
Abstract
Objectives
Estimating the prevalence of drug use in the general population is important given its potential health consequences but is challenging. Self-reported surveys on drug use have inherent limitations that underestimate drug use. We evaluated the performance of linking urine drug testing with a local, representative health examination survey in estimating the prevalence of drug use in New York City (NYC).
Methods
We used urine drug testing from the NYC Health and Nutrition Examination Survey (NYC HANES) to estimate the prevalence of drug use (benzodiazepines, cocaine, heroin, and opioid analgesics) among the study sample and compare the findings with self-reported responses to questions about past–12-month drug use from the same survey.
Results
Of 1527 respondents to NYC HANES, urine drug testing was performed on 1297 (84.9%) participants who provided urine and consented to future studies. Self-reported responses gave past–12-month weighted estimates for heroin, cocaine, or any prescription drug misuse of 13.8% (95% CI, 11.6%-16.3%), for prescription drug misuse of 9.9% (95% CI, 8.1%-12.1%), and for heroin or cocaine use of 6.1% (95% CI, 4.7%-7.9%). Urine drug testing gave past–12-month weighted estimates for any drug use of 4.3% (95% CI, 3.0%-6.0%), for use of any prescription drug of 2.8% (95% CI, 1.9%-4.1%), and for heroin or cocaine use of 2.0% (95% CI, 1.2%-3.6%).
Conclusion
Urine drug testing provided underestimates for the prevalence of drug use at a population level compared with self-report. Researchers should use other methods to estimate the prevalence of drug use on a population level.
Researchers and government health authorities have long been challenged by the difficulties of accurately determining the prevalence of drug use in the general population. 1 Precise data on the prevalence of potentially unhealthy substance use is imperative to inform public health interventions and policies. Population-based studies of the prevalence of drug use in the general population are typically based on voluntary self-reporting of substance use, such as the National Survey on Drug Use and Health (NSDUH) or the National Health and Nutrition Examination Survey (NHANES). Social desirability bias is particularly important because surveys on drug use involve disclosure of stigmatized and often illegal behavior. Therefore, population surveys may underestimate the prevalence of drug use, particularly injection drug use.2,3
Similar to how laboratory tests in NHANES provide national prevalence estimates of diabetes, 4 urine drug testing may help with estimating the prevalence of substance use on a population level. Urine drug testing has been used in studies to validate self-reported data from questions about substance use with a wide range of concordance.5-8 One study from a random sample of 627 adults aged 18-40 in Chicago found some utility in hair, urine, and oral drug testing to detect underreported drug use, with urine testing especially useful for detecting heroin use but not for detecting cocaine or recent marijuana use. 9
We tested urine specimens from participants of the New York City Health and Nutrition Examination Survey (NYC HANES), a local, representative health examination survey modeled on NHANES, 10 for the use of illicit drugs and misuse of prescription opioids and benzodiazepines to help estimate recent drug use. We anticipated that urine toxicology testing for drug use would correlate with self-report and therefore may be useful for estimating the prevalence of drug use in a major city in the United States.
Methods
Study Sample and Variable Definitions
We used self-reported data and urine testing from the 2013-2014 NYC HANES, a cross-sectional, population-based survey of noninstitutionalized adult New York City residents aged ≥20. Data collection for study participants consisted of 3 components: a 2-part interview, a physical examination, and a biologic specimen (blood, urine, and saliva) collection with an overall response rate of 36% (n = 1527). Details on the survey design, sampling strategy, and study population of NYC HANES are described elsewhere. 10 NYC HANES was approved by the City University of New York School of Public Health and the New York City Department of Health and Mental Hygiene (DOHMH) institutional review boards.
NYC HANES asked all respondents for data on self-reported past–12-month use of heroin, cocaine, prescription pain relievers (opioids such as oxycodone or hydrocodone), and prescription tranquilizers (benzodiazepines such as Xanax or Valium). NYC HANES determined misuse of prescription medications if respondents answered yes to 1 of 2 questions: “When you took prescription tranquilizers (or pain reliever) in the past 12 months, did you ever, even once, take more than was prescribed for you? This includes taking a higher dosage or taking it more often than directed” or “In the past 12 months, have you ever, even once, taken a prescription tranquilizer (or pain reliever) that was not prescribed for you?” The survey focused on these drugs because these drugs have historically contributed the most to drug overdose mortality in New York City. 11
At the time of enrollment in NYC HANES, participants consented to having their biological specimens stored for future research and had to indicate in the informed consent a yes or no response to the following statement: “I agree that the samples I provide can be stored for future public health research.” Therefore, participants were not aware that their urine would be tested specifically for drug metabolites. Blood and urine specimens are stored in a specimen bank at DOHMH and saliva specimens are stored at Albert Einstein College of Medicine in the Bronx, New York. All biological specimens stored for future research are stored with a unique specimen identification number and stored indefinitely unless removal is requested by a study participant.
This study involved a separate protocol written after completion of NYC HANES for the testing of the urine specimens for drug use, which was reviewed and approved by the NYC DOHMH institutional review board. DOHMH gave each specimen an identification number. DOHMH created a special drug panel for this study; we selected 10 analytes from standard validated tests: benzodiazepines, cocaine, codeine, hydrocodone, hydromorphone, methadone, morphine, oxycodone, oxymorphone, and 6-acetylmorphine. This panel would be similar to urine drug testing commonly used in clinical practice, 12 but it only included drugs that were asked about in NYC HANES. Testing for each specimen gave a binary positive or negative result for the presence of each drug tested. We grouped test results as any drug (any positive test), any prescription drug (positive test for benzodiazepines, codeine, hydrocodone, hydromorphone, methadone, morphine, oxycodone, or oxymorphone), and heroin (positive test for 6-acetylmorphine) and cocaine (positive test for cocaine). Quest Diagnostics performed urine testing by using immunoassay technology for the initial screening test; test results equal to or greater than a calibrated immunoassay cutoff concentration identified positive specimens. The laboratory conducted confirmatory testing on all initial positive screening tests.
Statistical Analysis
We weighted all survey data to adjust for the complex sampling design, nonresponse, missing data, and poststratification using the 2013 American Community Survey. 13 We suppressed urine-testing results for specific drugs because of the small number (≤5) of results with a positive value. We age-standardized all prevalence estimates to the 2000 US population 14 and rounded to the nearest 1000. All studies from the NYC HANES are age standardized to the 2000 US population because this is the second iteration of NYC HANES (the first was in 2004). Therefore, both surveys were age standardized to the 2000 US Census so they could be directly compared. We calculated weighted prevalence estimates for self-reported drug use for 3 categories: any drug misuse (heroin, cocaine, and misuse of prescription opioid analgesics or benzodiazepines), any prescription drug misuse (opioid analgesics or benzodiazepines), and any heroin or cocaine use by sex (male/female), age group (20-39, 40-59, ≥60), and race/ethnicity (non-Latino White, non-Latino Black, Latino, non-Latino Asian, non-Latino other). For urine drug testing, we calculated weighted prevalence estimates for 3 categories: any drugs (heroin, cocaine, prescription opioid analgesics, or prescription benzodiazepines), presence of prescription drugs (opioid analgesics or benzodiazepines), and the detection of heroin or cocaine. We used SAS version 9.4 (SAS Institute Inc) for statistical analysis and SUDAAN version 11.0.1 (RTI Intl) for applying survey weights.
Results
Of 1527 respondents to NYC HANES, 1297 (84.9%) consented to having their specimens used for future research and were tested for drug use (Table). For heroin, cocaine, or prescription drug misuse, self-report gave a weighted prevalence of 13.8% (95% CI, 11.6%-16.3%), whereas urine drug testing estimated a weighted prevalence of 4.3% (95% CI, 3.0%-6.0%). For drug categories, self-report gave a weighted prevalence of 9.9% (95% CI, 8.1%-12.1%) for any prescription drug misuse, whereas urine drug testing estimated a 2.8% (95% CI, 1.9%-4.1%) prevalence for any prescription drug misuse; self-report of heroin or cocaine gave a weighted prevalence of 6.1% (95% CI, 4.7%-7.9%), and urine testing estimated a weighted prevalence of 2.0% (95% CI, 1.2%-3.6%).
Prevalence estimates for drug use by self-report and urine drug testing, New York City, 2013-2014 a
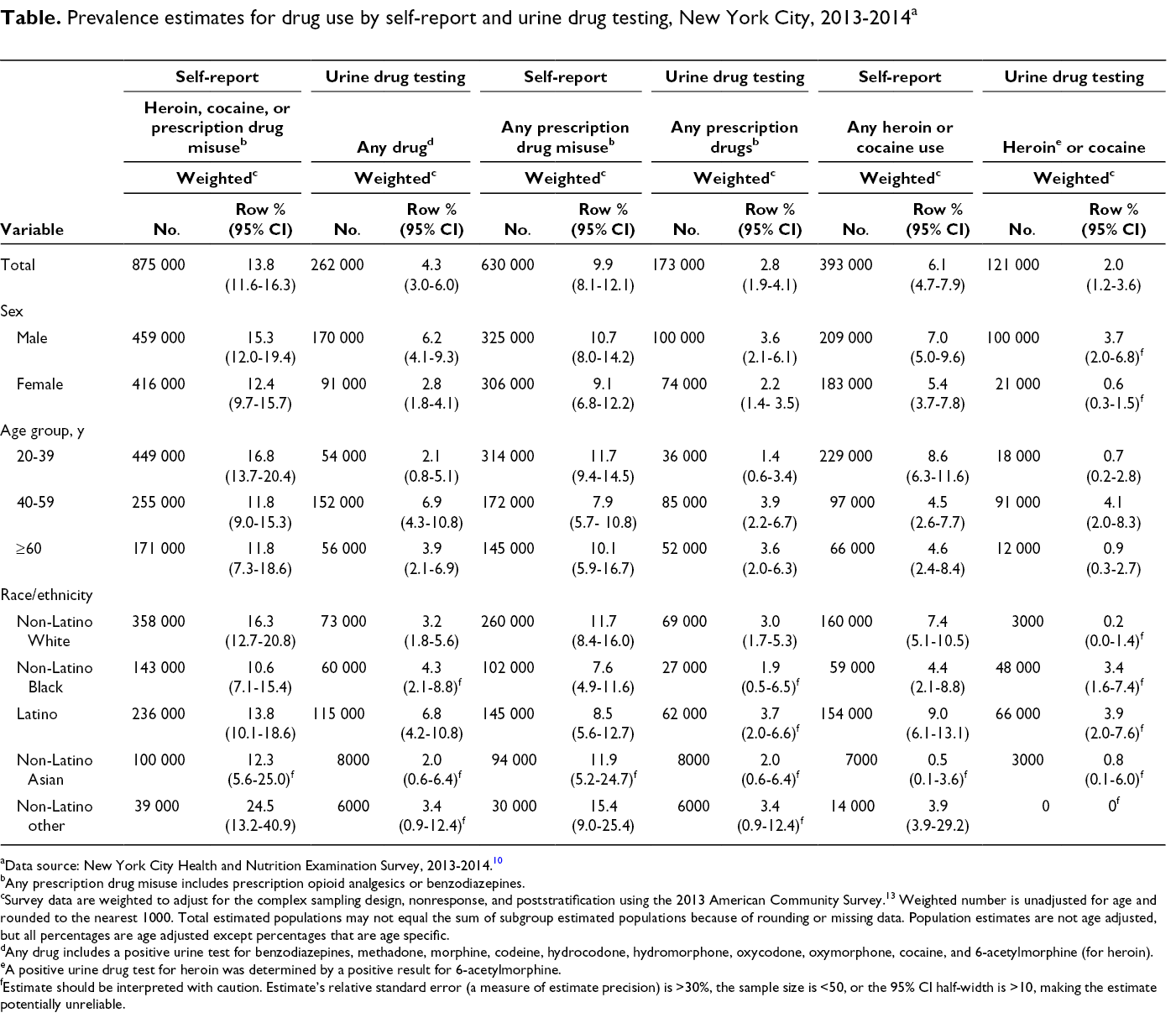
aData source: New York City Health and Nutrition Examination Survey, 2013-2014. 10
bAny prescription drug misuse includes prescription opioid analgesics or benzodiazepines.
cSurvey data are weighted to adjust for the complex sampling design, nonresponse, and poststratification using the 2013 American Community Survey.13 Weighted number is unadjusted for age and rounded to the nearest 1000. Total estimated populations may not equal the sum of subgroup estimated populations because of rounding or missing data. Population estimates are not age adjusted, but all percentages are age adjusted except percentages that are age specific.
dAny drug includes a positive urine test for benzodiazepines, methadone, morphine, codeine, hydrocodone, hydromorphone, oxycodone, oxymorphone, cocaine, and 6-acetylmorphine (for heroin).
eA positive urine drug test for heroin was determined by a positive result for 6-acetylmorphine.
fEstimate should be interpreted with caution. Estimate’s relative standard error (a measure of estimate precision) is >30%, the sample size is <50, or the 95% CI half-width is >10, making the estimate potentially unreliable.
Across all demographic groups, urine drug testing gave lower estimates than self-reported use in all drug categories (Table). Men had higher prevalence estimates than women in all drug categories and by self-report and urine drug testing. The magnitude of the difference between urine drug testing estimates and self-report estimated was larger among adults aged 20-39 than among adults aged 40-59 and ≥60. Among all age groups, adults aged 20-39 had the highest estimated prevalence of drug use based on self-report (16.8% [95% CI, 13.7%-20.4%] for self-reported heroin, cocaine, or prescription drug misuse) but the lowest estimated prevalence based on urine drug testing (2.1%; 95% CI, 0.8%-5.1%). By race/ethnicity, non-Latino other had the highest prevalence rates for any drug use (24.5%; 95% CI, 13.2%-40.9%) and prescription drug misuse (15.4%; 95% CI, 9.0%-25.4%) by self-report, but Latino people had the highest prevalence rates for these categories based on urine drug testing (6.8% [95% CI, 4.2%-10.8%] for any drug; 3.7% [95% CI, 2.0%-6.6%] for prescription drugs; and 3.9% [95% CI, 2.0%-7.6%] for heroin or cocaine).
Discussion
Our analysis found that urine drug testing of participants of NYC HANES gave substantially lower prevalence estimates of drug use than past–12-month self-reported national prevalence data. 15 Initially, we hypothesized that the rates of drug use based on urine drug testing of the NYC HANES population would be 8%-10%. We also anticipated that this investigation would contribute to knowledge about the prevalence of drug use, provide a demographic profile of people using drugs, identify the type of drugs used, and highlight geographic characteristics to inform targeted harm reduction interventions, including overdose prevention. However, we found that the estimates of drug use from urine drug testing were too low and unreliable to be helpful in public health planning for New York City; nevertheless, we learned several important lessons.
First, urine drug testing has the disadvantage of a short window of detection of most drugs, ranging up to 3 days for cocaine, 7 days for benzodiazepines, 1-4 days for most opioids including 6-acetylmorphine, and up to 11 days for methadone.12,16 This short window of detection severely limits the ability to detect current drug use, usually defined as past-month usage. 14 NYC HANES asked only about past–12-month use, and with this difference in time periods between the survey questions and urine tests, the self-reported results were not fully comparable with the urine test results. Occasional and even frequent drug users could self-report use during the past 12 months but would be unlikely to have a positive urine toxicology unless they had used the drug during the few days before testing. Therefore, urine drug testing can provide estimates on drug use only within a short window (ie, up to 11 days) and does not necessarily capture data on all problematic or current use.
Second, urine drug testing in our study required a specific consent by participants to have their biological specimen tested for future research. Therefore, selection bias may have occurred as to who decided to allow storage and future testing of their biological specimens and who did not. Although participants did not know their samples would be tested for drugs, some participants may have been concerned about this possibility and declined to have their biological sample stored for future testing. Therefore, we cannot rule out potential selection biases; however, most (84.9%) participants agreed to have their urine tested. Third, the approximate cost for the urine drug testing of all samples (both screening and confirmatory tests) was $30 000 in addition to survey costs; therefore, urine drug testing was not cost-effective for the data and knowledge gained from this study. Furthermore, because of the small sample size of NYC HANES, we were unable to obtain stable prevalence estimates for comparisons of self-reports and urine toxicology results. Finally, this study attempted to estimate the prevalence of drug use in New York City at a single point in time (2013-2014); therefore, data cannot be extrapolated to today or used to examine trends over time.
To our knowledge, this is the first study to attempt to use urine drug testing in conjunction with a weighted, representative, population-based survey to estimate the prevalence of drug use in the general population of a large metropolitan US city. A study conducted in Chicago in 2001 and 2002 used a population drug survey of a random population and found that adding biological testing (hair, urine, saliva) led to increased estimates of past–3-month cocaine use, from 4.2% to 13.1%. 9 Another study that compared self-reported drug use with urine drug testing in a clinical trial of 500 smokers under community corrections supervision found high rates of nonconcordance (ie, high false-negative rates where self-report denied use while urine drug testing was positive) for past–30-day cocaine, opioid, and marijuana use. 5 However, our experience using self-reported data and urine samples being collected for the NYC HANES found that the data from urine drug use testing were not reliable, and overall self-report gave higher prevalence estimates for drug use. Although multiple biological testing (hair, urine, saliva) could have more utility such as in the study conducted in Chicago,9 it would not address the issue of potential selection bias and would incur higher associated costs. Therefore, given our experience with urine drug testing and its limitations, we believe focus should be on using other data sources to estimate the prevalence of drug use at the population level. 1 Public health departments could use the intersection of multiple data sources, such as drug-related hospitalizations, substance use disorder treatment services, and mortality data from drug overdoses, along with data from NSDUH and medication prescription records to help estimate the prevalence of problematic drug use at the population level. Using multiple data sources may also be useful for identifying and describing distinct subgroups of problematic drug users and identifying particularly high-risk populations to inform tailored interventions.
Conclusion
Urine drug testing of respondents to a population health survey in New York City was not found to be useful or cost-effective to estimate the prevalence of drug use in New York City, likely because of the short window of drug detection. Different approaches using various data sources are recommended for surveillance of drug use on a population level.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant K23DA043651 (Han) from the National Institute on Drug Abuse.