
Abstract

Keywords
In the early 1980s, former US Department of Health and Human Services (HHS) Secretary Margaret M. Heckler convened the first federal group of experts to conduct a comprehensive study of the health status of racial/ethnic minority populations. The 1985 Report of the Secretary’s Task Force on Black and Minority Health, 1 also known as The Heckler Report, helped place minority health on the national stage. For the past 30 years, the report has served as a driving force for monumental changes in research, data, policies, programs, and legislation to address health disparities. For example, as a result of The Heckler Report, HHS established the Office of Minority Health (OMH) in 1986 and charged it with improving the health of racial/ethnic minority populations through the development of health policies and programs that eliminate health disparities.
Since the publication of The Heckler Report, much progress has been made to understand and address the health disparities of racial/ethnic minority populations. These disparities, which range from disease prevalence to health care access to health outcomes, are often linked to social, economic, or environmental disadvantages, such as unemployment, unsafe neighborhoods, and lack of affordable transportation options—conditions known as the social determinants of health. Less is known about involvement in the justice system (eg, arrests, court hearings, pretrial detention) including incarceration as factors that affect health, and limited federal funding is available to understand and address the health of persons involved in the justice system. 2 Attention to incarceration trends and criminal justice reform by researchers and advocates, however, has driven efforts by more researchers and policy makers to understand linkages between justice involvement and individual, family, and community well-being.
This supplemental issue of Public Health Reports focuses on the justice-involved population and health. Articles in this supplement examine the health of the justice-involved population and their families, propose policies and interventions to address health needs of the justice-involved population and their families, and assess how population health surveys can provide better information about the justice-involved population and identify opportunities for bridging knowledge gaps on health disparities and health needs of the justice-involved population.
The rate of incarceration in the United States is among the highest in the world. 3 Despite decreasing crime rates, the number of incarcerated persons increased by almost 350%, from 503 600 in 1980 to 2 225 100 in 2014. 4 In 2016, a total of 6.6 million persons were involved in the US criminal justice system, including 1.5 million in state and federal prisons, 740 700 in local jails, and 4.5 million on probation or under parole supervision. 5 And racial/ethnic minority groups are disproportionately represented in the justice-involved population, according to the most recent data (Table). Although non-Hispanic black persons composed 12.3% of the US population in 2016, 6 they constituted 37.0% of the federal prison population, 7 33.8% of the state prison population, 7 and 34.4% of the jail population. 8 Similarly, although Hispanic persons composed 17.3% of the US population in 2016, 6 they composed 32.0% of the federal prison population, 7 20.8% of the state prison population, 7 and 15.2% of the jail population. 8
General population and incarcerated populations in the United States, by race/ethnicity, 2016
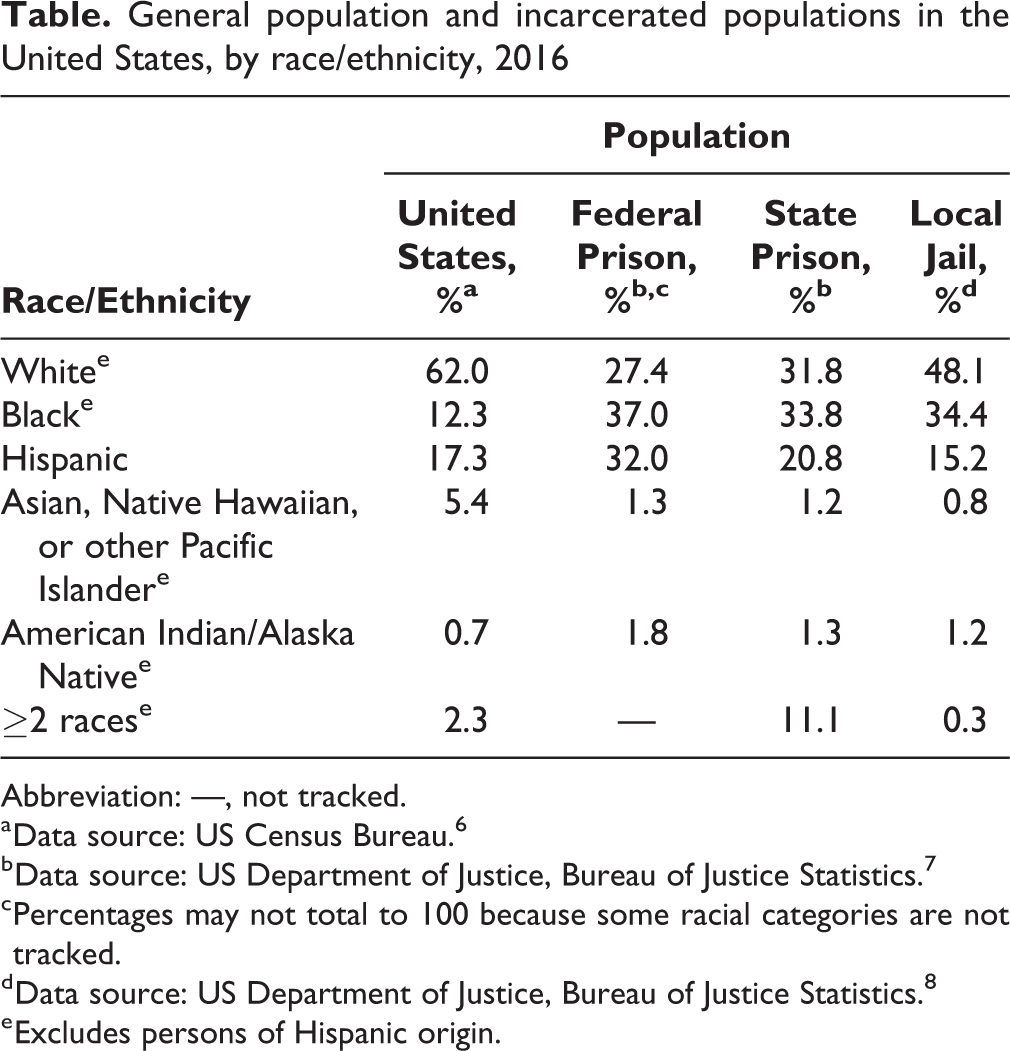
Abbreviation: —, not tracked.
a Data source: US Census Bureau. 6
b Data source: US Department of Justice, Bureau of Justice Statistics. 7
c Percentages may not total to 100 because some racial categories are not tracked.
d Data source: US Department of Justice, Bureau of Justice Statistics. 8
e Excludes persons of Hispanic origin.
Numerous health disparities exist between persons involved in the justice system and the general US population. Persons in state or federal prisons are 1.5 times more likely than persons in the general US population to report ever having a chronic condition, and half of all persons in state or federal prisons report having a chronic condition such as asthma, heart disease, or diabetes. Rates of infectious diseases, such as tuberculosis, HIV, hepatitis B and C, and sexually transmitted diseases, are higher among the incarcerated population than among the general US population. 9 More than half of the incarcerated population had a mental health problem (defined by recent clinical diagnosis, treatment, or symptoms of a mental disorder based on criteria specified in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition [DSM-IV]) at midyear 2005, including 56% of state prisoners, 45% of federal prisoners, and 64% of jail inmates. 10 Moreover, 58% of state prisoners and 63% of sentenced jail inmates met the DSM-IV criteria for drug dependence or abuse during 2007-2009. 11 Comparatively, 9.0% of persons aged 12 and older in the general US population had a substance use disorder in 2009, 12 and 11.3% of persons aged 18 and older had symptoms of serious psychological distress in 2005. 13
In addition to these disparities between the justice-involved population and the general US population, health disparities between racial/ethnic minority groups that are found in the general US population may also apply to the justice-involved population. These additional disparities may further exacerbate the disadvantage of justice-involved racial/ethnic minority populations compared with non-Hispanic white persons in the general US population. For example, African Americans are 7 times more likely than non-Hispanic white persons to die from HIV-related causes. 14 American Indian/Alaska Native adults are 2.4 times more likely than non-Hispanic white adults to be diagnosed with diabetes. 15 African American, Hispanic, and American Indian/Alaska Native persons are all more likely than non-Hispanic white persons to report having serious psychological distress. 16
Such substantial health disparities require a better understanding of the factors contributing to them, as well as innovative approaches that would enable policy makers and health systems to reduce those disparities. As part of its mission, OMH has initiated programs, policy efforts, and data initiatives to address the health needs of the justice-involved population and has partnered with other federal agencies on key initiatives to support and improve the health of this population. Using a social determinants of health lens, the office has sought to bridge the worlds of health, human services, and justice to support innovative policies and practices aimed at collaborative efforts to serve populations that are most vulnerable to health disparities and poor health outcomes. OMH implemented the HIV/AIDS Health Improvement for the Re-entry Population grant program 17 in 2012-2016 to improve the HIV/AIDS health outcomes of formerly incarcerated persons by supporting community-based efforts to ensure their successful transition from state or federal incarceration back to their communities. Grantees reported that their interventions resulted in improved connections to social services and improved medication adherence for formerly incarcerated persons enrolled in their services (unpublished data, OMH, November 2016). In October 2016, OMH launched the Re-entry Community Linkages (RE-LINK) program to address some of the health challenges of the justice-involved population by supporting the successful reentry of adults aged 18-26 who are released from jail. 18 RE-LINK funded projects in 8 cities to test the effectiveness of multiple stakeholders working together to implement a model transition process, which included health agencies ensuring access to health care coverage and health care and organizations providing housing, education, and employment services.
The development of partnerships with other agencies across HHS and with the US Department of Justice also reflects OMH’s commitment to understanding and addressing the social determinants of health through improved coordination and collaboration. For example, OMH partnered with the US Department of Justice in 2014-2017 on the Minority Youth Violence Prevention initiative, which brought together public health and law enforcement agencies to integrate public health and community policing approaches to reduce disparities in access to public health services, reduce the incidence of violent crimes, and improve the health and well-being of racial/ethnic minority communities. 19 Opportunities remain for OMH to collaborate with other stakeholders at the federal, state, county, local, and tribal levels through OMH channels, such as HHS’s Regional Minority Health Consultants, 20 to further address health disparities among the justice-involved population on a larger scale. The Regional Minority Health Consultants work in the 10 HHS regional offices to foster and strengthen relationships among federal, state, territorial, tribal, and community stakeholders to address minority health.
Although OMH’s demonstration grant programs help to provide evidence of effective practices for improving health status and health outcomes for the justice-involved population, the ability to measure the impact of criminal justice involvement and incarceration on health and health disparities has been challenging. This challenge is largely because of the limited number and lack of standardization of measures on criminal justice involvement and data on incarceration in health data collections. In March 2016, OMH hosted a workshop, “Improving Collection of Indicators of Criminal Justice System Involvement in Population Health Data Programs,” 21 along with the HHS Office of the Assistant Secretary for Planning and Evaluation and the National Academies of Sciences, Engineering, and Medicine Committee on National Statistics. The workshop convened subject-matter experts to identify recommendations for measures to assess criminal justice involvement as a social determinant of health and indicator of health status in health data collections. Stemming from discussions at this workshop, 3 articles in this supplement examine data methodology issues (eg, survey question wording, lack of relevant measures) to help bridge data gaps for understanding health status and health disparities within the justice-involved population. 22 -24 Another article discusses data gaps on pregnant women in the correctional system and the need to support a better understanding of their health and birth outcomes. 25
These and other articles in this supplement address the key issues and themes discussed at the March 2016 workshop, which are also woven throughout OMH’s justice and health portfolio, and highlight the public health implications of a vast and growing criminal justice system and population. Although the workshop supported a preliminary discussion centered on population health data collection, the articles in this supplement explore data and other issues in depth, providing additional information about incarceration-related health effects and proposing policies and interventions to address associated health disparities. For example, Wheeler and Mohle-Boetani 26 describe the effectiveness of a demonstration project that aims to treat tuberculosis within the correctional system, Massoglia and Remster 27 review the literature on linkages between incarceration and health outcomes, and Wise et al 28 examine the history of incarceration and HIV-related risk behaviors.
Addressing health at reentry is also important because more than 95% of incarcerated persons eventually return to their communities. 29 More than 600 000 persons are released each year after serving time in federal and state prisons, 7 and local jails have 10.6 million annual admissions and a 55% weekly turnover rate (the sum of weekly admissions and releases divided by the average daily population). 8 Incarcerated persons largely come from disadvantaged communities and return to underresourced neighborhoods and adverse conditions. In addition to pressing needs such as housing, employment, and education, barriers that negatively affect health can pose substantial challenges for returning citizens. Limited access to health coverage and health care can contribute to worsening health status of returning citizens and is associated with high rates of recidivism. 30 The risks of relapse, reoffending, and death are highest in the first days and weeks after release, making timely access to care and continuity of care especially important. 31
The effects of incarceration reach beyond prison and jail walls and affect the health of the families of incarcerated persons. Families of color are more likely than white families to be affected by incarceration. 30 In 2006, 44% of African American women and 32% of African American men had a family member who was imprisoned, compared with only 12% of white women and 6% of white men. 32 One in 28 children in the United States and 1 in 9 African American children in the United States had an incarcerated parent in 2008, 33 which puts these children at an increased risk of homelessness, financial instability, problems at school, and behavioral and mental health conditions, including depression and anxiety. 34 Wildeman et al 35 examine the research available on health consequences of incarceration on adult family members of incarcerated persons, adding to the limited body of knowledge on the effect of incarceration on the health and well-being of family members of incarcerated persons.
The economic costs of incarceration and unsuccessful reentry (eg, unemployment, lack of stable housing, relapse of substance use, recidivism) are high, especially costs linked to health. More than $12 billion is spent annually on health care in the public corrections system. 36 This figure increases dramatically when adding the costs of the entire justice system (eg, law enforcement, courts, prisons, jails) and indirect costs, such as the negative impact on employment, earnings, health, debt, housing, and food security. Incarcerated persons returning to the community with health needs, particularly mental illness or addiction, may face barriers to employment, have limited economic mobility, or remain persistently underemployed or unemployed, thus resulting in negative economic repercussions for the formerly incarcerated person, the person’s family, and the community. 33,37 Estimates by researchers show that inequities in health also result in tremendous costs. From 2003 to 2006, the estimated combined cost of health inequities and premature death in the United States was $1.24 trillion. 38 Health inequities experienced by formerly incarcerated persons could add to this cost. From both a societal and economic cost-benefit perspective, the health sector has an important role to play in addressing the health needs of formerly incarcerated persons. Access to health care and improved health status may also lead to improved opportunities for employment, housing, and family support, 30 which may result in better health and well-being for formerly incarcerated persons, their families, and their communities.
The health disparity issues raised in this supplemental issue of Public Health Reports represent a key priority for OMH as it continues to drive progress made since the release of The Heckler Report and work to advance health equity. It is also a key opportunity for the public health and justice fields to collaborate to inform and develop innovative and effective policies and programs that can support the health and well-being of the justice-involved population, improve public safety, and minimize the negative impact of collateral consequences (eg, poor health, family instability, ineligibility for employment). All persons in the United States, including persons who are currently incarcerated and formerly incarcerated persons who have paid their debt to society, should have the opportunity to reach their full potential for health, regardless of their race/ethnicity, age, gender, disability status, or socioeconomic status.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was funded by the US Department of Health and Human Services, Office of Minority Health.