
Abstract
Introduction:
With the goal of eliminating hepatitis C virus (HCV) as a public health problem in Washington State, Public Health–Seattle & King County (PHSKC) designed a Hepatitis C Virus Test and Cure (HCV-TAC) data system to integrate surveillance, clinical, and laboratory data into a comprehensive database. The intent of the system was to promote identification, treatment, and cure of HCV-infected persons (ie, HCV care cascade) using a population health approach.
Materials and Methods:
The data system automatically integrated case reports received via telephone and fax from health care providers and laboratories, hepatitis test results reported via electronic laboratory reporting, and data on laboratory and clinic visits reported by 6 regional health care systems. PHSKC examined patient-level laboratory test results and established HCV case classification using Council of State and Territorial Epidemiologists criteria, classifying patients as confirmed if they had detectable HCV RNA.
Results:
The data enabled PHSKC to report the number of patients at various stages along the HCV care cascade. Of 7747 HCV RNA-positive patients seen by a partner site, 5377 (69%) were assessed for severity of liver fibrosis, 3932 (51%) were treated, and 2592 (33%) were cured.
Practice Implications:
Data supported local public heath surveillance and HCV program activities. The data system could serve as a foundation for monitoring future HCV prevention and control programs.
An estimated 4.1 million adults in the United States had previously been or were currently infected with hepatitis C virus (HCV) during 2013-2016. 1 The number of persons with acute HCV infection increased about 3.5-fold from 2010 to 2016 (from 850 to 2967 reported cases), largely reflecting the rising rate of injection drug use and, to a lesser extent, improved case detection. 2 In the United States, the number of persons with chronic HCV infection is increasing and is most prevalent among persons born during 1945-1965 (ie, baby boomers). Because most currently infected persons were unknowingly exposed decades ago, morbidity and mortality are expected to increase in the coming decades. 3 Given the increasing prevalence of HCV infection, the Centers for Disease Control and Prevention (CDC) and the US Preventive Services Task Force recommend that baby boomers receive a 1-time HCV antibody test to identify HCV infection (hereinafter, birth-cohort testing). 4,5
In the context of the high burden of chronic HCV infections and the availability of highly effective therapies, a challenge is to identify infected persons and link them to care and treatment. Public health departments can facilitate case identification and linkage to care; however, existing databases often lack longitudinal laboratory and clinical data. These data gaps result in problems with determining whether a report is confirmed, probable, or not a case, and they limit health departments’ ability to determine whether patients have been linked to care, treated, or cured. To address these gaps, Public Health–Seattle & King County (PHSKC) developed a comprehensive HCV surveillance system. We provide an overview of the development of this system—its design, data collection strategies, database, and analytic issues—with a focus on how the data are being used to monitor trends and address gaps in the progression from HCV diagnosis to treatment and cure (hereinafter, the HCV care cascade) in Seattle–King County, Washington.
Materials and Methods
Surveillance Program and Data System
The CDC-supported PHSKC Hepatitis C Virus Test and Cure (HCV-TAC) program was originally funded from September 30, 2014, through September 29, 2018, and comprised 9 entities: PHSKC; the Hepatitis Education Project, an organization that provides hepatitis testing, educational outreach, and medical case management services 6 ; the University of Washington; and 6 community-based clinical sites in King County (Neighborcare Community Health Centers, HealthPoint Community Health Centers, Country Doctor Community Health Centers, Swedish Medical Center, Harborview Medical Center, and Kaiser Permanente Washington).
The 4 goals of HCV-TAC were to (1) increase and monitor the number of persons at risk for HCV infection who are tested, receive care and treatment, and are cured; (2) increase primary care providers’ capacity to diagnose and cure HCV infection through the expansion of a telehealth HCV clinical training network (Project ECHO [Extension for Community Healthcare Outcomes] 7 ) and online training for health care providers 8 ; (3) establish networks of HCV specialists and primary care providers to develop and implement services for subpopulations with high rates of HCV infection; and (4) support and evaluate efforts to reduce HCV infections and provide best practices that can be applied elsewhere.
During the program period, we integrated surveillance, clinical, and laboratory data into a comprehensive database that supported the program’s objectives. PHSKC used these data to monitor HCV incidence in King County, enhance HCV testing efforts among target populations, track progress in the care cascade, and support patient linkage to care.
Data Sources
Acute HCV infection and chronic HCV infection are nationally 9 and locally 10 notifiable diseases. All health care providers and laboratories in Washington State are legally required to report cases to public health departments. PHSKC’s data system integrated (1) hepatitis case reports received via telephone and fax from health care providers and laboratories (beginning in 2000, these reports were entered into a local legacy database), (2) hepatitis test results reported via electronic laboratory reporting (ELR) to the Washington State Department of Health (WA DOH), and (3) laboratory and clinic visit data reported by the 6 HCV-TAC clinical sites.
Data System Design
PHSKC redesigned its legacy database to improve the timeliness and completeness of reporting. Historically, clinicians and laboratories submitted hepatitis case reports via telephone and fax. Administrative staff members manually entered these reports as well as reports from the WA DOH ELR web portal into the legacy database. Because of resource constraints (eg, demands on staff time), PHSKC generally entered only initial case reports for patients into the legacy database (ie, patients without an existing hepatitis B or hepatitis C record, based on a search of the patient’s last name, first name, and date of birth). To minimize the administrative burden of manual data entry and ensure more complete capture of data from laboratory reports, beginning in 2014, HCV-TAC program staff members worked with the King County Information Technology Department (hereinafter, IT Department) to redesign the hepatitis module of the legacy database.
PHSKC modified the legacy database from an incident-based structure (ie, 1 record per acute and chronic HCV infection event) to a person-based structure (ie, 1 record per person, with shared demographic, laboratory, and clinical data across hepatitis events). To achieve this structural modification, PHSKC mapped data elements from ELR and clinical sites to elements in the modified surveillance database. The IT Department created new fields to accommodate laboratory elements that did not previously exist in the database, including collection dates and ordering facility/provider information for each laboratory result. We designed a relational interface to display multiple laboratory reports per person over time and information captured across multiple health care visits per person, and we de-duplicated records in the legacy database to derive a single demographic record per person. The IT Department created a person-history table to preserve changes to data on patients’ demographic characteristics over time.
The redesigned database (completed in 2018) enabled PHSKC to automatically import hepatitis laboratory reports from the WA DOH ELR system and partner laboratory and clinical data, eliminating the need for manual data entry. Algorithms compare data on patient demographic characteristics from incoming reports with existing patient records. Incoming data for patients matching an existing record (ie, with a matching score above a defined threshold) are appended to that record. A new record is created when it is determined that a patient does not already exist in the database (ie, with a matching score below a defined threshold). The system holds records deemed ambiguous matches for manual review and de-duplication.
Target Populations
PHSKC designed the HCV-TAC program in 2013 to serve target populations disproportionately affected by HCV. The 6 health care facilities that partnered with the HCV-TAC program serve an estimated 140 000 of 520 000 (27%) baby boomers in King County. PHSKC selected these clinical sites to serve a broad geographic and demographic distribution of HCV patients. Three of the clinical sites (HealthPoint, Neighborcare, and Country Doctor) are federally qualified health centers (FQHCs) and are the largest providers of primary medical and dental care in Seattle for low-income and uninsured patients; in 2014, roughly 30% of patients at each site were uninsured. 11 Many FQHC patients were recent immigrants, and the population was racially and ethnically diverse (in 2014, racial and/or ethnic minority groups accounted for 67% of patients at HealthPoint, 60% of patients at Country Doctor, and 70% of patients at Neighborcare). 11 Harborview Medical Center is an urban public hospital primarily serving medically underserved patients, including immigrants, persons who inject drugs, and persons with HIV. Harborview’s Hepatitis and Liver Clinic is the largest provider of HCV care in the Pacific Northwest. Swedish Medical Center comprises 5 hospitals and 100 clinics in King County, including a liver transplant program, and serves more than 100 000 King County primary care patients. Kaiser Permanente is a not-for-profit health plan that serves more than 200 000 residents in King County, including Medicaid and uninsured patients. All HCV-TAC clinical sites allow HCV treatment for current substance users.
During the program period, the 6 HCV-TAC clinical sites submitted data for King County patients who were (1) known to have HCV infection, defined as the presence of a record documenting a previous clinical HCV diagnosis, a positive HCV laboratory test result (antibody, RNA, or genotyping), or history of being treated for HCV infection; (2) born during 1945-1965, tested for HCV infection, and HCV antibody negative; and (3) born during 1945-1965 and did not have records of HCV testing. In 2013, PHSKC instructed clinical sites to reach back as far as possible in their electronic health records (EHRs) to determine eligibility for each subset; sites reported identifiers only for patients known to have HCV infection.
Frequency and Format of Data Collection
Clinical sites submitted historical data to PHSKC that dated back to January 1, 2013, and began quarterly reporting of laboratory and clinical data in 2015. Because of administrative delays in finalizing laboratory results and billing diagnoses, some sites had up to a 4-month lag in transmitting complete quarterly data.
WA DOH transmitted hepatitis data to PHSKC reported through its ELR system in Extensible Markup Language (XML) format on a weekly basis. These data included all King County laboratory reports submitted to WA DOH (ie, not restricted to the 6 HCV-TAC clinical sites). PHSKC asked clinical sites to report data in XML file format to ensure uniformity in data submission and allow the IT Department to upload data without creating a separate upload process for each site. The IT Department uploaded historical ELR data to the modified database dating back to January 1, 2013. Laboratories not yet participating in ELR submitted hepatitis reports to PHSKC by fax daily; PHSKC administrative staff members manually reviewed data on patient demographic characteristics to determine whether cases had been previously reported and manually entered laboratory reports into the modified database.
Data Elements in the Modified Database
Laboratory reports for HCV patients included the following results, where available: HCV antibody tests (positive results only), HCV antibody detection signal-to-cutoff ratio (which helps identify true-positive results), all qualitative and quantitative HCV RNA test results (including negative and indeterminate findings), HCV genotype, liver enzyme tests (including alanine aminotransferase [ALT], aspartate aminotransferase [AST], and platelets), all FibroSure results (which measure level of scarring to the liver, including necroinflammatory activity score and grade and fibrosis score and stage), and positive hepatitis A and hepatitis B serology results. Beginning in 2013, PHSKC asked laboratories to submit only ALT, AST, platelets, and hepatitis A/hepatitis B serology results ordered on the same day or within 1 month of a positive hepatitis C test, if possible, because providers may have ordered these tests for reasons other than managing HCV care.
The 6 HCV-TAC clinical sites extracted patient encounter data from their EHRs for quarterly submission to PHSKC. These files included the following data elements: name, birthdate, social security number, visit date, provider, clinic, patient’s health insurance at that visit, comorbidities listed at that visit, treatment history, medical history, assessment notes, plan notes, HCV medications the patient was currently taking or prescribed at that visit (including start/stop dates), and treatment outcome (eg, achieved cure, treatment failure, treatment discontinued, lost to follow-up). For the subset of patients identified by the clinical sites who tested negative for HCV, and for those who had never been tested, de-identified visit-level data consisted of visit date, provider, clinic, race, ethnicity, and county of residence. These data were not attached to a patient’s records in the database. Sites with multiple clinic locations queried all locations for HCV-related visits at that site to identify patients.
Case managers and disease investigators entered data on patient encounters into the modified database, including the aforementioned laboratory and clinical data elements (if not already recorded) and dates and times of case management outreach attempts and outcomes (eg, lost to follow-up, linked to care, already in care, refused care, not actively infected, out of jurisdiction, deceased, not eligible for case management, in process).
Data Analysis and Reporting
PHSKC epidemiologists analyzed the HCV-TAC data at least quarterly by using SAS version 9.4. 12 They parsed laboratory data using Logical Observation Identifiers Names and Codes and local codes to identify the type of hepatitis tests conducted. Using a hierarchical combination of Systemized Nomenclature of Medicine and local result codes, epidemiologists classified result values across disparate fields (eg, abnormal result flags, text queries, and numerical values) to a standardized format. They transformed the data to display all tests performed per patient over time as a single observation. PHSKC established case classification according to the current Council of State and Territorial Epidemiologists criteria 13 by examining data on laboratory and clinical results extracted from the patient’s entire medical record. PHSKC classified patients as confirmed if they had detectable HCV RNA. PHSKC identified potential acute HCV cases based on a newly positive HCV antibody test combined with elevated ALT/AST results. To help differentiate between acute HCV infection and chronic HCV infection, PHSKC staff members contacted the ordering provider and reviewed health records to identify the reason for testing and applicable risk factors.
PHSKC reported de-identified patient-level data to CDC quarterly for monitoring and evaluation of the project. PHSKC monitored patient progress on the HCV care cascade, including confirmatory RNA test results, staging (genotype test or fibrosis staging test), treatment start date, treatment completion, and 12-week posttreatment testing for cure. PHSKC classified patients as cured based on an HCV RNA negative result at ≥12 weeks posttreatment or based on reporting of cures in the clinical data. Epidemiologists analyzed discrepancies between laboratory data and clinical data to determine patient outcomes (ie, infected, cured, or reinfected) based on the timing of the report.
PHSKC created quarterly reports for the 6 participating health care clinics that summarized their HCV patient populations and proportion at each step of the HCV care cascade and provided patient-level reports to sites to help identify patients requiring linkage to care or other clinical follow-up.
To evaluate each clinic’s performance with birth-cohort HCV testing, PHSKC created a data set representing all clinic visits and associated laboratory results among the entire birth-cohort population. We identified patients with at least 1 primary care visit during a specified period (denominator), and we used laboratory data to determine the percentage of these patients screened for HCV antibody before or during that period (numerator). Epidemiologists used these data to calculate the percentage of screened birth-cohort members for each site and at all sites combined over time.
Results
PHSKC’s legacy database was poorly suited for chronic HCV surveillance: it lacked key laboratory, clinical, and demographic data elements for identifying and tracking HCV cases longitudinally during multiple clinical encounters (Table).
Attributes of Public Health—Seattle & King County’s data system for hepatitis C surveillance, clinical, and laboratory data before and after implementation of the Hepatitis C Virus Test and Cure (HCV-TAC) programa
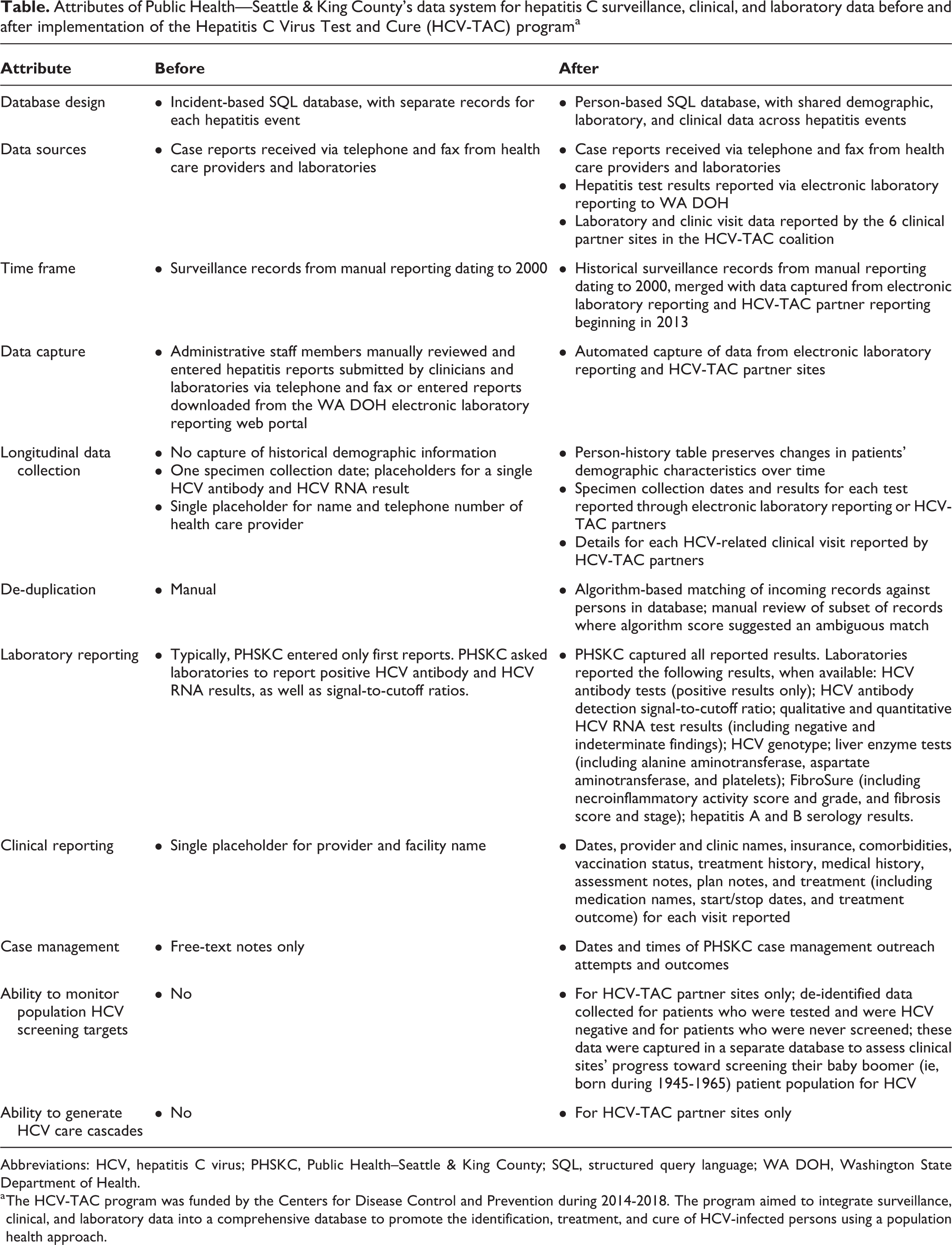
Abbreviations: HCV, hepatitis C virus; PHSKC, Public Health–Seattle & King County; SQL, structured query language; WA DOH, Washington State Department of Health.
a The HCV-TAC program was funded by the Centers for Disease Control and Prevention during 2014-2018. The program aimed to integrate surveillance, clinical, and laboratory data into a comprehensive database to promote the identification, treatment, and cure of HCV-infected persons using a population health approach.
Importing all hepatitis test results reported to WA DOH via ELR into the modified database improved PHSKC’s ability to identify cases relative to the legacy database. PHSKC identified a cumulative 22 814 confirmed cases of HCV infection in King County that were manually entered into the database from January 1, 1991, through July 31, 2018. From January 1, 2013, through July 31, 2018, PHSKC identified an additional 3727 confirmed cases by automatically uploading the state’s hepatitis ELR data into the modified database. Because of efforts by WA DOH to improve ELR, combined with HCV-TAC efforts asking participating laboratories to report additional hepatitis results, the proportion of HCV laboratory test results reported through ELR increased annually from 2013 to 2017. The percentage of hepatitis laboratory results received by PHSKC each year that were reported through ELR was 60% in 2013, 65% in 2014, 69% in 2015, 82% in 2016, and 94% in 2017.
The retrospective collection of laboratory data from HCV-TAC partners enhanced the completeness of case identification. We identified 1045 confirmed cases of HCV infection from partner data that we did not identify via manual reporting from laboratories and health care providers or ELR from January 1, 2013, through July 31, 2018. Some reports were from partners that were not yet participating in ELR at the start of the project.
PHSKC used its modified data system to describe changes in HCV screening longitudinally (eg, the percentage of screened patients in the birth cohort). The data system also enabled us to create a care cascade to assess the percentage of patients diagnosed, staged, genotyped, prescribed treatment, and cured among our partner sites. Of 27 586 confirmed cases of HCV infection in King County, 7747 (28%) were seen at our partner sites and were HCV RNA positive. Of these 7747 confirmed cases, 5377 (69%) had genotype or fibrosis staging results, 3932 (51%) were prescribed HCV treatment based on clinical data, and 2572 (33%) were cured at ≥12 weeks after the estimated completion of treatment.
Discussion
The US National Viral Hepatitis Action Plan for 2017-2020 calls for the elimination of viral hepatitis and development of robust surveillance and health information systems 14 for evaluating trends in HCV case identification and cure. The PHSKC HCV-TAC data system enhanced the completeness and usefulness of population-level HCV surveillance data, allowing PHSKC to monitor HCV testing and treatment targets in King County. These data enabled PHSKC to determine how many patients were screened for HCV and the percentage who were infected, staged, treated, and cured. The data also allowed PHSKC to evaluate longitudinal changes relative to baseline (the start of the project in 2013). These analyses were not feasible before implementing this data system. PHSKC continues to collect data and support analyses using the data system beyond the original funding period, which ended in 2018. This information will enable PHSKC to identify disparities in HCV diagnosis, initiation of treatment, and treatment outcomes and to develop targeted interventions.
An additional benefit of the data system was that provision of reports created by PHSKC to facilitate monitoring and coordination of clinical care increased collaboration with clinicians caring for HCV-infected persons. The integration of data received from multiple health care facilities and laboratories in King County into a single database has aided epidemiologists, clinicians, and case managers, who would otherwise be required to extract data from multiple systems to obtain comprehensive patient summaries necessary for monitoring progress through the chronic HCV infection care cascade.
Limitations
This system had several limitations. Differences in the way each clinical site’s EHR captures information created challenges in data ascertainment and interpretation. First, providers do not record some information reliably or in a standardized format, including history of substance use or HCV treatment, and sometimes this information can be found only in free-text notes, not structured fields, depending on the EHR. Second, treatment start dates in EHRs generally represent dates on which providers ordered prescriptions, not necessarily the date on which the first dose was taken, and providers do not consistently document treatment end dates in structured fields. The treatment end date is currently considered important for assessing treatment outcomes because guidelines state that HCV RNA must be undetected at ≥12 weeks after treatment is completed to establish whether the patient was cured. When the start date and end date for a derived treatment are incorrect, a treatment outcome may be misclassified. Lastly, information on the clinical stage of liver disease based on methods such as AST to Platelet Ratio Index, FibroSure, liver biopsy, and Fibroscan results may be available only as scanned documents and cannot be queried directly during data extraction. Some sites extracted staging data manually from scanned documents; however, this activity is likely unsustainable because it requires trained reviewers and is resource intensive.
Another limitation of our data system was that fewer than one-third (7747 of 27 856; 28%) of all confirmed patients with HCV infection in King County were seen at one of our partner sites. Funding for this project allowed us to collect clinical data from only a subset of regional health care facilities, which limited our ability to identify all patients who had been treated and subsequently cured in King County. Although it is technically feasible to recruit additional sites to submit clinical data, doing so would require resources for onboarding expenses (eg, for structural and content validation), which is a barrier to system expansion. Public health jurisdictions that are unable to capture clinical data for surveillance can rely on laboratory data alone to identify patients requiring linkage to care (eg, patients with a positive HCV RNA result who do not have HCV staging laboratory results) and to monitor for markers of cure (eg, a positive HCV RNA result followed by a negative HCV RNA result after a minimum of 12 weeks). Approaches and limitations of using proxy measures to measure treatment outcomes have been described previously. 15,16 More than 30% of patients seen at HCV-TAC partner sites (1360 of 3932) who started treatment did not have follow-up HCV RNA results ≥12 weeks after their estimated treatment completion date; as such, the percentage of patients identified as cured was likely underestimated.
Lastly, because PHSKC collected only de-identified data for HCV antibody–negative patients and patients never tested for HCV, there were limitations in assessing birth-cohort HCV screening. The lack of patient identifiers means that PHSKC cannot de-duplicate data across sites or against existing surveillance records to identify persons screened elsewhere, which may result in an underestimation of the proportion of the population screened for HCV.
Practice Implications
Historically, laboratories and health care providers reported cases of acute and chronic HCV infection to PHSKC by telephone and fax. Because of the large volume of reports and limited resources, staff members entered only first reports for cases of HCV infection into PHSKC’s legacy surveillance database. The CDC-funded HCV-TAC program enabled PHSKC to modify its public health surveillance database to incorporate data from ELRs and clinical data extracted from EHRs. Integrating these data sources provided additional information about confirmatory testing, staging, and treatment response, which PHSKC was not previously able to identify. Combined with clinical visit information that was previously available only through labor-intensive medical record review, the redesigned database facilitates optimal public health, health care system, and clinical management of chronic HCV infection to improve population health and to support ongoing local HCV elimination program needs. This system has the potential to serve as the foundation for monitoring future HCV prevention and control programs.
Footnotes
Acknowledgments
The authors acknowledge Wendy Inouye, Meagan Kay, and Shelly McKeirnan of PHSKC, who provided key input and direction about the design of the HCV-TAC data system, and Casey Cassidy at the King County Information Technology Department for project management support. The authors also thank staff members at HCV-TAC partner sites who worked on data extraction and transformation, including Ron Johnson (Kaiser Permanente); Vasyl Aleksenko, Yan Bai, Maria Taasan-Baradi, and Troy Hanninen (Swedish Medical Center); Frederick Dowd, Christine Fong, Steve Senter, and Scott Terry (Harborview Medical Center); and Eric Grendell, Adam Ledvina, and Jerry Wilkinson (PTSO of Washington). The authors also thank staff members at the Washington State Department of Health, including Andrea Agnesani, Rita Altamore, Amanda Jones, Amy Liu, Nancy Stone, and Melissa Turner, for providing hepatitis laboratory results extracted from the state’s ELR system, offering guidance about use of the data, and accommodating requests aimed to improve surveillance and reporting.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was provided by the Centers for Disease Control and Prevention (CDC; grant 6 NU 51PS004601). The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.