
Abstract

Keywords
Public Health Reports (PHR) is the official journal of the Office of the Surgeon General and the US Public Health Service. Published continuously since 1878, it is one of the oldest scholarly public health journals in the United States. It shares a common ancestral publication with the Centers for Disease Control and Prevention’s (CDC’s) Morbidity and Mortality Weekly Report. 1 PHR is a vital part of the US public health publishing field, filling a content niche at the intersection of public health research, practice, policy, training, and federal perspectives.
Publishing research results in the right journal is crucial for maximizing the impact of research. When choosing a submission venue, authors consider such characteristics as the thematic fit with their work, the publisher’s estimated turnaround time, and acceptance rates. Although some journals are beginning to report such metrics to the public, 2,3 others, including PHR, have not done so. A lack of such information may lead to missed publication opportunities and out-of-scope submissions. Here, we aim to fill this information gap by providing our readers with a new series of annual updates on PHR’s content and performance. This article is the first of that new series.
During 2020, PHR received 902 new submissions, including 864 for its regular bimonthly issues and 38 for the invited or sponsored supplemental issues. The journal’s 2020 acceptance rate for bimonthly peer- (or editor-) reviewed content was 17.5%; 824 total final decisions were made during 2020, including 144 acceptances and 680 rejections. These data exclude the supplements and the articles that are not peer or editor reviewed, such as Surgeon General’s Perspective articles and Executive Perspective articles (articles by US Department of Health and Human Services [HHS] officials) and any Reports and Recommendations submissions that did not undergo peer review (eg, reports from the National Vaccine Advisory Committee). However, these data do include such content as letters to the editor and responses to such letters, peer-reviewed Reports and Recommendations, and contributions to the departments of Law and the Public’s Health and From the Schools and Programs of Public Health, which are reviewed by the department’s associate editor and may undergo peer review.
Time to first decision—including decisions of accept, conditional accept, reject (before or after review), or revise and resubmit made on the original submission—is a metric that is important to authors because it indicates the journal’s suitability for time-sensitive submissions. Considering PHR’s bimonthly peer-reviewed content and applying to it the same inclusion and exclusion criteria mentioned previously, 899 first decisions were made during 2020. Excluding from the analysis 16 original submissions that were affected by a onetime disruption in the journal’s electronic submission system in January 2020 and were processed manually, the mean time to first decision was 35 days (range, 0-274 days), and the median time to first decision was 15 days (interquartile range [IQR], 9-44 days) (Table 1).
Content of volume 135 (January–December 2020) of Public Health Reports, by performance area and metric
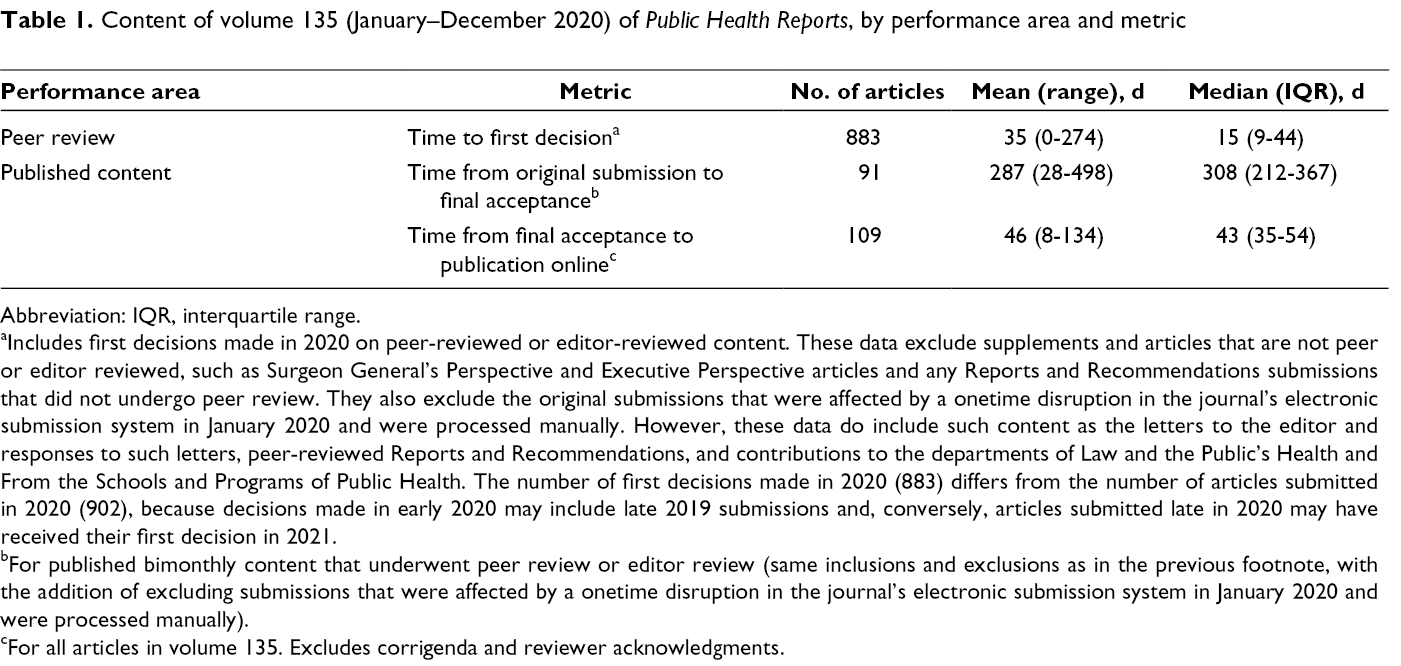
Abbreviation: IQR, interquartile range.
aIncludes first decisions made in 2020 on peer-reviewed or editor-reviewed content. These data exclude supplements and articles that are not peer or editor reviewed, such as Surgeon General’s Perspective and Executive Perspective articles and any Reports and Recommendations submissions that did not undergo peer review. They also exclude the original submissions that were affected by a onetime disruption in the journal’s electronic submission system in January 2020 and were processed manually. However, these data do include such content as the letters to the editor and responses to such letters, peer-reviewed Reports and Recommendations, and contributions to the departments of Law and the Public’s Health and From the Schools and Programs of Public Health. The number of first decisions made in 2020 (883) differs from the number of articles submitted in 2020 (902), because decisions made in early 2020 may include late 2019 submissions and, conversely, articles submitted late in 2020 may have received their first decision in 2021.
bFor published bimonthly content that underwent peer review or editor review (same inclusions and exclusions as in the previous footnote, with the addition of excluding submissions that were affected by a onetime disruption in the journal’s electronic submission system in January 2020 and were processed manually).
cFor all articles in volume 135. Excludes corrigenda and reviewer acknowledgments.
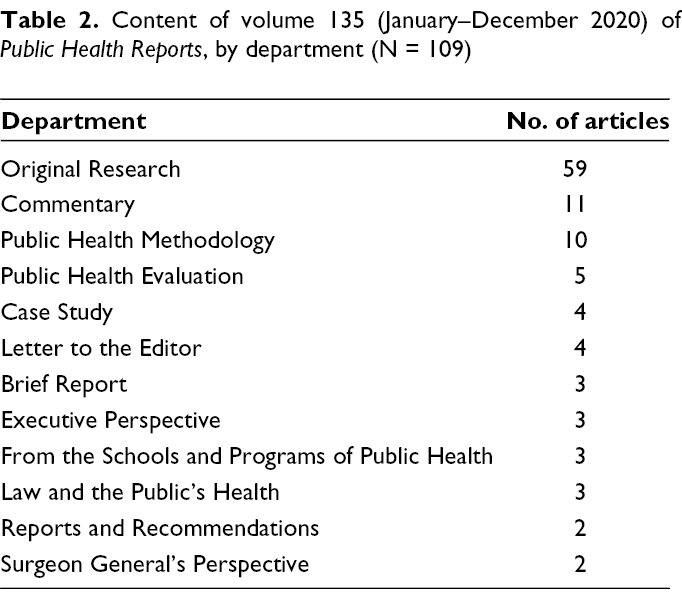
PHR published 109 articles, excluding corrigenda and reviewer acknowledgments, in volume 135 (January–December 2020): original research (59 articles), commentaries (11 articles), public health methodology (10 articles), public health evaluation (5 articles), case studies (4 articles), letters to the editor (4 articles), brief reports (3 articles), Executive Perspectives (3 articles), From the Schools and Programs of Public Health (3 articles), Law and the Public’s Health (3 articles), Reports and Recommendations (2 articles), and Surgeon General’s Perspectives (2 articles) (Table 2). Among those published articles that were reviewed (N = 91; same inclusion and exclusion criteria, excluding an additional 12 submissions that were affected by a onetime disruption in the journal’s electronic submission system in January 2020 and were processed manually), the time from original submission to final acceptance was a mean (range) of 287 (28-498) days and a median (IQR) of 308 (212-367) days (Table 1). The time from final acceptance to online publication for all 109 articles in volume 135 was a mean (range) of 46 (8-134) days and a median (IQR) of 43 (35-54) days. Analysis by department did not reveal any substantial differences in turnaround times among the article categories.
Content of volume 135 (January–December 2020) of Public Health Reports, by department (N = 109)
All but 2 corresponding authors of regular (non-supplement) articles in volume 135 were from US institutions: 1 was from the United Kingdom (Public Health England) and 1 was from Canada (University of Montreal). The 107 US authors were affiliated with academia (n = 50; 46.7%); HHS (eg, CDC, National Institutes of Health, Office of the Assistant Secretary for Health, and US Department of Agriculture) (n = 28; 26.2%); state, local, tribal, and territorial public health organizations (n = 16; 15.0%); the health care sector (n = 5; 4.7%); nonprofit organizations (n = 5; 4.7%); and private organizations (n = 3; 2.8%).
Thematically, content in volume 135 can be grouped into 11 public health topics, spanning various conditions and concerns associated with public health practice, policy, and training, as well as health disparities (Table 3). The top 3 most common topics were chronic health conditions (39 articles), infectious diseases (35 articles), and health disparities and the health of racial/ethnic minority populations and other socially or economically disadvantaged populations (29 articles).
Content of volume 135 (January–December 2020) of Public Health Reports, by topic a (N = 109)
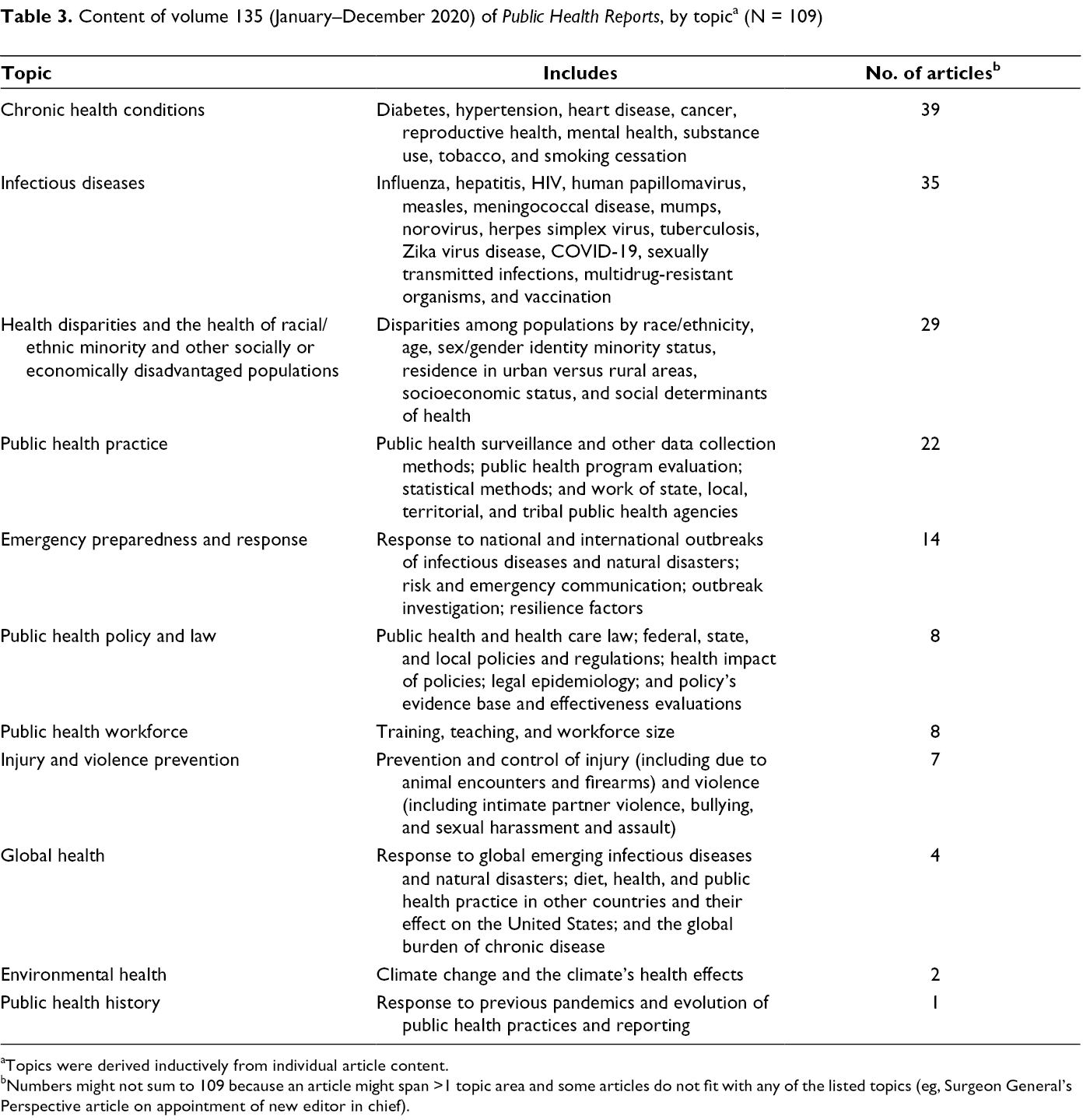
aTopics were derived inductively from individual article content.
bNumbers might not sum to 109 because an article might span >1 topic area and some articles do not fit with any of the listed topics (eg, Surgeon General’s Perspective article on appointment of new editor in chief).
Recent events brought the topic of health disparities and minority health into sharp focus. Articles on health disparities (n = 15) focused on 1 or more of the following characteristics: race/ethnicity (n = 8); socioeconomic status (n = 4); sex/gender (n = 2); rural–urban location (n = 2); and health care access, age, and educational attainment (n = 1 each). PHR also published 14 articles focusing on the health of racial/ethnic minority populations and other socially or economically disadvantaged populations, such as American Indian/Alaska Native people (n = 2), young people living in rural areas (n = 2), people with disabilities, Arab women, people engaging in risky sexual behaviors, low-income populations, a cohort of low-income multiethnic mothers, the criminal justice–involved population, non–US-born people, Arab American mothers, “high-need high-cost” patients (ie, medically and functionally impaired people who incur high health care expenses), newly arrived immigrant children, and young people who identify as lesbian, gay, bisexual, transgender, and queer or questioning (all n = 1 each). Health conditions assessed across these studies (n = 29) included maternal and child health outcomes (including child’s blood lead levels; n = 4); overall mortality (n = 3); HIV (n = 3); cancer risk, screening, and prevention (n = 3); substance use, including opioid use (n = 3); health consequences of climate change and natural disasters (n = 2); and COVID-19, influenza, cardiovascular health, preventable hospitalizations, hepatitis C, public health workforce participation, tobacco use, food insecurity, nutrition/diet quality, community-acquired pneumonia, health care delivery, and mental health (n = 1 each; 1 or more conditions per study).
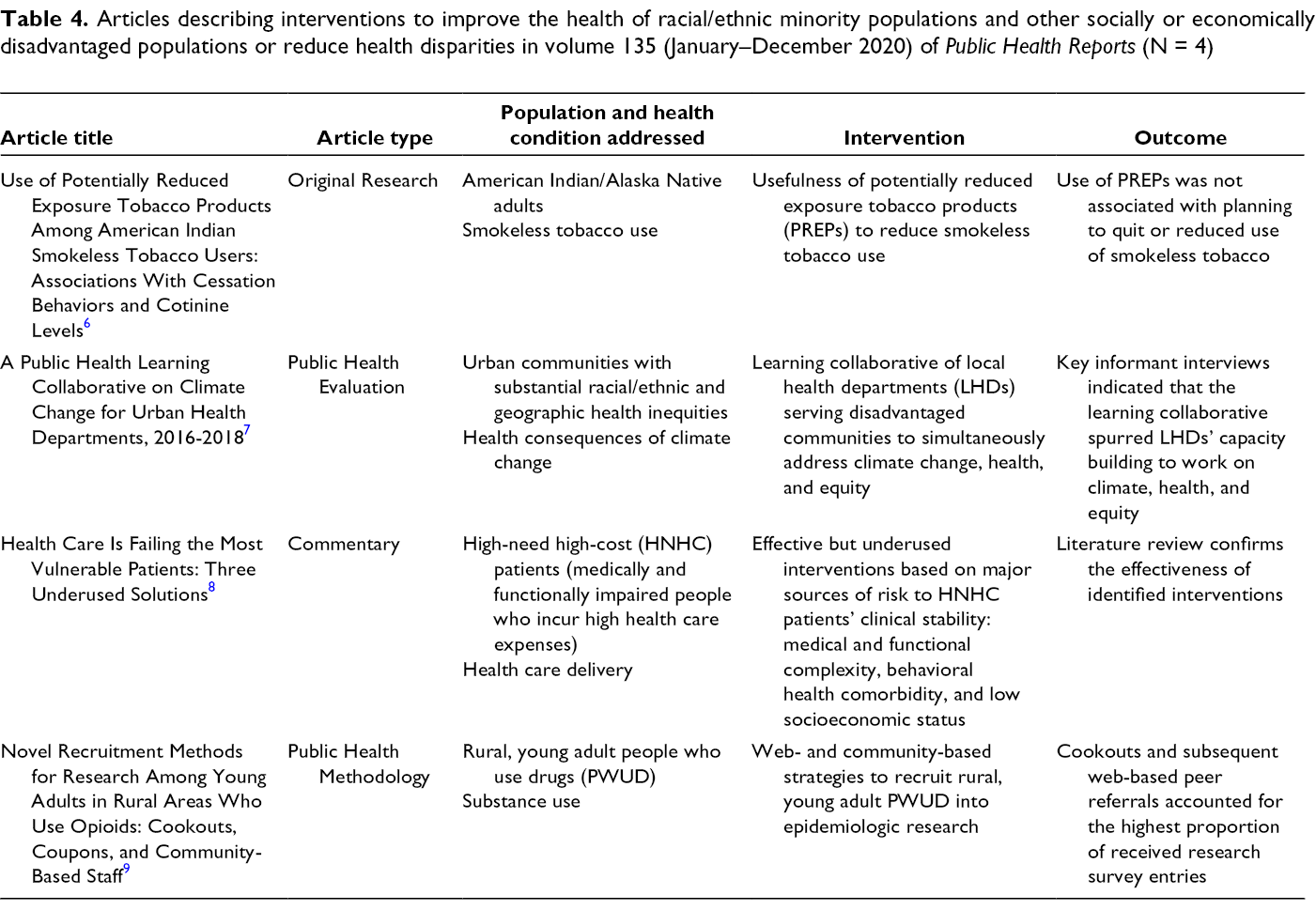
It is important to frame the scholarly discussion about reducing health disparities and improving the health of racial/ethnic minority populations and other socially or economically disadvantaged populations in terms that are fair, equitable, and inclusive, 4 and to move the discussion from an observational plane to identifying effective, practical interventions and strategies. Such interventions should target disparities not only at the individual/participant level but also at the structural (including organizational/agency) level. Interventions that focus on structural outcomes as the primary endpoint are key to adequately redressing structural racism in our health systems, prisons/jails, schools, and other institutions. 5 Four of the 29 PHR articles on health disparities and minority health addressed interventions to improve the health of racial/ethnic minority populations and other socially or economically disadvantaged populations or reduce health disparities. 6 -9 Three of these articles found interventions to be effective, 7 -9 and 1 article observed no effect 6 (Table 4). Methodologically, 2 of these studies were cross-sectional, 6,9 1 study was qualitative, 7 and 1 study was based on a review of published work. 8 None featured experimental designs. Two interventions were at the individual level, 6,9 and 2 targeted system/agency-level outcomes. 7,8 Of particular interest among these articles is a study that described novel methods of recruiting for epidemiologic research young adults living in rural areas who use opioids. 9
Articles describing interventions to improve the health of racial/ethnic minority populations and other socially or economically disadvantaged populations or reduce health disparities in volume 135 (January–December 2020) of Public Health Reports (N = 4)
On March 27, 2020, PHR issued a call for papers on the public health response to COVID-19. 10 In response, PHR received 453 original submissions and published 6 articles in 2020. Several articles were particularly noteworthy, including a commentary about the unique mental health challenges during the pandemic experienced by young people who identify as lesbian, gay, bisexual, transgender, and queer or questioning 11 ; a case study detailing lessons learned from a multiagency partnership that provides COVID-19 care for homeless people in Boston 12 ; and a historic perspective drawing parallels between San Francisco’s public health response to the 1918-1919 influenza pandemic and the city’s COVID-19 mitigation efforts. 13
During 2020, PHR published impactful articles that generated scholarly, public, and media attention, including a comparison of the racial/ethnic composition of students, graduates, and faculty at Association of Schools and Programs of Public Health–member institutions during 1996-1997 versus 2016-2017 14 and the recommendations of the National Vaccine Advisory Committee for developing an updated National Vaccine Plan. 15
During 2020, PHR also received media attention for its historic content, especially in connection with the response to the COVID-19 pandemic. An article in National Geographic about asymptomatic COVID-19 16 cites a 2009 PHR review of influenza transmission from asymptomatic infections to highlight the lack of scientific consensus on the infectiousness of silent viral cases. 17 A CNN article warning about a second wave of COVID-19 on the basis of the 1918 experience 18 cited 2 articles from PHR’s 2010 supplement comparing the 1918 and 2009 influenza pandemics—a retrospective article on the 1918 US public health measures in connection with mask-wearing and anti-spitting laws 19 and an overview of US institutional response to the 1918 pandemic as evidence of pandemics’ impact on the Army and Navy. 20 Another article from the same supplement discussing the experience of 3 US cities that kept their schools open during the 1918 influenza pandemic 21 was quoted in a 2020 Washington Post commentary discussing US school closings during COVID-19. 22
In addition to 6 regular issues produced during 2020, PHR published a supplemental issue on public health policy approaches for reducing the morbidity, mortality, and incidence of HIV, viral hepatitis, sexually transmitted diseases, and tuberculosis. The supplement was sponsored by CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Its highlights include a commentary by the former US Surgeon General Jerome M. Adams, MD, MPH, on syringe services programs, 23 a rapid review of the impact of systems-level policies and interventions on population outcomes of the opioid epidemic, 24 and a report of the differential association of HIV funding with HIV mortality by race and ethnicity. 25
Important recent editorial changes included the appointment in 2019 of a new editor in chief, Hazel D. Dean, ScD, DrPH (Hon), FACE, of CDC’s Center for Surveillance, Epidemiology, and Laboratory Services, 26 and the streamlining of internal processes for improving authors’ publication experiences with PHR. One area for future exploration at the journal is a better understanding of its authors’ demographic characteristics, including how inclusive PHR has been in representing racial/ethnic and sex/gender-identity minority groups and researchers at various career stages, especially compared with other journals’ similar efforts. 27 Efforts to promote inclusiveness are already underway and include identifying editorial committee members and reviewers and calling for topical themes that reflect the increasingly diverse demographic of our society.
Footnotes
Authors’ Note
In addition to her position at the National Institutes of Health, P. Jones also serves as a member of the Editorial Committee of Public Health Reports.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.