = mostly, 3 = somewhat, 4 = not at all) and were phrased as “Thinking specifically about the COVID-19 vaccine, do you think the COVID-19 vaccine is . . .” (1) necessary? (2) important? (3) safe? (4) effective? (5) convenient? and (6) affordable? In addition to analyzing responses individually, we summed the responses to create a continuous score for which a 1-unit increase indicates greater hesitancy and lower trust and confidence; this score could range from 7 to 29. We defined hesitancy as a score ≥16. “Don’t know” responses were coded at the midpoint (eg, 3 on a 1-5 scale) of the Likert scale for each item.
Other covariates
We obtained all data on covariates from the interviewer-administered survey. We assessed covariates that could have been independently associated with vaccine hesitancy or being unvaccinated, such as sociodemographic characteristics: age per 5-year increment, race (Black/non-Black [Hispanic and non-Hispanic]), sex (male/female), and structural determinants (homelessness [yes/no] and incarceration [yes/no] in the past 6 months). We classified alcohol use disorder (none, harmful/hazardous, severe/dependent) by using the first 3 items in the Alcohol Use Disorders Identification Test, 18 and we assessed marijuana use, noninjection illicit drug use (cocaine, heroin, fentanyl, methamphetamine, painkillers, sedatives, tranquilizers, hallucinogens, other stimulants, and other drugs), and injection drug use in the past 6 months. We determined HIV serostatus (positive, negative) by detection of HIV-1 antibodies using an enzyme-linked immunosorbent assay with confirmation by Western blot. Receipt of the influenza vaccine in the past 12 months (yes/no) was based on self-report. Number of self-reported comorbidities (0 or 1, 2, ≥3) was based on whether a health care provider had ever told the participants that they had hypertension, diabetes, kidney disease, chronic obstructive pulmonary disease/lung disease, cardiovascular disease, stroke, cancer, or obesity.
Statistical Analysis
To compare uptake of the COVID-19 vaccine among participants in the ALIVE study with the Maryland general population, we applied age standardization. We obtained data on vaccination rates among the Maryland general population for each age group (18-49, 50-64, ≥65 y) from the Maryland Department of Health 19 and 2020 population sizes for each age stratum from the Maryland Department of Planning. 20 We then calculated the age-specific prevalence of COVID-19 vaccination among participants in the ALIVE study and in the Maryland general population. To calculate the age-adjusted rate, we took a weighted average of strata using the US general population age distribution for reference weights. 21 We calculated the age-standardized prevalence and prevalence ratios that compared COVID-19 vaccination rates among participants in the ALIVE study with rates among the Maryland general population.
We combined the vaccine hesitancy scale into “very much/mostly,” “somewhat/not at all,” and “don’t know” and calculated the prevalence of each response for each question in the cohort. We then estimated the crude odds ratios (ORs) for the association of each hesitancy response with being unvaccinated, using the least hesitant group as the referent.
We divided the hesitancy score into quartiles and calculated the prevalence of being in the top quartile for the self-reported vaccine hesitancy score (ie, the most hesitant). The top quartile consisted of scores ≥16, indicating a high level of vaccine hesitancy. We used logistic regression to estimate the crude and adjusted ORs (aORs) for the association of each characteristic with hesitancy. In multivariable analysis, all models included sex, race, and age, but we also conducted selection of nondemographic covariates by identifying the set of covariates that minimized the Akaike information criterion. Next, we modeled the association between each sociodemographic and behavioral covariate and being unvaccinated. Finally, in a subanalysis among those in the top quartile of vaccine hesitancy (n = 85), we assessed sociodemographic and behavioral factors associated with vaccination.
We conducted 2 sensitivity analyses. First, we repeated the logistic regression of top-quartile vaccine hesitancy on hypothesized risk factors, but we recoded “don’t know” responses to be at the highest end of the scale (ie, most hesitant, least confident). Second, we repeated the logistic regression of top-quartile vaccine hesitancy on hypothesized risk factors, but we included all covariates in the adjusted model.
We considered P < .05 to be significant. Hypotheses were not preregistered, and results should be considered exploratory. We conducted all statistical analyses in SAS version 9.4 (SAS Institute Inc).
Results
Of 346 survey participants, 66% (n = 228) were male, 87% (n = 302) were Black, and the median age was 60 (interquartile range, 55-66) years. Thirty-one percent (n = 107) had HIV. One-quarter of the sample (n = 88) had used an illicit drug other than marijuana in the past month. The median vaccine hesitancy score was 10.5 (range [interquartile range], 7-29 [8-16]), with strong internal consistency (Cronbach α = 0.88). For each item in the vaccine hesitancy questionnaire, most survey participants (55%) indicated that they “very much” or “mostly” trusted the COVID-19 vaccine. The response “don’t know” was common: >20% responded “don’t know” for the question “Do you think it is effective?” Nearly one-third (n = 110) had not received any doses of the COVID-19 vaccine. Only 3% (n = 11) received the 1-dose vaccine, while 65% (n = 225) received the 2-dose vaccine.
Age-specific COVID-19 vaccination rates were consistently lower among participants in the ALIVE study than among the Maryland general population. Thus, when the proportion unvaccinated was compared between the ALIVE study and the Maryland general population, the resulting prevalence ratios were >1; however, none were significant (Figure). The directly standardized estimates per 1000 population were 595 (95% CI, 467-723) vaccinations among participants in the ALIVE study and 713 (95% CI, 712-714) among the Maryland general population. After standardization, participants in the ALIVE study were 20% more likely than the Maryland general population to be unvaccinated (prevalence ratio = 1.20; 95% CI, 0.97-1.49; P = .10).
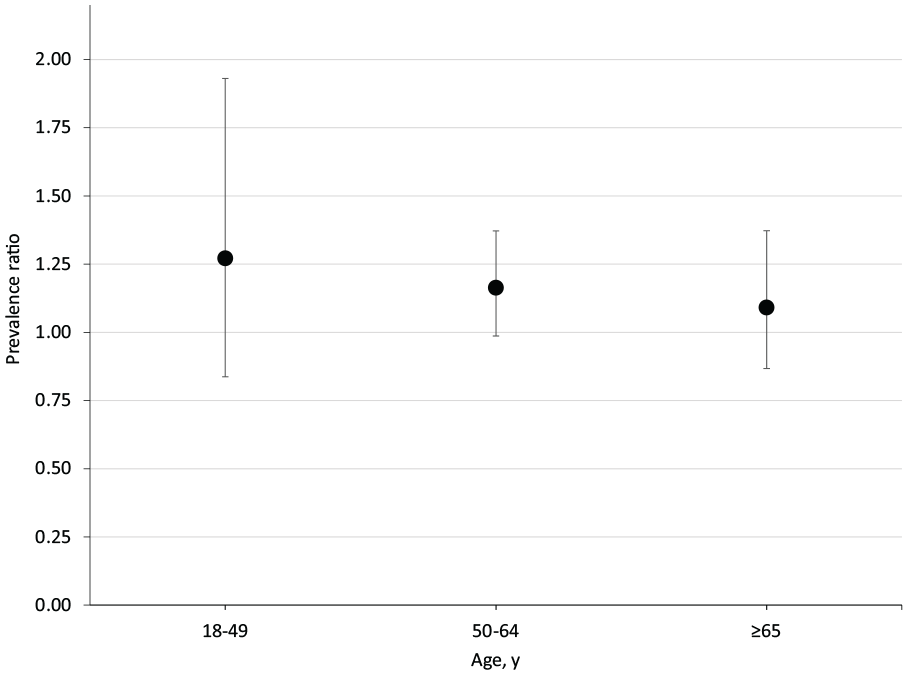
Stratum-specific prevalence ratios that compare the proportion of unvaccinated people in the ALIVE study (AIDS Linked to the IntraVenous Experience) in Baltimore, Maryland, with the proportion of unvaccinated people in the general population of Maryland (referent), March–June 2021. Error bars indicate 95% CIs. Data sources: Maryland Department of Health 19 and Maryland Department of Planning. 20
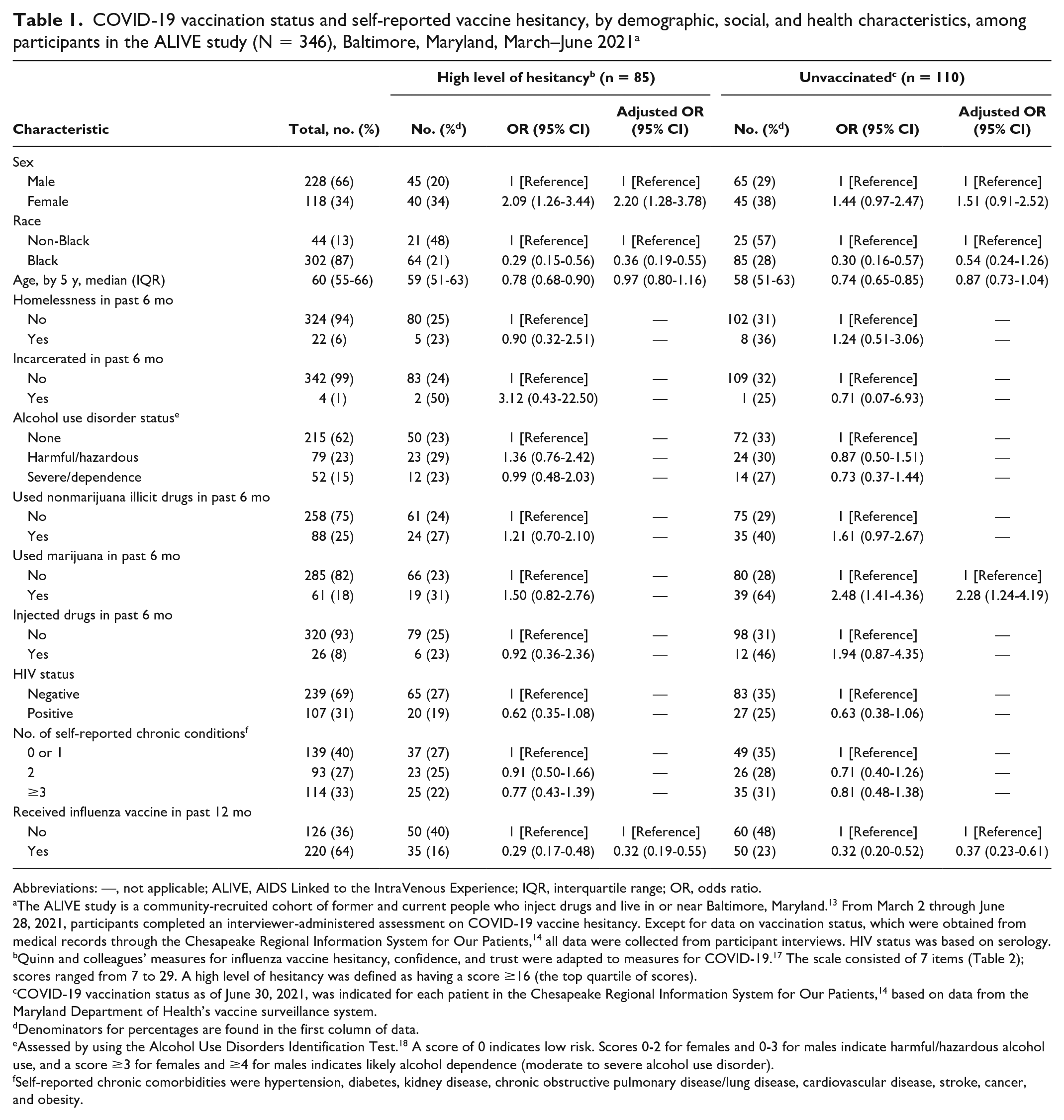
Among participants in the ALIVE study, female participants were significantly more likely than male participants (OR = 2.09 [95% CI, 1.26-3.44]; aOR = 2.20 [95% CI, 1.28-3.78]) to be in the top quartile of vaccine hesitancy in crude and adjusted analyses (Table 1). Black participants were significantly less likely than non-Black participants (OR = 0.29 [95% CI, 0.15-0.56]; aOR = 0.36 [95% CI, 0.19-0.55]) to be vaccine hesitant. Older age (OR per 5-year increase = 0.78 [95% CI, 0.68-0.90]) was significantly associated with lower levels of hesitancy in the crude analysis but not in the adjusted analysis. Participants who received an influenza vaccine in the past 12 months were significantly less likely than participants who did not receive an influenza vaccine to be vaccine hesitant (OR = 0.29 [95% CI, 0.17-0.48]; aOR = 0.32 [95% CI, 0.19-0.55]).
COVID-19 vaccination status and self-reported vaccine hesitancy, by demographic, social, and health characteristics, among participants in the ALIVE study (N = 346), Baltimore, Maryland, March–June 2021 a
Abbreviations: —, not applicable; ALIVE, AIDS Linked to the IntraVenous Experience; IQR, interquartile range; OR, odds ratio.
The ALIVE study is a community-recruited cohort of former and current people who inject drugs and live in or near Baltimore, Maryland. 13 From March 2 through June 28, 2021, participants completed an interviewer-administered assessment on COVID-19 vaccine hesitancy. Except for data on vaccination status, which were obtained from medical records through the Chesapeake Regional Information System for Our Patients, 14 all data were collected from participant interviews. HIV status was based on serology.
Quinn and colleagues’ measures for influenza vaccine hesitancy, confidence, and trust were adapted to measures for COVID-19. 17 The scale consisted of 7 items (Table 2); scores ranged from 7 to 29. A high level of hesitancy was defined as having a score ≥16 (the top quartile of scores).
COVID-19 vaccination status as of June 30, 2021, was indicated for each patient in the Chesapeake Regional Information System for Our Patients, 14 based on data from the Maryland Department of Health’s vaccine surveillance system.
Denominators for percentages are found in the first column of data.
Assessed by using the Alcohol Use Disorders Identification Test. 18 A score of 0 indicates low risk. Scores 0-2 for females and 0-3 for males indicate harmful/hazardous alcohol use, and a score ≥3 for females and ≥4 for males indicates likely alcohol dependence (moderate to severe alcohol use disorder).
Self-reported chronic comorbidities were hypertension, diabetes, kidney disease, chronic obstructive pulmonary disease/lung disease, cardiovascular disease, stroke, cancer, and obesity.
Among participants in the ALIVE study, in the crude analysis (but not the adjusted analysis), Black participants were significantly less likely than non-Black participants to be unvaccinated (OR = 0.30 [95% CI, 0.16-0.57]). Furthermore, marijuana use in the past 6 months as compared with no marijuana use was associated with increased odds of being unvaccinated (OR = 2.48 [95% CI, 1.41-4.36]; aOR = 2.28 [95% CI, 1.24-4.19]). Receiving an influenza vaccine in the past 12 months was strongly associated with lower odds of being unvaccinated (OR = 0.32 [95% CI, 0.20-0.52]; aOR = 0.37 [95% CI, 0.22-0.61]).
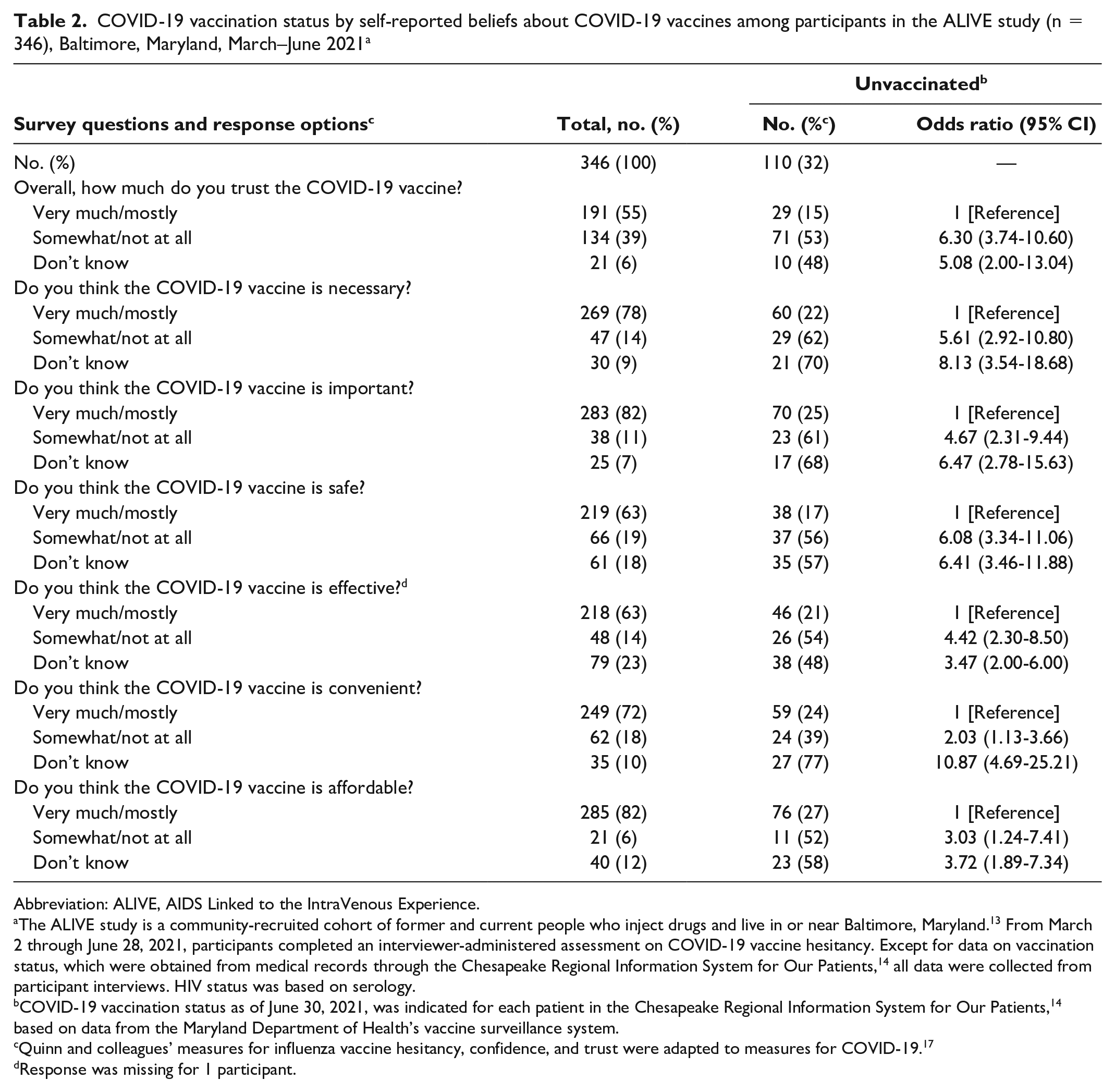
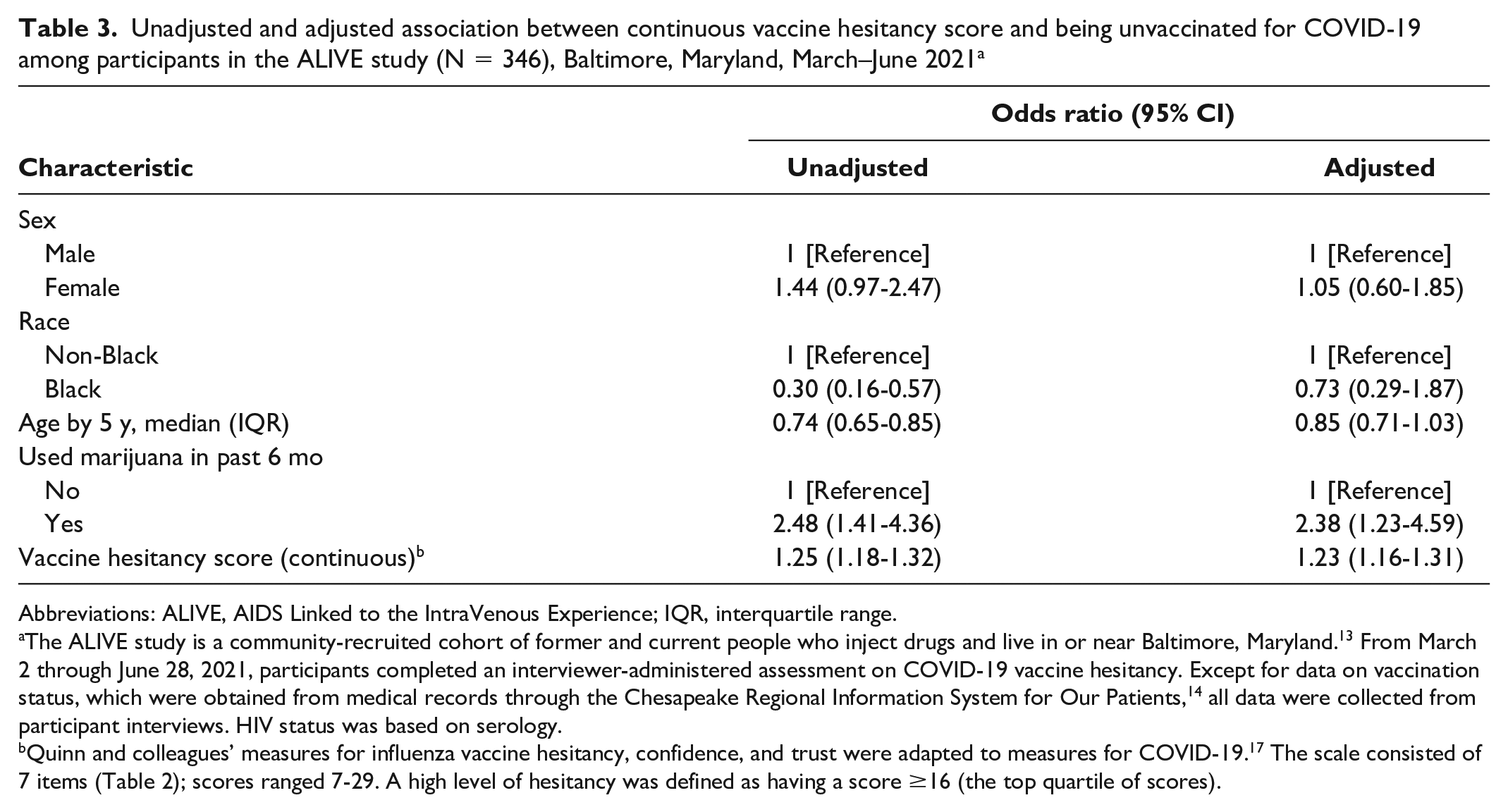
Hesitant responses were strongly associated with increased odds of being unvaccinated, ranging from “How much do you trust [the vaccine]?” (OR = 6.30 [95% CI, 3.74-10.60]) to “Do you think the COVID-19 vaccine is convenient?” (OR = 2.03 [95% CI, 1.13-3.66]) (Table 2). “Don’t know” responses were also strongly associated with being unvaccinated. When vaccine hesitancy was considered a continuous measure, a 1-unit increase in the scale was associated with 23% (aOR = 1.23 [95% CI, 1.16-1.31]) higher odds of being unvaccinated (Table 3).
COVID-19 vaccination status by self-reported beliefs about COVID-19 vaccines among participants in the ALIVE study (n = 346), Baltimore, Maryland, March–June 2021 a
Abbreviation: ALIVE, AIDS Linked to the IntraVenous Experience.
The ALIVE study is a community-recruited cohort of former and current people who inject drugs and live in or near Baltimore, Maryland. 13 From March 2 through June 28, 2021, participants completed an interviewer-administered assessment on COVID-19 vaccine hesitancy. Except for data on vaccination status, which were obtained from medical records through the Chesapeake Regional Information System for Our Patients, 14 all data were collected from participant interviews. HIV status was based on serology.
COVID-19 vaccination status as of June 30, 2021, was indicated for each patient in the Chesapeake Regional Information System for Our Patients, 14 based on data from the Maryland Department of Health’s vaccine surveillance system.
Quinn and colleagues’ measures for influenza vaccine hesitancy, confidence, and trust were adapted to measures for COVID-19. 17
Response was missing for 1 participant.
Unadjusted and adjusted association between continuous vaccine hesitancy score and being unvaccinated for COVID-19 among participants in the ALIVE study (N = 346), Baltimore, Maryland, March–June 2021 a
Abbreviations: ALIVE, AIDS Linked to the IntraVenous Experience; IQR, interquartile range.
The ALIVE study is a community-recruited cohort of former and current people who inject drugs and live in or near Baltimore, Maryland. 13 From March 2 through June 28, 2021, participants completed an interviewer-administered assessment on COVID-19 vaccine hesitancy. Except for data on vaccination status, which were obtained from medical records through the Chesapeake Regional Information System for Our Patients, 14 all data were collected from participant interviews. HIV status was based on serology.
In the subanalysis among participants in the ALIVE study in the top quartile of vaccine hesitancy (n = 85), 58 (68%) were unvaccinated. Women (OR = 2.29 [95% CI, 0.89-5.95]) had higher odds than men of being unvaccinated, although this difference was not significant (Table 4). However, increasing age per 5-year increment was associated with significantly higher odds of being unvaccinated (OR = 1.35 [95% CI, 1.17-1.54]). Furthermore, participants who were living with HIV were significantly less likely than participants without HIV to have been unvaccinated (OR = 0.35 [95% CI, 0.13-1.00]; P = .0497).
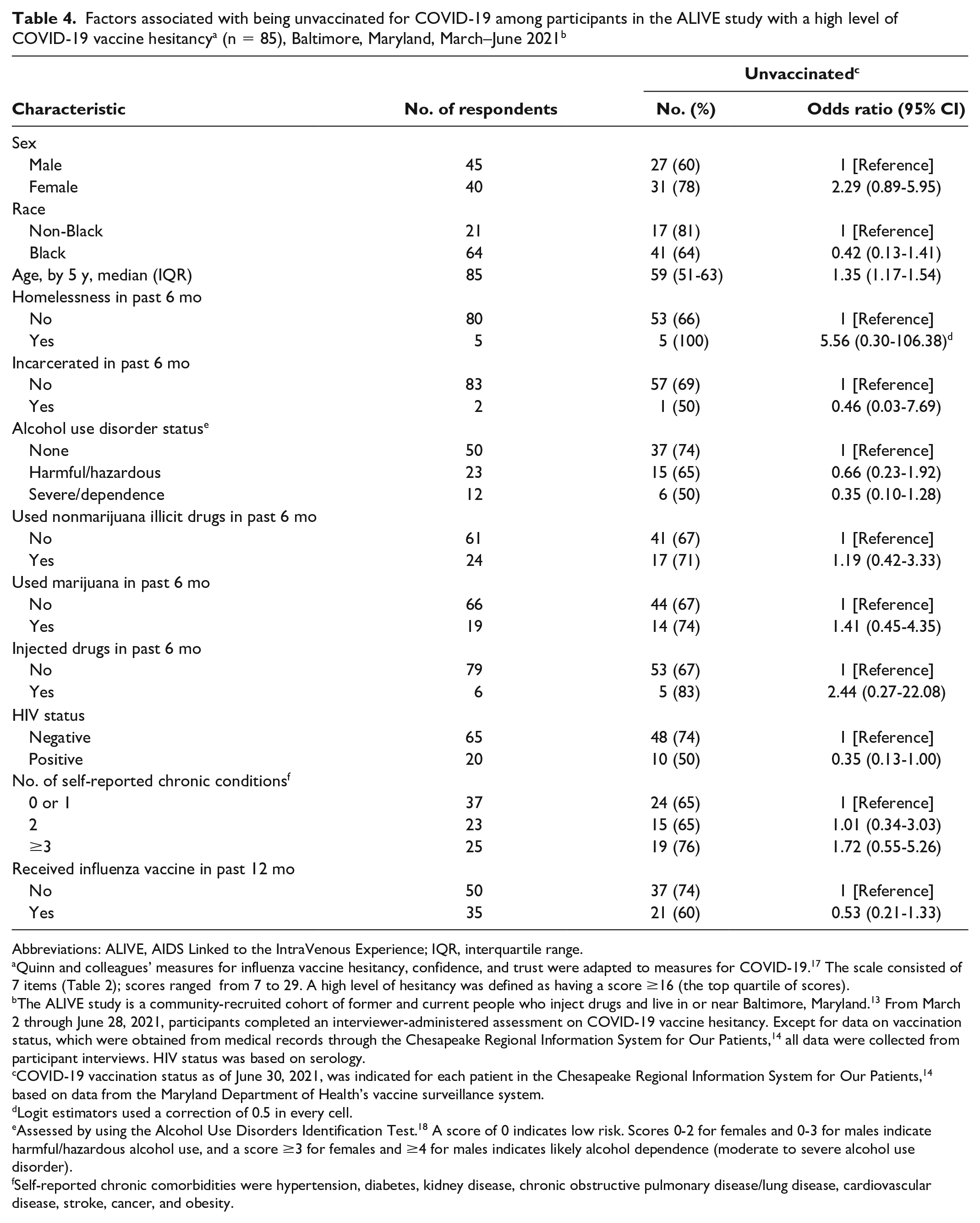
Abbreviations: ALIVE, AIDS Linked to the IntraVenous Experience; IQR, interquartile range.
Quinn and colleagues’ measures for influenza vaccine hesitancy, confidence, and trust were adapted to measures for COVID-19. 17 The scale consisted of 7 items (Table 2); scores ranged from 7 to 29. A high level of hesitancy was defined as having a score ≥16 (the top quartile of scores).
The ALIVE study is a community-recruited cohort of former and current people who inject drugs and live in or near Baltimore, Maryland. 13 From March 2 through June 28, 2021, participants completed an interviewer-administered assessment on COVID-19 vaccine hesitancy. Except for data on vaccination status, which were obtained from medical records through the Chesapeake Regional Information System for Our Patients, 14 all data were collected from participant interviews. HIV status was based on serology.
COVID-19 vaccination status as of June 30, 2021, was indicated for each patient in the Chesapeake Regional Information System for Our Patients, 14 based on data from the Maryland Department of Health’s vaccine surveillance system.
Logit estimators used a correction of 0.5 in every cell.
Assessed by using the Alcohol Use Disorders Identification Test. 18 A score of 0 indicates low risk. Scores 0-2 for females and 0-3 for males indicate harmful/hazardous alcohol use, and a score ≥3 for females and ≥4 for males indicates likely alcohol dependence (moderate to severe alcohol use disorder).
Self-reported chronic comorbidities were hypertension, diabetes, kidney disease, chronic obstructive pulmonary disease/lung disease, cardiovascular disease, stroke, cancer, and obesity.
We did not detect any substantial differences in the relative measures of association between vaccine hesitancy measures and vaccination after recoding the “don’t know” responses to reflect greater hesitancy. The characteristics associated with being vaccinated and vaccine hesitancy in multivariable models were similar to those shown in the main analysis when no model selection was conducted.
Discussion
To our knowledge, our analysis is among the first to describe COVID-19 vaccination status in a community-based sample of PWID in the United States. As of June 30, 2021, 68% of the sample had received ≥1 dose of COVID-19 vaccine, which was a larger proportion than in the Maryland general population on this date (62%); however, some disparities remain. 18 In particular, ALIVE participants on average are older than the general population. After age standardization, ALIVE participants were 20% more likely than the Maryland general population to be unvaccinated, although this finding was not significant. Nonetheless, these data are reassuring, particularly because data from other substance-using cohorts have suggested low levels of intention to be vaccinated.10,12 In sum, our findings suggest that efforts to vaccinate all adults in Maryland were generally effective for the PWID population.
A key strength of this study was the use of electronic medical record data from the gold standard state vaccination surveillance system data reported in the Maryland health information exchange to determine vaccination status. As expected, people with higher levels of vaccine hesitancy were less likely to be vaccinated against COVID-19. Furthermore, responding “I don’t know” to questions about trust in the COVID-19 vaccine was strongly associated with being unvaccinated, suggesting that lack of knowledge about the vaccine or uncertainty about vaccine information could delay vaccination. Indeed, nearly half of the sample did not trust the vaccine or did not know if it could trust the vaccine, and more than one-third doubted its effectiveness or did not know that it was effective. The implications of characterizing people who indicated that they “don’t know” about the safety and effectiveness of the vaccines are important because they could be more receptive to educational interventions than people who expressed definitive hesitancy.
The only factor that was strongly and significantly associated with reduced odds of high levels of vaccine hesitancy and being unvaccinated was self-reported receipt of the influenza vaccine in the past year. This finding suggests that attitudes about vaccination may be more important than other social or economic characteristics for determining vaccine uptake. Conversely, alcohol use disorder, illicit drug use other than marijuana, and injection drug use were not significantly associated with high levels of vaccine hesitancy or being unvaccinated. These findings are consistent with a study among US adults who used tobacco and marijuana that found no association between COVID-19 vaccine hesitancy and substance-using behaviors. 11 Marijuana use was not associated with hesitancy; however, it was associated with being unvaccinated. Although further research is needed, marijuana use could reduce the likelihood of health-seeking behaviors, such as vaccination. 22 Other factors associated with reduced odds of vaccination included non-Black race and younger age. The former is interesting because it differs from vaccination rates in the Maryland general population, where Black residents are less likely than White residents to be vaccinated. 23 The latter finding is consistent with vaccination uptake in the general US population, where people aged <55 (vs ≥55) years were less accepting of the vaccine. 24 Thus, the groups identified in our analysis may be appropriate for enhanced outreach by health care organizations serving people who use illicit drugs.
Some participants who expressed high levels of unvaccinated hesitancy were still vaccinated as of June 30, 2021. Among those with high levels of vaccine hesitancy, HIV positivity was associated with being vaccinated. This could be due to people living with HIV receiving their primary care from HIV specialists who could assuage concerns given their potential immunocompromised status. For many people with HIV, distrust in the health care system may be compensated by trust in their health care provider. Health care provider constancy (seeing the same provider at 90% of HIV clinic visits) is one of the strongest factors in avoiding lapses in HIV care and maintaining viral suppression. 25 People without HIV have fewer stable primary care opportunities than people with HIV; however, more research is warranted to understand the role of HIV, hesitancy, and vaccination status.
Limitations
Our study had several limitations. First, participants completed this survey after the emergence of COVID-19 and are not representative of the entire cohort. Only about one-quarter of survey participants reported recent drug use, which is less than prepandemic levels of reported substance use. Thus, our sample overrepresented people who were likely to be stable (ie, had no recent illicit drug use), and vaccination rates are likely lower among participants who we were not able to reach by telephone (vs those we could reach). Second, the ALIVE study represents a cohort of older, primarily Black people who reside in Baltimore and may not be generalizable to other substance-using populations in the United States. Third, because vaccine hesitancy can change over time and because our study was cross-sectional, we do not know which factors could be associated with a shift from hesitancy toward trust. Results reflect vaccine coverage as of June 30, 2021, and hesitant people could have been subsequently vaccinated, especially given vaccination mandates and greater awareness of more transmissible or more virulent variants of SARS-CoV-2.
Conclusion
Vaccination rates in our study cohort were higher than in the Maryland general population but lower than among similarly aged adults, indicating that residual barriers remain. Risk factors for being unvaccinated were self-reported hesitancy and lack of knowledge about vaccines or uncertainty about vaccine information. Furthermore, the primary protective factor against being unvaccinated was self-reported history of receiving the influenza vaccine. By contrast, excluding marijuana, illicit drug use was not associated with reduced vaccine uptake. Health care organizations serving people who use drugs may help increase uptake among those who are not yet vaccinated (1) by proactively educating clients about COVID-19 vaccines and their benefits and addressing falsely held negative beliefs and (2) by using approaches shown to be helpful to people from socially or economically marginalized communities who mistrust vaccine information.
Footnotes
Acknowledgements
The authors thank all participants in the ALIVE study for their contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the National Institute on Drug Abuse (U01-DA-036297 [G.D.K., S.H.M.], R01-DA-053136 [B.L.G.], and K01-DA-043421 [J.A.C.]). G.D.K. was supported by funding from the National Institute of Allergy and Infectious Diseases (K24-AI118591). This publication resulted in part from research supported by the Johns Hopkins University Center for AIDS Research, a National Institutes of Health (NIH)–funded program (1P30-AI-094189), which is supported by the following NIH cofunding and participating institutes and centers: National Institute of Allergy and Infectious Diseases; National Cancer Institute; Eunice Kennedy Shriver National Institute of Child Health and Human Development; National Heart, Lung, and Blood Institute; National Institute on Drug Abuse; National Institute on Aging; National Institute of General Medical Sciences; National Institute of Diabetes and Digestive and Kidney Diseases; and National Institute on Minority Health and Health Disparities. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the article.