
Abstract
Objective:
Previous nonfatal overdose is a key risk factor for drug overdose death; however, current nonfatal overdose surveillance is limited to people who receive medical attention. We identified states that tracked nonfatal overdoses treated in prehospital and hospital care settings, assessed the effects of different surveillance methods on the magnitude of nonfatal overdose estimates, and estimated states’ nonfatal-to-fatal overdose ratio.
Methods:
Two analysts independently reviewed state websites to characterize states’ methods of capturing nonfatal overdose events from December 2022 through February 2023. We collected information on surveillance methods in 5 states that met the inclusion criteria, including data source, measure specification, drug(s) involved, and whether states performed deduplication or published mutually exclusive measure specifications to capture unique events across care settings. We calculated nonfatal-to-fatal overdose ratios to assess the effects of different data sources on estimates of nonfatal overdoses.
Results:
Illinois, Maine, North Carolina, and West Virginia used syndromic surveillance data and New Jersey used hospital discharge data to track nonfatal overdose-related emergency department visits. Illinois and West Virginia tracked nonfatal overdose-related encounters with emergency medical services. Other states tracked opioid overdoses reversed following naloxone administration by emergency medical services, law enforcement, and community members. Maine, New Jersey, and West Virginia published nonfatal overdose information by using mutually exclusive measure specifications; the number of nonfatal overdoses per fatal overdose in these states ranged from approximately 5:1 to 14:1.
Practice Implications:
Establishing a standard framework to combine data from existing national surveillance systems in prehospital and hospital care settings can improve nonfatal overdose estimates and enable comparisons between jurisdictions to help decision makers identify areas most in need of essential services.
More than 110 000 people in the United States died from drug overdose in the 12-month period ending in September 2023. 1 Although nonfatal overdose is a key risk factor for drug overdose death, decision makers traditionally have used fatal overdose data (which often lags by 6 months or more) to inform policy and programmatic decisions.2-4 Nonfatal overdose estimates can supplement fatal overdose data by providing more timely insights that would enable decision makers to intervene and connect people to lifesaving resources. However, comprehensively capturing data on nonfatal overdoses can be difficult because many of these events occur outside the health care system, and people can be treated by first responders or community members, transported to a hospital, or left untreated.
Current state and national-level nonfatal overdose surveillance primarily tracks the number of overdose responses in prehospital settings (by emergency medical services [EMS] and law enforcement) and hospital care settings (emergency departments [EDs] or inpatient hospitalizations). 5 Each data source provides a unique perspective of drug overdoses occurring among individuals who interact with medical services; however, these data systems may separately capture information on the same person or overdose event (eg, if a person is treated by EMS and transported to an ED), thus making it difficult to combine these data into a single comprehensive estimate of nonfatal overdose.
Overdose surveillance systems are limited to nonfatal overdoses that are treated within the health care system, thus potentially missing a substantial number of overdose events that do not receive medical attention or are successfully reversed by community members in the absence of a medical professional. Lack of professional medical attention after an overdose could also result from stigma, drug use in isolation, limited EMS or ED capacity, or fear of legal repercussions for people who call 9-1-1 for a drug overdose.
Having comprehensive nonfatal overdose data to supplement fatal overdose estimates could provide additional insights, such as an estimation of the ratio of nonfatal-to-fatal overdoses, which can help decision makers assess and predict the number of overdose events in specific localities; identify populations in greatest need of prevention, harm reduction, and treatment services; and guide efficient distribution of lifesaving opioid overdose reversal medications (eg, naloxone).
Few estimates of nonfatal-to-fatal overdose ratios have been published. One nationwide study estimated that approximately 15 nonfatal overdoses per 1 fatal overdose were treated in EDs from 2010 through 2020. 6 Minnesota and Rhode Island have also estimated nonfatal-to-fatal overdose ratios (14:1 and 37:1, respectively).7,8 However, given the differences in the data sources used to derive this metric, further work is needed to comprehensively capture and standardize methods of estimating nonfatal overdoses in the United States.
In this study, we examined publicly available information on drug overdose surveillance methods of states currently reporting nonfatal overdose responses by EDs and first responders. We aimed to (1) identify states capturing data on nonfatal overdoses in prehospital and hospital care settings, (2) assess the effects that different data sources and measure specifications can have on the magnitude of nonfatal overdose estimates, and (3) estimate the ratio of nonfatal-to-fatal overdoses as a metric to inform drug policies and programs among states monitoring nonfatal overdose in prehospital and hospital care settings.
Methods
We conducted this study in 2 phases. For phase 1, which occurred in July and August 2022, we manually reviewed publicly available information published on government websites for all US states and the District of Columbia regarding their efforts to monitor local responses to suspected drug overdoses. We evaluated published reports and surveillance dashboards based on selected characteristics of their overdose surveillance methods, including type of data, timeliness, drug involvement, and specification of nonfatal outcomes. Detailed methods and results from this analysis have been published elsewhere. 5
For phase 2, which occurred from December 2022 through February 2023, we conducted a detailed manual and quantitative review of nonfatal overdose surveillance methods among states monitoring nonfatal overdoses in both prehospital and hospital care settings. To meet inclusion criteria, states were required to publish, on their state website, data related to both nonfatal overdoses treated in an ED and nonfatal overdoses treated by first responders (EMS or law enforcement). States were also required to publish fatal overdose data of the same year and drug type as the nonfatal overdose indicators. We excluded states if fatal and nonfatal estimates were not published as counts for a full calendar year (to guide calculations of nonfatal-to-fatal overdose ratios). Among states meeting inclusion criteria, we conducted further characterization of their methods of capturing and reporting drug overdose events.9-13 For fatal and nonfatal overdose data, we recorded the data source, year, intent, and drug involved. For nonfatal overdose data, we recorded the measure specification for published estimates and whether states performed any deduplication efforts or published mutually exclusive measure specifications to capture data on unique overdose events across care settings. We also recorded instances in which states published nonfatal overdose estimates from other data sources (eg, community members). Two analysts (C.E.J. and M.C.) independently reviewed each website to characterize states’ methods of capturing nonfatal overdose data. Each state validated the final characterization of all surveillance methods.
We calculated nonfatal-to-fatal overdose ratios for overdoses involving any drug and opioids. For each state–drug pairing, we created a range of ratios, with ED visits representing the lower bound and the cumulative total of additional data types published (ED visits, encounters with first responders, and other community responses) representing additional upper bounds. We used Microsoft Excel version 16 (Microsoft Corporation) to make calculations.
The Office of National Drug Control Policy determined the intent of this study was to improve public health surveillance for nonfatal drug overdose using publicly available information from state websites and, thus, did not involve human subjects and did not require institutional review board approval.
Results
Five states (Illinois, Maine, New Jersey, North Carolina, and West Virginia) met our inclusion criteria by publishing nonfatal overdose data from both EDs and first responders on their state websites. Illinois, Maine, North Carolina, and West Virginia used syndromic surveillance to track all nonfatal overdose-related ED visits, including nonfatal overdose events that resulted in hospital admission (Table 1). New Jersey used hospital discharge data to track nonfatal overdose-related ED visits defined as the number of patients who were treated and released and a separate indicator for overdoses that resulted in hospital admission (Table 1).
Data sources and measure specifications used by selected states to track nonfatal overdoses treated in hospital care settings, United States, 2021 a
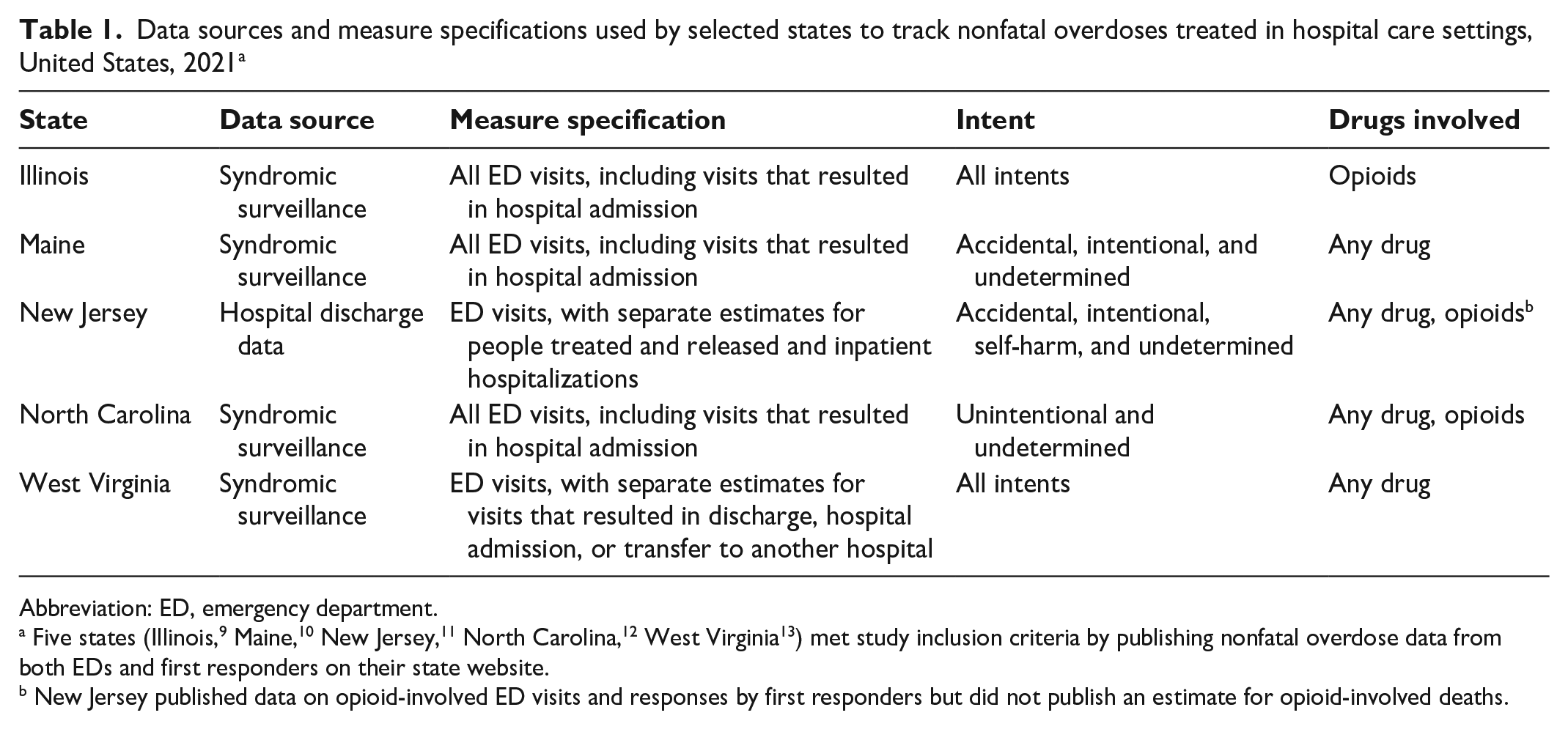
Abbreviation: ED, emergency department.
Five states (Illinois, 9 Maine, 10 New Jersey, 11 North Carolina, 12 West Virginia 13 ) met study inclusion criteria by publishing nonfatal overdose data from both EDs and first responders on their state website.
New Jersey published data on opioid-involved ED visits and responses by first responders but did not publish an estimate for opioid-involved deaths.
Illinois and West Virginia published the number of nonfatal overdose encounters with EMS (Table 2). Other states tracked encounters with first responders who reversed an opioid overdose following naloxone administration. New Jersey reported the number of overdose reversals following naloxone administration by EMS and state police. North Carolina tracked overdose reversals following naloxone administration by law enforcement through a voluntary reporting program. Maine tracked EMS encounters and overdose reversals following naloxone administration by law enforcement. Maine and North Carolina also published data on overdoses reversed by community members who administered naloxone.
Data sources and measure specifications used by selected states to track nonfatal overdoses treated in prehospital settings, United States, 2021 a
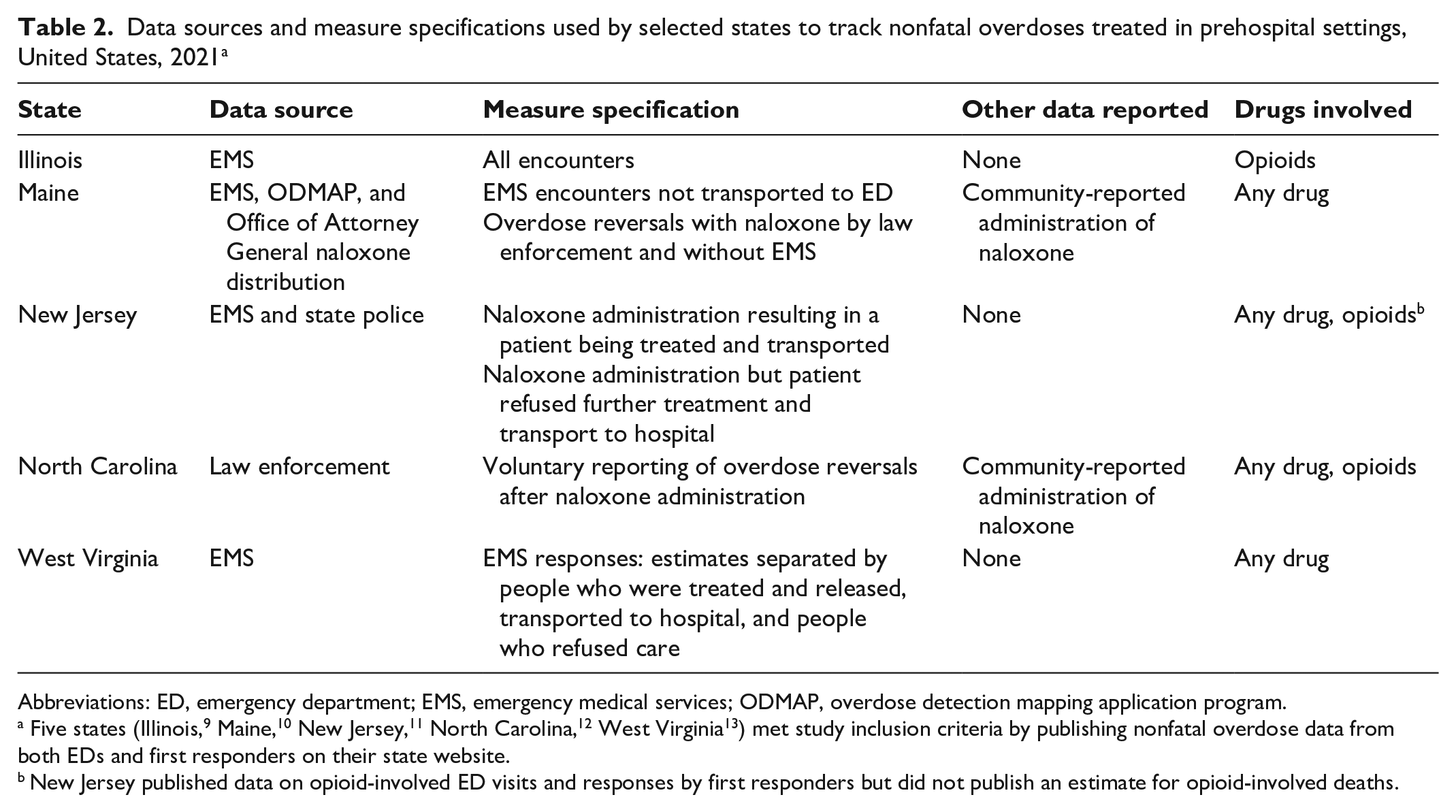
Abbreviations: ED, emergency department; EMS, emergency medical services; ODMAP, overdose detection mapping application program.
Five states (Illinois, 9 Maine, 10 New Jersey, 11 North Carolina, 12 West Virginia 13 ) met study inclusion criteria by publishing nonfatal overdose data from both EDs and first responders on their state website.
New Jersey published data on opioid-involved ED visits and responses by first responders but did not publish an estimate for opioid-involved deaths.
Maine and New Jersey reported performing data deduplication between multiple data sources (Table 3). Maine reported deduplicating overdose events treated by EDs, EMS, and law enforcement; however, they were unable to determine how many overdoses that were reversed by community members who administered naloxone also went on to receive treatment by other health care professionals or law enforcement. New Jersey also reported performing data deduplication of nonfatal overdoses after naloxone administration by EMS and state police. Maine, New Jersey, and West Virginia published detailed outcome information that made mutually exclusive measure specifications across care settings possible. For example, Maine published data on all ED visits, EMS encounters not transported to an ED, and overdoses reversed by law enforcement following naloxone administration without EMS. New Jersey published data on ED visits in which the patient was treated and released separately from ED visits in which the patient was admitted to the hospital and published data on naloxone administered by first responders by patient disposition (allowing New Jersey to differentiate between people treated and transported to a hospital and people who refused further treatment). West Virginia also published patient outcome information, which allowed the state to track all ED visits and EMS encounters in which the patient was not transported to a hospital.
States performing data deduplication or using mutually exclusive measure specifications to capture unique nonfatal overdose events across prehospital and hospital care settings, United States, 2021 a
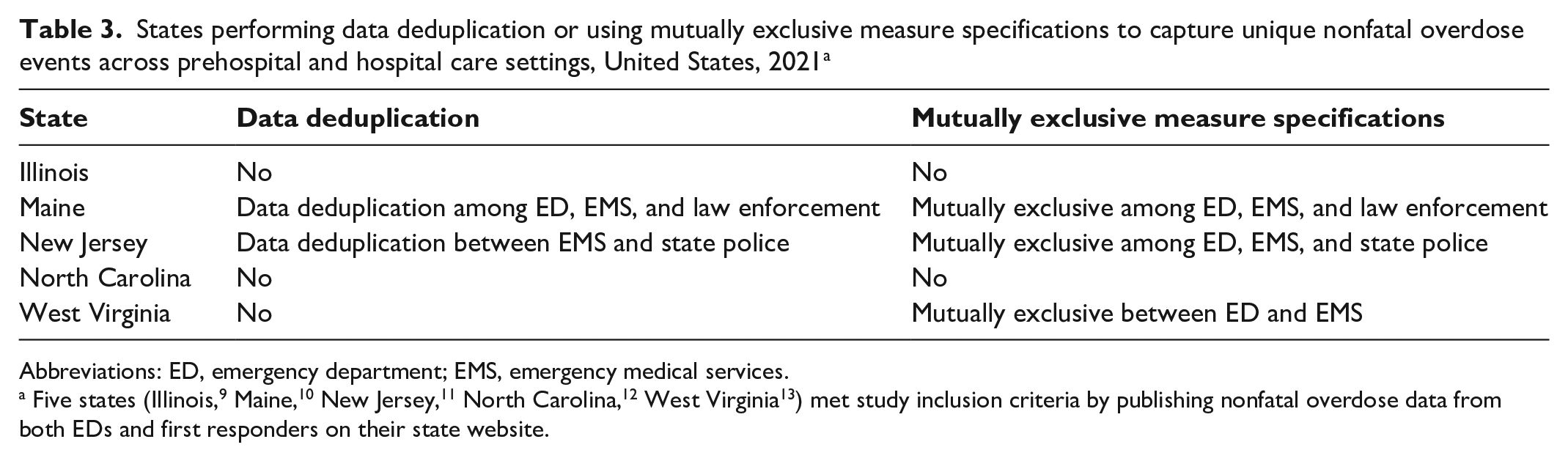
Abbreviations: ED, emergency department; EMS, emergency medical services.
Nonfatal-to-fatal overdose ratios varied by drug and measure specification. For states that published any drug-related overdose, Maine reported mutually exclusive measure specifications with a lower bound of 7.0 (nonfatal ED visits per fatal overdose) and an upper bound of 14.1 (nonfatal ED visits, nonfatal encounters with first responders, and overdoses reversed after naloxone administration by community members per fatal overdose) (Figure 1). West Virginia also reported mutually exclusive measure specifications with a lower bound of 5.2 (nonfatal ED visits per fatal overdose) and an upper bound of 7.5 (nonfatal ED visits and encounters with first responders per fatal overdose). When mutually exclusive measure specifications were not used, West Virginia’s upper bound ratio increased to 11.5. New Jersey reported mutually exclusive measure specifications with a lower bound of 6.3 (nonfatal ED visits per fatal overdose) and an upper bound of 7.0 (nonfatal ED visits and overdoses reversed after naloxone administration by first responders per fatal overdose). When mutually exclusive measure specifications were not used, New Jersey’s upper bound increased to 10.3. North Carolina reported non–mutually exclusive measure specifications with a lower bound of 4.2 (nonfatal ED visits per fatal overdose) and an upper bound of 5.2 (nonfatal ED visits, overdoses reversed after naloxone administration by first responders, and overdoses reversed after naloxone administration by community members per fatal overdose).
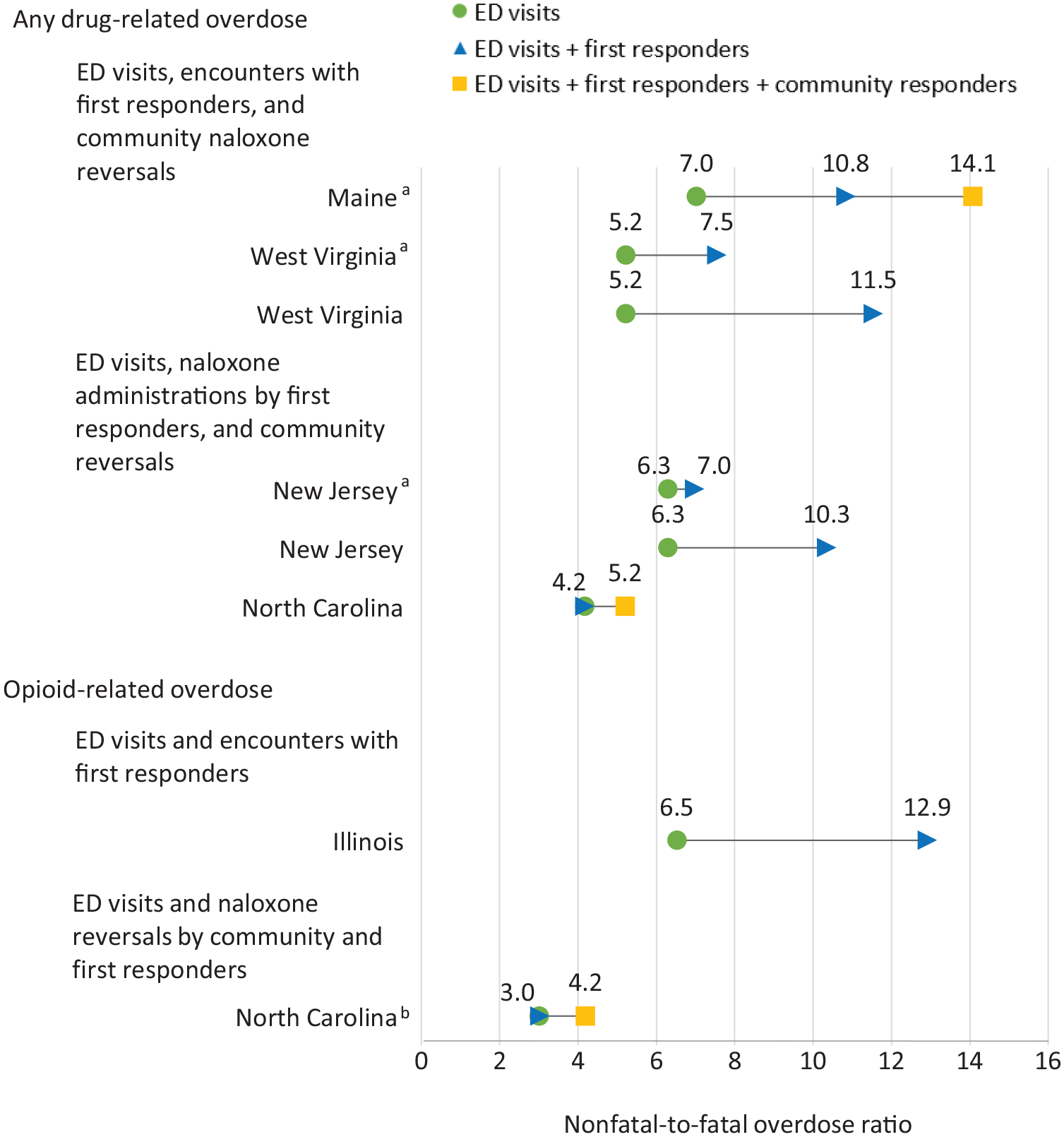
Nonfatal-to-fatal overdose ratios for selected states by drug, United States, 2021. Five states (Illinois, 9 Maine, 10 New Jersey, 11 North Carolina, 12 West Virginia 13 ) met study inclusion criteria by publishing nonfatal overdose data from both emergency departments (EDs) and first responders on their state website.
Illinois and North Carolina reported opioid-related nonfatal overdoses using non–mutually exclusive measure specifications. Illinois had a lower bound of 6.5 (nonfatal ED visits per fatal overdose) and an upper bound of 12.9 (nonfatal ED visits and nonfatal encounters with first responders per fatal overdose). North Carolina had a lower bound of 3.0 (nonfatal ED visits per fatal overdose) and an upper bound of 4.2 (nonfatal ED visits, overdoses reversed after naloxone administration by first responders, and overdoses reversed after naloxone administration by community members per fatal overdose).
Discussion
In the 5 states included in this study, we estimated that 5 to 14 additional nonfatal overdoses occurred for every fatal overdose. Evaluating these ratios can provide insights to assess the effectiveness of drug policies and programs and to efficiently target the distribution of resources for prevention, treatment, and harm reduction. Several factors can influence the ratio of nonfatal-to-fatal overdoses. For example, low ratios may indicate that few people are surviving drug overdoses, which could reflect an increasingly lethal illicit drug supply and/or low use of EMS or ED services because of capacity issues, stigma, or fear of legal consequences associated with calling 9-1-1. Increased access to naloxone within a community could also result in a low ratio because fewer nonfatal than fatal overdoses will be captured by traditional nonfatal overdose surveillance systems that rely on interactions with the health care system. On the other hand, high ratios may reflect a decreasingly lethal drug supply, a new emerging drug causing nonfatal overdoses but not yet large numbers of fatal overdoses, and/or an environment in which people are willing to call 9-1-1 and the state has the capacity to respond to overdoses and connect people to essential treatment, harm reduction, and recovery services.
Even among states that were comprehensively capturing and reporting fatal and nonfatal overdoses, we found substantial variation in data sources and the measure specifications used by states to publicly report nonfatal overdoses. Variation in these methods can influence the magnitude of nonfatal overdose estimates and make it difficult to compare overdose morbidity between state and local jurisdictions, hindering the ability of decision makers to efficiently distribute resources to areas most in need.
Four states relied on syndromic surveillance, and 1 state relied on discharge data to track nonfatal overdose-related ED visits. Within these data sources, variation was observed in the measure specifications used to estimate the number of ED visits for nonfatal overdoses. For discharge data, nonfatal overdose information is determined from the final diagnosis codes used to identify the reason for an ED visit for billing purposes; for syndromic surveillance, nonfatal overdose information is gathered from preliminary information before a diagnosis is confirmed and includes chief complaint free-text descriptions in addition to standard diagnosis codes. 14 Although syndromic surveillance can provide more timely estimates of nonfatal overdose compared with discharge data, this approach may overestimate the number of ED visits. Vivolo-Kantor et al 15 found that syndromic surveillance captured 67.8% more overdose visits from all drugs and 15.6% more opioid-involved overdose visits compared with hospital discharge data. The authors suggested that these findings may have been caused by an inability to remove data on admitted patients from syndromic surveillance data. In addition, the discrepancies may reflect differences in case definitions used for syndromic versus discharge data, such as the additional use of chief complaint free-text descriptions for syndromic surveillance.
For tracking encounters with first responders, 2 states used EMS, 1 state used law enforcement, and 2 states used both data sources. Within EMS encounters, variation was observed in the definitions used and whether the measure included all EMS responses or just a subset of responses based on a patient’s response to naloxone administration. Thus, states that track all encounters with first responders will have a higher estimate of nonfatal overdoses than states that track only naloxone administration resulting in overdose reversal.
Although states need to develop nonfatal overdose surveillance systems to help guide state and local decisions, having comprehensive, timely, and standardized nonfatal overdose surveillance data that are comparable between states can assist the federal government in distributing lifesaving resources. Inclusion of data from prehospital and hospital care settings can also provide local decision makers with improved nonfatal overdose estimates, which can help public health and public safety professionals detect and respond to spikes in overdose activity at the community level. 16
It is possible that states collect more information on drug overdoses than identified in our study. For example, a number of national surveillance systems currently track responses to overdoses in prehospital and hospital care settings. In hospital care settings, the Centers for Disease Control and Prevention’s Drug Overdose Surveillance and Epidemiology (DOSE) system and the Agency for Healthcare Research and Quality’s Healthcare Cost Utilization Project use standard definitions to collect hospital discharge data on inpatient stays and ED visits related to a drug overdose; however, not all states participate in these programs.17,18
In prehospital settings, the National Highway Traffic Safety Administration’s National EMS Information System (NEMSIS) Nonfatal Drug Overdose Dashboard collects near–real-time data in a standard format from approximately 95% of all EMS agencies in the United States that respond to 9-1-1 requests for emergency care. 19 These reports also capture information on naloxone administrations and whether the patient was transported to a medical facility. Other novel surveillance systems include the Overdose Mapping and Application Program, which provides near–real-time suspected overdose surveillance data to support public safety and public health efforts to respond to sudden increases in overdose events, and the National Poison Data System, which monitors all calls to poison centers in the United States.20,21
Increased state participation in national surveillance systems, in which reporting standards specified by CDC’s DOSE for hospital discharge data and NEMSIS for EMS data are used, would help decision makers more accurately compare nonfatal overdose estimates across state and local jurisdictions. Combining data from EMS and EDs would also improve our understanding of the true incidence of overdoses in the United States and enable decision makers to pinpoint the exact location where overdoses are occurring, rather than the location of the hospital where the person is being treated, which could inform treatment and prevention efforts. However, because these surveillance systems are capturing data on many of the same overdose events (eg, if a person is treated by EMS and then transported to an ED), combining data from these surveillance systems could result in a single event being counted multiple times, resulting in a substantial overestimate of the number of nonfatal overdoses occurring in the United States. For example, West Virginia reports that 61% of nonfatal overdose EMS encounters are treated and transported to a hospital. 13 If added together, these events would be double-counted by EMS and ED surveillance systems, highlighting the need for improved coordination between nonfatal overdose surveillance systems in prehospital and hospital care settings to identify unique overdose events. Unfortunately, data deduplication between these systems can be resource intensive and time-consuming because of challenges with data linkage in the absence of a unique patient identifier that can be used across the care continuum.
One potential solution to address challenges of data deduplication could be to develop mutually exclusive measure specifications to minimize the number of duplicate overdose events counted across care settings; this framework could provide decision makers with more accurate estimates of nonfatal overdoses to inform drug policies and programs (Figure 2). In hospital care settings, we propose reporting data for all ED visits, including people who are treated and released and people who are admitted to a hospital, using standardized hospital discharge data. In prehospital settings, we propose reporting data for nonfatal overdose EMS encounters not transported to a hospital. These data would include all EMS encounters and not just encounters in which the person received naloxone. Overdoses reversed with naloxone or other responses without EMS could also be reported to capture overdose events among people who do not receive medical attention, such as events reported by public safety agencies, poison control centers, harm reduction organizations, or other community programs. Data on fatal overdoses should be obtained from comprehensive vital statistics programs to supplement nonfatal overdose data and to inform the calculation of nonfatal-to-fatal overdose ratios. Maine and West Virginia currently publish data that enable mutually exclusive measure specifications in accordance with our proposed framework.
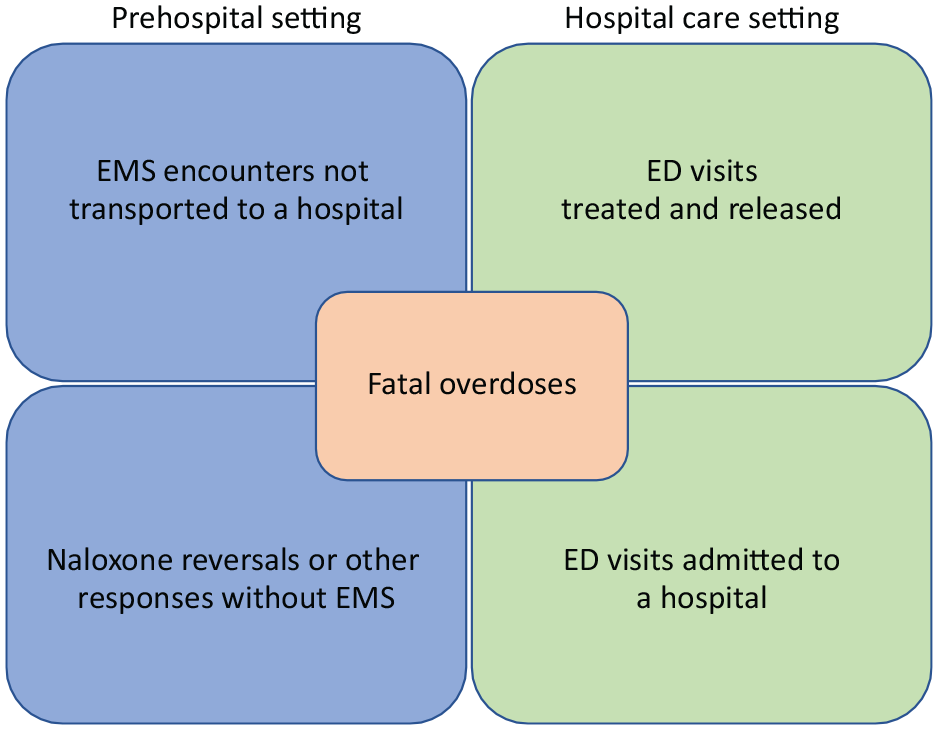
Example framework for tracking nonfatal overdose with mutually exclusive measure specifications. Abbreviations: ED, emergency department; EMS, emergency medical services. Opioid overdose reversals with naloxone administration or other responses without EMS could include data from public safety agencies, poison control centers, harm reduction organizations, or other community programs that track self-administration or administration by community members of naloxone.
We identified 3 additional challenges with reporting nonfatal overdoses during our review of drug overdose surveillance methods in US states. First, states and the federal government should make a concerted effort to update data fields in ED and first responder data systems when a response to an overdose becomes fatal. In phase 1, we found that most states use ED (n = 45 states) and first responder (n = 34 states) data to track nonfatal overdoses, but only about half of states that publish these data differentiate between fatal and nonfatal outcomes. 5 It is likely that first responders are unaware of patient outcomes once EMS intervenes or after the patient is transported to a hospital. Identifying methods of notifying and updating first responder data systems could help produce more accurate nonfatal overdose estimates. Improved data sharing between EMS and ED information systems is also needed so that hospitals can accurately document patient diagnoses and the emergency care services received by patients before patient arrival to the hospital. Second, we observed variations in states’ nonfatal drug overdose definitions regarding the intent of an overdose. In the hospital care setting, some states reported nonfatal overdose–related ED visits resulting from overdoses of unintentional or undetermined intent, whereas other states reported nonfatal overdoses of all intents (including intentional overdoses [eg, self-harm]). In addition, this information may not be documented in other data systems from the prehospital setting. To ensure measures are reported consistently and are comparable between jurisdictions, states should follow reporting standards specified by CDC’s DOSE for hospital discharge data and NEMSIS for EMS data. The third challenge relates to the identification of specific drugs involved in an overdose. Rapid drug testing equipment may not be available for EDs and EMS to determine the drugs involved at the scene of a presumed overdose. Symptom improvement following naloxone administration can be used as a proxy to identify the presence of an opioid but would not provide insight on other potential drugs involved (such as stimulants).
Practice Implications
Improving nonfatal overdose surveillance systems has important implications for detecting and responding to spikes in overdose activity, and nonfatal overdose surveillance systems can be used to inform the distribution of lifesaving resources throughout the United States. However, further standardization is needed between state and local jurisdictions to enable consistent and comparable nonfatal overdose estimates.
If nonfatal overdose data from prehospital and hospital care settings were able to be combined in a standard format to produce more accurate estimates, decision makers could use this information in conjunction with fatal overdose data to more accurately assess and predict overdose events and identify areas most in need of essential services in a timely manner. In 2021, our analysis indicates that EDs, first responders, and community members responded to 5 to 14 additional nonfatal overdoses for each fatal overdose that occurred. Given that nonfatal overdose is a key risk factor for subsequent fatal overdose, each nonfatal overdose represents an opportunity to intervene and save a life.2-4
Footnotes
Acknowledgements
The authors thank staff members at the Maine Drug Data Hub, the State of New Jersey Department of Health, the North Carolina Department of Health and Human Services, the Illinois Department of Public Health, and the West Virginia Office of Drug Control Policy who reviewed our characterization of their methods for capturing data on nonfatal overdose. They did not receive compensation for these contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.