
Abstract
Keywords
Drug overdose is a critical public health concern in the United States. More than 107 000 drug overdose deaths occurred in 2022, a slight increase from 2021. 1 Recent estimates of nonfatal drug overdoses treated in emergency departments, however, indicate a decline in rates from 2021 to 2022. 2 Opioids, primarily illegally made fentanyls, were the most commonly identified drug in fatal drug overdoses in 2022, followed by psychostimulants with abuse potential and cocaine. 3 In 2018, opioids were the most commonly identified drug in nonfatal drug overdoses treated in emergency departments, followed by benzodiazepines and stimulants. 4
Care and treatment for people at risk for drug overdose, including medications for opioid use disorder (MOUD), behavioral treatment, harm reduction services, and social services, can reduce the risk of overdose.5,6 The strongest evidence base for effective treatment of opioid use disorder (OUD) is US Food and Drug Administration–approved medications (ie, methadone, buprenorphine, and extended-release naltrexone) alone or in combination with behavioral health strategies such as counseling, motivational interviewing, 6 and cognitive behavioral therapy.7,8 Because US Food and Drug Administration–approved pharmacologic treatment for stimulant use disorder is lacking, evidence-based treatment options include behavioral health strategies such as motivational interviewing, contingency management, community reinforcement approach, and cognitive behavioral therapy. 9
People at risk for overdose can be identified and linked to care and treatment in a range of settings or “entry points,” such as clinical settings, harm reduction and syringe service programs, criminal justice settings, and community-based organizations. However, gaps remain in understanding how often these people are linked to and retained in care along with longitudinal outcomes among people receiving treatment. The lack of consistent and standardized surveillance data across jurisdictions limits the ability to monitor population-level linkage to and retention in care (LTC) for substance use disorders (SUDs) and associated outcomes.
A small number of US surveillance systems capture data on LTC for SUD, and existing systems have limitations. The Substance Abuse and Mental Health Services Administration’s National Survey on Drug Use and Health provides national-, state-, and substate-level data on SUD prevalence for specific substances, need for and receipt of treatment including MOUD, and perceived recovery among household respondents. 10 Limitations of the National Survey on Drug Use and Health include lack of timeliness, exclusion of some populations with a disproportionate risk of overdose (eg, people who are unsheltered or incarcerated), and limited availability of local-level data. The Substance Abuse and Mental Health Services Administration’s Treatment Episode Data Set (TEDS) 11 provides national- and state-level data on admissions to and discharges from publicly funded substance use treatment programs, but TEDS provides limited information on how people were linked to care and is not representative of all treatment settings (eg, it excludes data on treatment in private facilities). No existing surveillance system provides comprehensive estimates across the cascade of care for SUD—from identification of need to treatment linkage (ie, initiation), to retention in treatment and recovery. Some state and local health departments conducted surveillance of LTC for SUD using local data systems with funding from the Centers for Disease Control and Prevention’s (CDC’s) Overdose Data to Action (OD2A 12 ) cooperative agreement during 2019-2023. 12 Under OD2A, 20 CDC-funded state and local health departments used locally available data to identify and track various LTC-related indicators and outcomes. However, funded health departments did not use standardized indicators, which prohibited comparisons of outcomes across jurisdictions.
Developing and implementing a cascade of care model for SUD and a set of standardized LTC surveillance indicators can provide information that can be used by public health partners to guide overdose prevention and response efforts. Previous research has built upon the HIV cascade of care to identify stages relevant to OUD.13-15 For example, Williams et al13-15 developed and later updated an OUD-specific framework with several distinct stages: (0) primary prevention, (1) secondary prevention, (2) estimated prevalence of OUD, (3) OUD diagnosed, (4) linkage to care, (5) MOUD initiation, (6) MOUD retention >6 months, and (7) remission or recovery. The Rhode Island Department of Health leveraged an early version of this framework to develop a state-specific cascade of care that used various data sources to measure 5 stages: (0) at risk, (1) diagnosed, (2) initiated, (3) retained, and (4) recovery. 16 Cascade of care models for OUD have also been applied to specific settings and populations, such as jails, 17 a public hospital system in New York City, 18 and the Florida Medicaid population. 19
The primary objective of this commentary is to describe CDC’s process for identifying a cascade of care model for SUD and developing a set of standardized indicators to advance local- and state-level surveillance of LTC for SUD. A secondary objective is to describe how these indicators can be used by state and local health departments to monitor and improve efforts to connect people at increased risk for overdose to evidence-based treatment and other support services.
Process for Developing the Cascade of Care for SUD and Standardized Indicators
To develop the cascade of care and standardized indicators, we conducted an environmental scan of published literature, regulations, government reports, and existing public health practice to identify existing LTC models and indicators. We used this information to develop a foundational model consisting of 3 primary stages: (1) diagnosis, (2) linkage to treatment, and (3) retention in treatment (ie, ≥6 months). Staff from OD2A-funded state and local health departments, with expertise in overdose surveillance, prevention, and response, provided iterative input that was used to expand and refine the model and identify a set of indicators that would be feasible to implement with available data. The resulting LTC surveillance indicators offer a minimum set of standardized measures that health departments can use to assess whether people at increased risk for overdose are referred to, linked to, and retained in treatment.
The cascade of care for SUD (Figure) describes a progression through 6 stages adapted to measurable surveillance indicators at a granular level: (1) identification of people in need of treatment, (2) engagement with LTC programs, (3) referral to care and treatment, (4) linkage to treatment (eg, initiation), (5) treatment retention, and (6) recovery. Many people who may benefit from treatment are never diagnosed with an SUD. 20 Therefore, to capture the largest population possible, people in need of treatment are broadly defined as people with a confirmed SUD diagnosis or who meet criteria consistent with an SUD. 21 This model intentionally focuses on linking people in need to evidence-based care and treatment services, although some individuals may progress to a state of recovery without treatment.
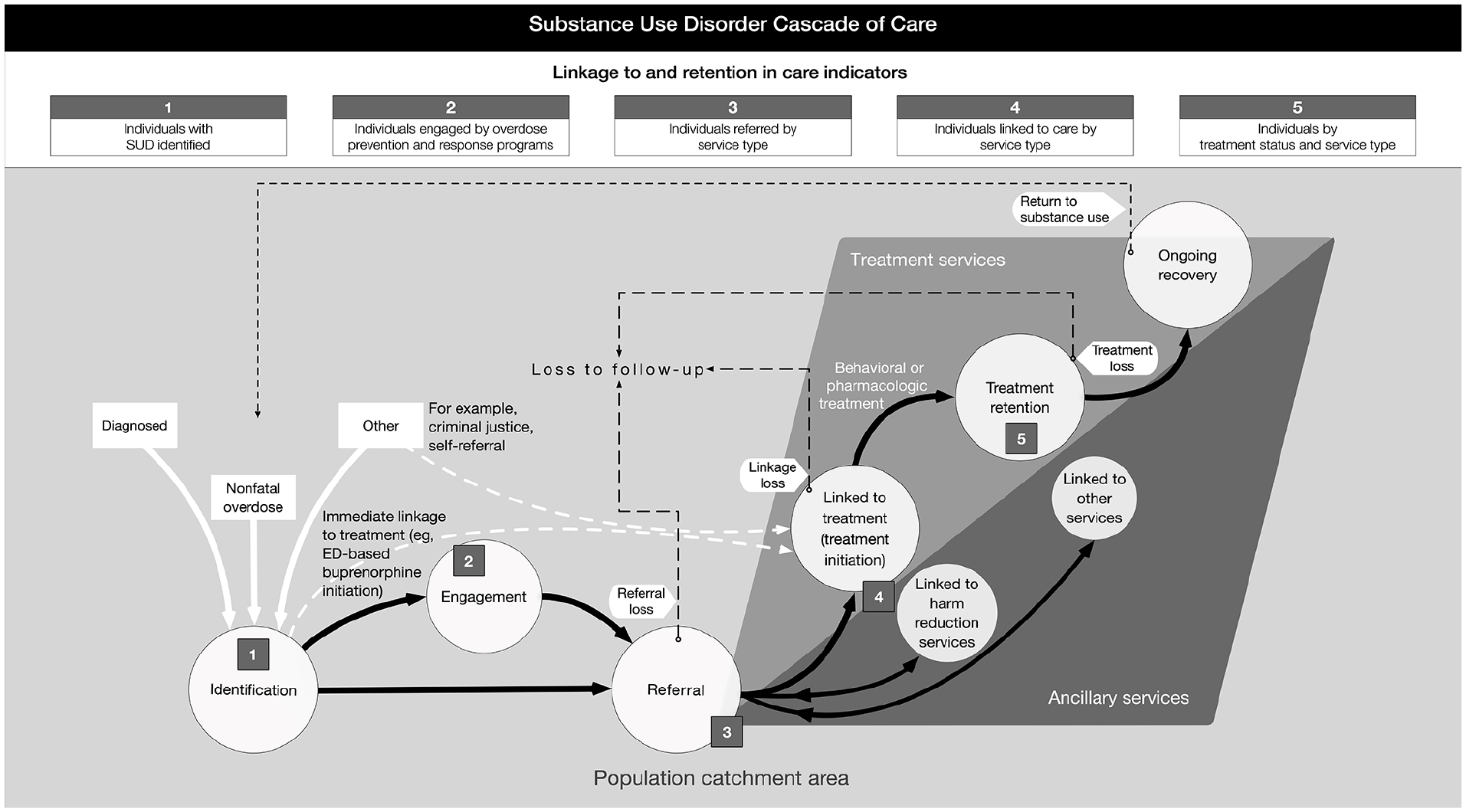
The cascade of care for substance use disorder. The figure shows how people with a substance use disorder may progress along the cascade of care to receive care and treatment services and the linkage to and retention in care surveillance indicators used to measure each stage. Abbreviation: ED, emergency department.
People may not follow a linear progression through the SUD cascade of care. Some may self-refer to treatment programs, bypassing public health identification, and some may be lost to follow-up and then reengage with treatment. Moreover, some people with an SUD may not perceive a need for treatment or be ready for treatment.22-24 The model includes these contingencies with people lost to follow-up being reengaged along the cascade of care and potentially being relinked to treatment and ancillary services. Although the model concludes with recovery, SUD treatment does not have a well-defined endpoint and can be lifelong for some people.14,16,25
The LTC surveillance indicators (Table) follow the SUD cascade of care from identifying people in need of treatment to describing treatment status 6 months after initiation of care. The indicators are designed to be flexible in implementation and to consider a health department’s capacity to collect and analyze data on LTC indicators. Health departments can use these standardized indicators to prioritize the relationships, data, and technology necessary to advance surveillance of LTC for SUD.
Linkage to care surveillance indicators for the substance use disorder (SUD) cascade of care
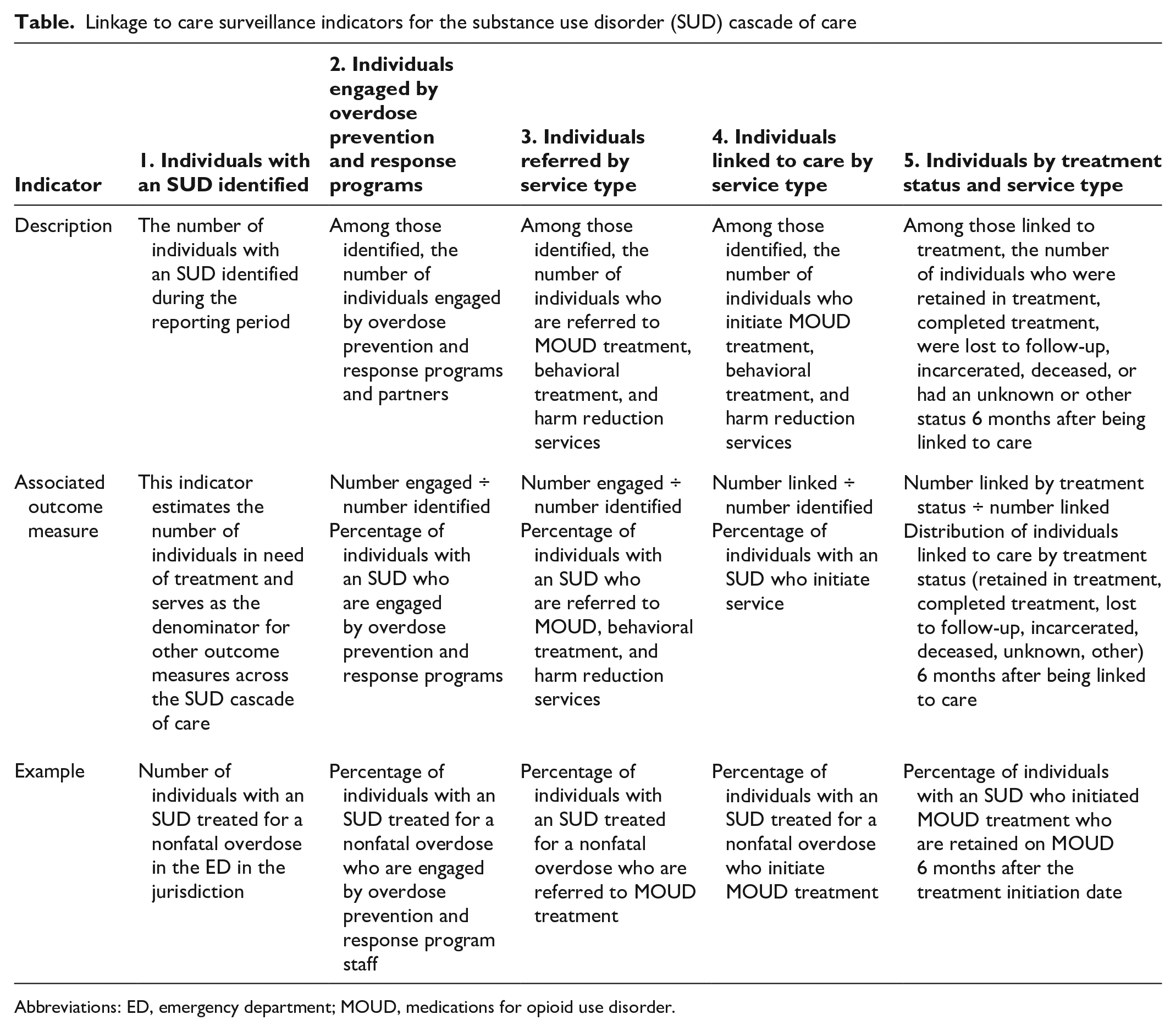
Abbreviations: ED, emergency department; MOUD, medications for opioid use disorder.
Individuals With an SUD Identified
This indicator establishes baseline counts of people with an SUD identified through public health surveillance across entry points. Entry points define important cohorts, including people treated in emergency departments or by emergency medical services for a nonfatal overdose, people soon to be or recently released from jail or prison, people accessing harm reduction services, and people diagnosed with comorbid conditions (eg, acute hepatitis C).
Individuals Engaged by Overdose Prevention and Response Programs
This indicator counts the number of people identified who are engaged by overdose prevention and response program staff (eg, peer navigators, care coordinators, case managers, peer support specialists) through in-person contact, telephone calls, or other personal interactions. As the numerator, this indicator can be used to calculate the percentage of people with an SUD who are engaged by overdose prevention and response programs.
Individuals Referred by Service Type
This indicator counts the number of people identified who are referred to (1) MOUD, (2) behavioral treatment, and (3) harm reduction services. As a numerator, health departments can use this indicator to calculate the percentage of people with SUD identified who were referred to various care and treatment options. As a denominator, this indicator can track the effectiveness of referrals potentially leading to linkage to or initiation of care and treatment services.
Individuals Linked to Care by Service Type
This indicator counts the number of people identified who initiate (1) MOUD, (2) behavioral treatment, or (3) harm reduction services. Health departments can use this indicator to estimate the percentage of people with an SUD who initiate care and treatment services.
Individuals by Treatment Status and Service Type
This indicator describes treatment status 6 months after treatment initiation separately for (1) MOUD and (2) behavioral treatment. Treatment status options may include retained, completed, lost to follow-up, incarcerated, or deceased. Health departments can use this indicator to estimate treatment retention and loss to follow-up at 6 months. Little consensus on a measured endpoint for SUD treatment exists. 25 Clinical quality measures, such as the Centers for Medicare & Medicaid Services’ Merit-based Incentive Payment System program, endorse 180 days of continuous pharmacotherapy for MOUD treatment as a minimum duration of care. 26 The proposed 6-month follow-up period for treatment status aligns with these quality measures and provides a feasible follow-up period for health departments even if most patients require multiyear, if not indefinite, MOUD. 27
Using Surveillance Data to Improve Linkage to Care Programs
Health departments and other public health partners can use actionable surveillance data at each step of the SUD cascade of care to monitor and improve LTC programming. The proposed LTC indicators can be stratified by demographic characteristics, entry points, SUD type, and other program parameters to identify intervention needs and evaluate programs. These data are essential in designing and evaluating efforts to improve LTC and directing public health resources to prevent nonfatal and fatal overdoses.
Health departments play an important role in coordinating efforts to collect, link, and analyze data from multiple sources and in sharing LTC surveillance data with community partners to design and implement effective interventions. Health departments can also use partner relationships with emergency medical services, law enforcement, clinicians, harm reduction organizations, treatment providers, people with lived experience, and other organizations to share data and provide valuable insight for overdose prevention and response program planning.
Measuring LTC indicators requires collecting and linking data from multiple sources often managed by various partners and housed in different systems. Potential data sources include emergency department visit or hospital discharge data on nonfatal overdoses, Medicaid or health insurance claims data related to SUD treatment, prescription drug monitoring program data on buprenorphine prescriptions, data from criminal justice partners, and harm reduction program data. Linking individual-level data from these disparate systems will provide a more complete picture of LTC along each stage of the SUD cascade of care compared with measures from isolated systems while identifying areas where programs may need to tailor their approach or allocate dedicated staff and resources.
Overdose prevention programs may vary in their readiness to collect and analyze LTC surveillance data. As programs build capacity related to relationships, data, and technology, their ability to conduct surveillance throughout the SUD cascade of care will improve. Health departments that take advantage of available data sources will gain valuable experience to support a more integrated and interoperable system. Investments in collecting and managing linkable, timely data, especially treatment data, will exponentially improve SUD cascade of care surveillance.
Opportunities to Expand Surveillance of LTC for SUD
Several health departments have begun implementing components of the standardized LTC indicators in their communities. In 2023, CDC began funding 12 local health departments via the Overdose Data to Action: Limiting Overdose through Collaborative Actions in Localities (OD2A: LOCAL) cooperative agreement to collect and analyze data on LTC indicators and disseminate findings to local partners to inform LTC prevention efforts. 28 Funded health departments are planning and taking steps to identify key data sources, develop data use agreements with partners, create data collection tools and systems, and investigate the feasibility of linking individual-level data across data sources. Plans include linking individual-level nonfatal overdose data with Medicaid claims data to measure treatment linkage and retention among people who experienced a nonfatal overdose and training peer navigators to collect data on the LTC indicators using a case management system. This work will help determine the feasibility of collecting standardized LTC surveillance data, identify any essential refinements to the LTC indicators, and disseminate best practices informed by OD2A: LOCAL recipients.
Establishing data use and data-sharing agreements with partners who maintain key data sources can facilitate health departments’ access to timely data, thereby improving data usability to inform programmatic and policy decisions. Health departments can foster relationships and engage with agencies that manage SUD treatment data to identify best approaches for sharing these data. Ongoing technology and policy advancements can further broaden health departments’ capacity to implement LTC surveillance.
Technical solutions can also facilitate the sharing, access, and use of data that exist in siloed systems with various governance, privacy, and ethical considerations. Technical solutions such as Fast Healthcare Interoperability Resource–based application programming interfaces could support data exchange between service providers and health departments. 29 Query and response functions using Fast Healthcare Interoperability Resource paradigms could allow health departments to proactively request and securely receive data necessary for LTC surveillance from health care providers. Identity management and matching solutions, such as Privacy Preserving Record Linkage, 30 allow individual-level data linkage without compromising privacy. For example, a single state health department used Privacy Preserving Record Linkage to match and integrate records from disparate data sources to create a longitudinal data platform used to inform SUD prevention, treatment, and harm reduction interventions. 31 This process allows partners to share data without exposing personally identifiable information.
Advancements that align privacy, regulatory, and legal policies can support health departments’ access to SUD treatment data, which are critical for measuring LTC and treatment outcomes (eg, initiation, retention, loss to follow-up) while preserving patient privacy. In February 2024, the US Department of Health and Human Services published revisions to 42 CFR Part 2, which included allowing disclosure of deidentified treatment records to public health authorities without requiring patient consent and streamlining data sharing by aligning privacy protections with Health Insurance Portability and Accountability Act standards. 32 Patients can also consent to sharing their data, including for public health surveillance purposes. While the previous regulations impeded care coordination and treatment providers’ ability to share treatment data with health departments, these recent changes may improve health departments’ ability to track treatment initiation and retention indicators. However, allowing access to identifiable data for public health surveillance would likely support health departments’ ability to link patient records across data sources, monitor progress through the cascade of care, and evaluate and enhance LTC interventions.
Conclusions
The development of standardized indicators across the cascade of care is essential to inform and improve programmatic efforts focused on linking and retaining people in care and treatment for SUDs. These efforts involve multisector collaborations across federal agencies, health systems and health care providers, state and local health departments, and community-based organizations as well as bidirectional data sharing and communication to reach populations at greatest risk for overdose. Timely and standardized surveillance data are the foundation for informing efforts to address the overdose crisis in the United States.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Williams receives consulting fees and equity from Ophelia Health Inc, a treatment provider for opioid use disorder.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kahuina Consulting, LLC’s contribution was supported by the Centers for Disease Control and Prevention under contract nos. 75D30121C12151 and 75D30123C16234.