
Abstract
Abstract Background Hepatitis C virus (HCV) infection is the most common bloodborne infection in the U.S. However, only a small proportion of persons are treated and cured. Previous research has not characterized sociodemographic characteristics of who receives treatment. We examined predictors of undetectable for HCV in Orange County, the sixth largest county in the United States, where HCV is the most commonly reported infection. Methods: From 2014 to 2020, we acquired public health surveillance data from 91,165 HCV antibody-positive care encounters from the California Reportable Disease Information Exchange (CalREDIE). We used a time-to-event proportional hazards framework to estimate individual and area-level correlates of time-to-HCV undetectable viral load among HCV + individuals. Results: Older adults (>65 years) showed an increased hazard of undetectable viral load relative to younger adults (HR = 2.00). In addition, residents of census tracts with greater enrollment in health insurance showed a greater likelihood of undetectable viral load (HR = 1.36). The moderating effect of higher tract median household income and higher tract levels of health insurance were more likely to have undetectable viral load and was statistically significant. Conclusion: In a large urban county, HCV antibody-positive older adults appear much more likely to show undetectable viral load compared to younger adults. Residents in areas with higher quartiles of health insurance enrollment have an increased likelihood of undetectable viral load. The extent to which constraints impede HCV care requires further investigation, including follow-up studies on health insurance type to test the relationship of health insurance type to undetectable viral load.
Background
According to the Centers for Disease Control and Prevention (CDC), the incidence of hepatitis C (HCV) in the United States has steadily increased since 2013 with an estimated 2.4 million individuals living with the virus.1–3 Hepatitis C is an infectious virus and the most common bloodborne pathogen in the U.S. If left untreated, the HCV virus can cause cancer and liver-related death increased liver fibrosis, and a higher risk of all-cause morbidity and mortality.2,4–7 In California, the CDC estimates a crude mortality rate of HCV in of 4.98 deaths per 100,000 people in 2018.
HCV Diagnosis and Care Cascade
Tracking patients through initial HCV diagnosis to treatment is done through a care cascade. This care cascade involves initial HCV infection diagnosis, treatment evaluation, treatment initiation, and treatment completion.8–13 With successful treatment leading to a sustained virologic response (SVR) with the virus remaining undetectable 12 weeks post-treatment completion.8–13 Although generally accepted as the standard of care, the care cascade may vary by treatment facility and clinician. This cascade is crucial because it identifies where patients can drop out of HCV care and assists public health practitioners in defining denominators for analysis using the number of patients in that part of the care cascade.
Diagnosis of HCV is imperative for patients to receive care. To diagnose HCV infection, patients must complete antibody testing and a subsequent viral load test to confirm viremia or chronic infection. Active infection of HCV is only confirmed using a viral load test. 14 The recommended diagnosis procedure begins with an HCV antibody enzyme-linked immune absorbed assay (ELISA) test with a follow-up RNA viral load test with viremic patients referred to treatment.15,16
A viable cure for HCV is available. In 2014, the Food and Drug Administration (FDA) approved the first wave of Direct Acting Antivirals (DAAs), curing the disease in as few as eight weeks with a likelihood of reinfection post-SVR.13,17–24 Numerous studies have shown that these DAAs are over 95%% effective.8,17,21,23–26
Although DAA medications are effective, their cost (ranging from $24,000 to $100,000) is a barrier to utilization, preventing infected individuals from seeking treatment.27–30 Insurance coverage of these medications should be examined to understand their independent and multiplicative effect on attaining an undetectable viral load.
Orange County, California, is the sixth most populous county in the U.S. with a population of 3.3 million. 31 The morbidity and mortality from hepatitis C infection in Orange County is substantially greater than any other infectious disease in the last decade (excluding the recent COVID-19 pandemic.)12,32
Despite the availability of effective treatment, it remains unclear what fraction of Orange County, California (O.C.) with an antibody-positive test, the sociodemographic determinants of who ultimately receives treatment are not well-characterized due to gaps in surveillance data. Other studies have not examined undetectable viral load using public health surveillance data in the U.S. and have only examined effectiveness of point of care testing on viral load.33–37
To better understand the infection rates in O.C. and how it relates to HCV testing, we examine the relationship between the individual (age, gender, out of state status) and area-level factors (census-tract level median income and insurance coverage) and the likelihood of an undetectable viral load for HCV.
Methods and Data Sources
Study Population
Participants in this dataset included 23,950 HCV antibody positive patients (and 91,165 patient encounters) in the (California Reportable Disease Information Exchange) CalREDIE infectious disease report database.
Sampling and Sampling Procedure
This dataset was a convenience sample compiled from all HCV antibody positive case reports assigned to O.C., California from January first, 2014, to March first, 2020. 12 Each person was counted individually and each test result categorized a as a different encounter. Out of the 159 to 140 total encounters, 91,365 were able to be joined to census tracts and 91,165 had no missing variables. that could be joined using census tract information to American Community Survey 2017 data. A sample diagram can be found in appendix A.
Sample Size Determination
This dataset was compiled from all hepatitis C antibody positive results from CalREDIE from 2014 to March first, 2020. All HCV viral load tests, regardless of the result, are reported to CalREDIE. Power calculations were conducted and there was an appropriate sample size to perform this analysis with 0.80 power according to the statistical software. 38
Data Collection Procedure
Data were extracted through CalREDIE's data warehouse for all those who tested antibody positive for hepatitis C
39 This research received approval from the Institutional Review Boards of the University of California, Irvine protocol H.S. # 2019-548 and the O.C. Health Care Agency (OCHCA)
Data Analysis
The dependent, or time-to-event variable is an undetectable viral load. An undetectable viral load was classified as having less than 20 copies/ml on a PCR RNA viral load test. 40 A sensitivity analysis was conducted with different viral load cut-offs to determine an undetectable viral load that could lead to sustained virologic response or natural clearing of HCV infection 40 We measured history of HCV infection by extracting data from the CalREDIE database for patients assigned to the OCHCA who tested positive using a HCV antibody test; cases with addresses outside of California were designated out of state.
We specified a Cox proportional hazard model, and the time period for evidence of undetectable viral load was by year. This regression uses time over multiple individual encounters per person to control for it in analysis and helps to see what the hazard of an event (in this case, whether an undetectable viral load) will happen. 41 The hazard function, in this case, is the “risk” of having an undetectable viral load at time t.40,41 In this dataset, there were 23,950 people with 91,165 total encounters as panel data. The unit of analysis is by person. The proportional hazards assumption using Schoenfeld residuals was not met so we cannot assume that the hazards are the same for every individual in this regression, 38 however these results are still insightful and can be used to better target public health interventions.
Independent variables at the individual level included age, gender, and in/out of state status. The coding for gender was categorical as collected (male, female, or unknown) and recoded into binary, male, or female. Age was divided into 10-year age groups after the age of 19 also as binary (65 and younger and over 65 years of age). 19 Due to 80% of missing race/ethnicity data in this dataset, we did not examine this covariate in these analyses.
Observations with census tract information were joined with data from the 2017 American Community Survey (ACS) (n = 23,950 or 73%). The 2017 ACS was used as it was the most recent ACS 5-year estimate conducted at the time of analysis. This matching allowed us to examine the role of median household income and % of residents with health insurance with an undetectable HCV viral load. Health insurance was further divided into % with private health insurance, % with no health insurance, and government health insurance (state or federal, Medicaid or Medicare.) 42 These data were aggregated into quartiles to be consistent with the literature and to better understand the wealth as distributed. 43 Data were analyzed using Stata version 13 (StataCorp, College Station, TX).
Results
The mean age was 52.47 years (± 15.20, min: 0, maximum of 119) (Table 1). Participants were mostly male (58.66%), and 20.47% of participants were over 65 years. California residents comprised 98.25% of the sample and the remaining 1.83% were out of state. A total of 259 individual patients (1.08%) showed an undetectable viral load at any time between 2014 and 2020.
Sociodemographic and Descriptive Characteristics of Individuals with HCV Antibody Positive Encounters Encounters in Orange County, California from 2014 to 2020 n = 23,950.

Adults over 65 were more likely to have an undetectable viral load relative to younger adults (HR = 1.60 [1.47-1.756]) (Table 2, hazard curve in Figure 1). In addition, in/out of state residence does affect an undetectable viral load making the hazard lower (HR = 0.65 95% Confidence Interval [0.45-0.95].

Multiple Cox regression curve of an undetectable hepatitis C viral load.
Multivariable Cox Proportional Hazard Regressions with Selected Covariates of an Undetectable Viral Load among Antibody Positive Encounters in Orange County, California.
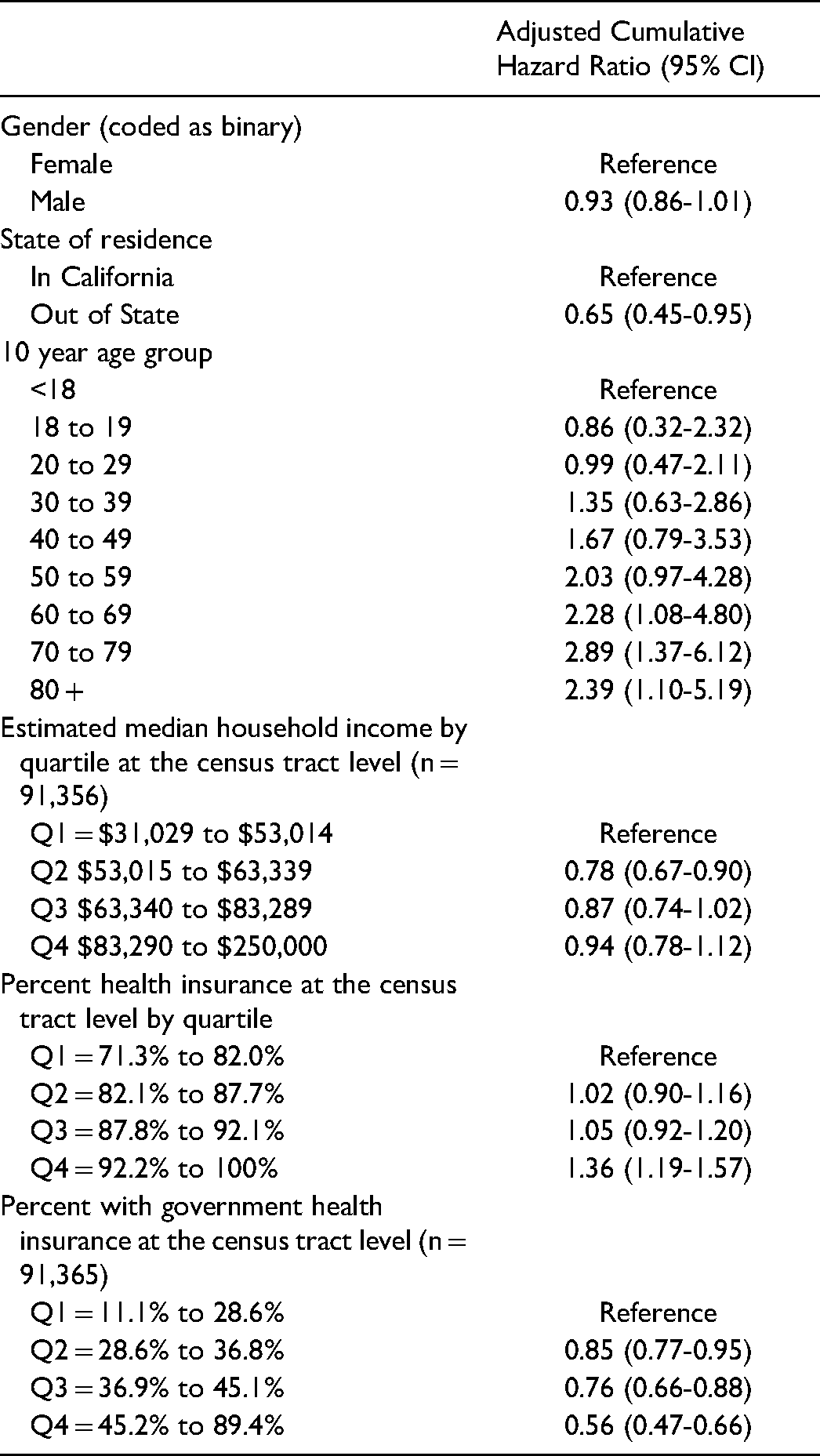
Residents of census tracts with the highest percentage of any health insurance coverage were more likely to have an undetectable viral load (HR = 1.36, 95% CI [1.09-1.70]). Patients in tracts with higher quartiles of government health insurance were less likely to have an undetectable viral load. The fourth quartile of % health insurance (over 92% coverage compared to quartile 1) HR = 1.36 (1.19-1.57) and all quartiles of % on government health insurance compared to quartile 1 were less likely to have an undetectable viral load. In general, persons residing in census tracts with a higher percentage of public health insurance showed reduced HRs of receiving treatment.
An interaction term between median income and health insurance was significant (Table 3)
Multivariable Cox Proportional Hazard Model with ACS Variables with and Without Interaction Term among Antibody Positive Encounters in Orange County, California.
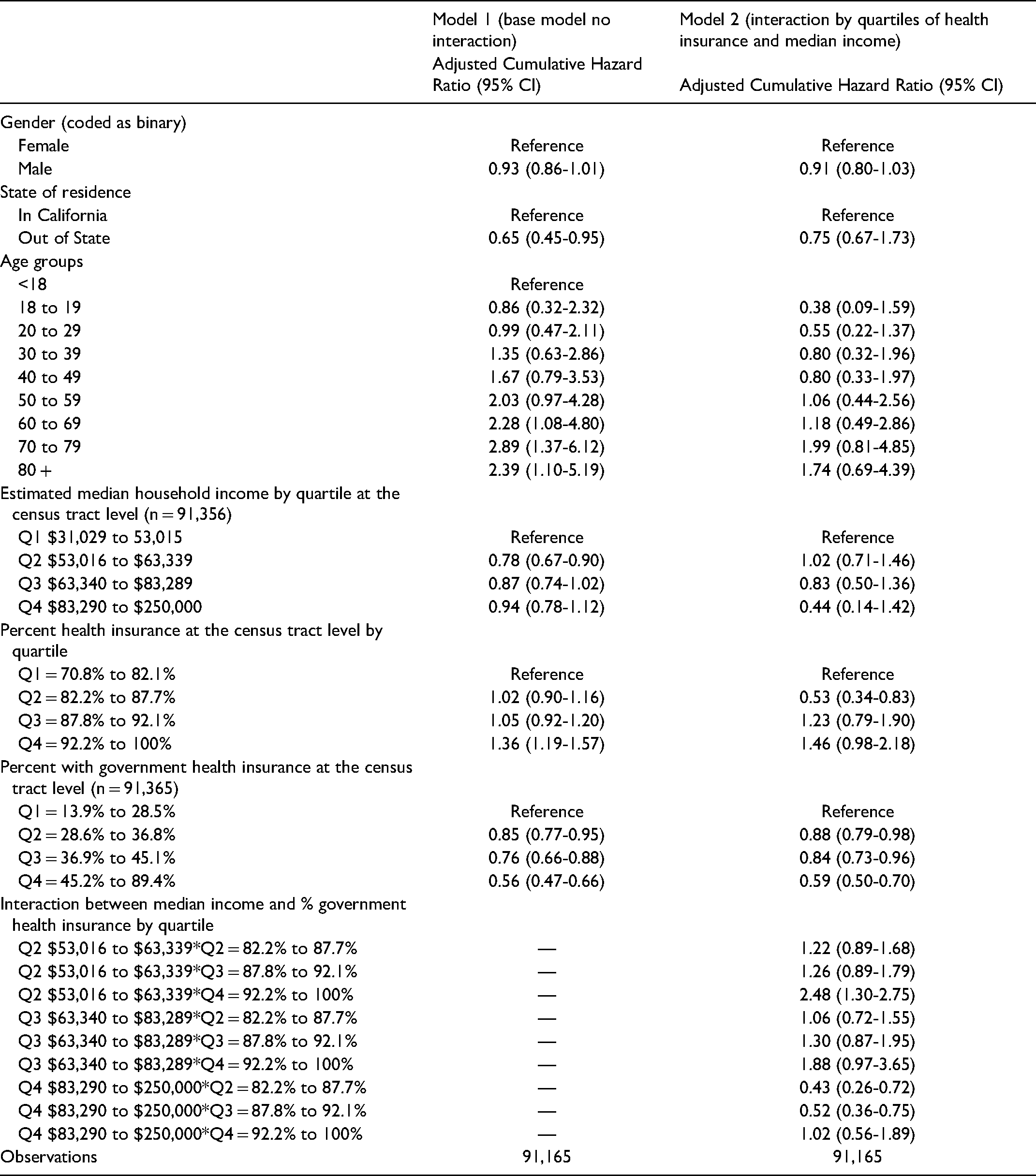
When holding quartile of income constant, increasing the quartile of insurance increased the HR of an undetectable viral load. Quartile 4 compared to quartile 1 had the highest HR of 9.75.
Multivariable Cox Proportional Hazard Models Stratified by Patients Over 65
Given the discovered difference in treatment rates by those over 65 compared to younger patients and the strong relationship between retirement age and health insurance type, we conducted a stratified post hoc analysis for those aged 65 and younger (n = 74,136) and those over 65 (n = 17,029 in Table 4, hazard curves in Figure 2). Among older adults, a greater proportion of public health insurance at the census tract corresponds with an increased probability of that patient having an undetectable viral load.

Multiple Cox regression stratified by age coded as binary (65 and under, and over 65) of an undetectable hepatitis C viral load.
Stratified Cumulative Hazard Ratios of an Undetectable Viral Load among HCV Antibody Positive Encounters in Orange County, California.

Discussion
This study examined over a seven-year period with 91,165 care encounters of 23,950 patients in the sixth largest county in the U.S., approximately 97% of patients who have HCV virus antibodies do not indicate undetectable viral load indicating a lack of HCV treatment or spontaneous clearance. Those who lived in census tracts with higher quartiles of private health insurance, and those over the age of 65, had higher odds of an undetectable viral load with 34% patients not being tested at all for viral load. Taken together, findings indicate an alarming level of potential under-diagnosis and linkage to care for detected HCV antibody-positive cases. These results indicate financial and health insurance barriers to diagnosis that impede patients’ ability to be linked to care.
These findings imply inadequate screening for those 65 and younger compared to their older counterparts. 44 This confirmed results from a study that found that universal screening identified that those younger than the 1945 to 1965 birth cohort comprised nearly 48% of all HCV cases in four large metropolitan emergency departments. 45
Those in census tracts with lower insurance coverage are less likely to have undetectable viral load. In a study of 38,025 persons in sites across the United States, Ditah and colleagues found that those who did not continue HCV follow-up care were less likely to have health care insurance. 46 Our work builds upon that of Ditah and colleagues and covers a period after DAA approval. If others replicate our work using individual-level data on health insurance type, this financial barrier to treatment requires significant policy attention and amelioration.
47 Our study with a large sample size, in a large geographical area allows health practitioners to identify gaps in the care cascade and where some patients may still have infections.
The current study has policy implications, including bridging the gaps for poor insurance coverage negatively impacting care. Persons living with HCV need appropriate health insurance for those uninsured to help initiate treatment. Connections to care with more expansive insurance plans could be implemented using peer navigators and specialty pharmacies to target those ages 65 and younger and lower income. 48 Scientists must conduct further research to identify patients who fall out of the care cascade and better target interventions to link patients to care.
Limitations
Some of the limitations related to using surveillance data for secondary analysis. The missing covariates in surveillance data do not capture or indicate information relevant to HCV infection such as risk factors (eg, race, employment), occupation, individual insurance providers, persons in incarceration settings or risk behaviors such as injection drug use or those without homes. We are also unable to determine comorbidities such as HIV, hepatitis B infection, or other disease using these data. We cannot examine in this dataset if these groups with increased vulnerability have an increased risk of contracting HCV.2,46 Those with less access to health care and lower incomes are less likely to have an undetectable viral load, widening the gap of those who are unable to pay for expensive DAA medications. The inability to categorize and analyze these populations may lead to an underestimation of socioeconomic characteristics on likelihood of undetectable viral load.
Another limitation is the incomplete nature of public health surveillance data with missing values on individual covariates. We do not have accurate race/ethnicity data for these HCV cases, as 80% are missing. Regarding lab tests, we only know if individuals are viremic if they have tested for viral load, and we cannot verify if undetectable viral load was due to spontaneous clearance or treatment. We could not use these cases in the analysis because they had a missing address or failed to geocode. In addition, census tract-level information does not necessarily reflect the status of individuals living in that tract. Also, viremic, out-of-state patients may have returned to their home state for treatment, which we cannot capture in this dataset.
Finally, O.C. is a popular tourism destination for substance abuse rehabilitation in the U.S. This dataset may not reflect the burden of HCV in other settings such as homeless encampments and incarceration facilities. 49 Our results only reflect an undetectable HCV viral load from one county in California. They may not be generalizable to other locations in the state or the United States as a whole. Despite this limitation, the size of O.C.'s population (> 3 million) indicates that these results have public health implications for this community and counties of similar size and demographics.
Conclusion
In an era of effective treatment, the overwhelming HCV antibody positive patients OC do not have a detectable HCV viral load and are potentially infectious. Only 1% of all persons with HCV positive antibody tests had an undetectable viral load from 2014 to the beginning of 2020, which indicates a lack of HCV diagnosis and treatment initiation. Disparities in insurance coverage illustrate the potential for severe inequity in treatment. The USPSTF updated their guidelines in 2020, recommending universal HCV screening for all people ages 18 to 79. 50 Universal HCV screening and viral load testing will help increase care and treatment initiation. Ensuring that health insurance will cover treatment costs and connecting persons living with HCV to appropriate treatment and treatment completion are top priorities. Subsequent work in this area would benefit from understanding the structural, socioeconomic, and cost barriers to achieving this successful care cascade.
Supplemental Material
sj-docx-1-hme-10.1177_23333928211066181 - Supplemental material for Measuring Hazards of Undetectable Viral Load among Hepatitis C Antibody Positive Residents of a Large Southern California County
Supplemental material, sj-docx-1-hme-10.1177_23333928211066181 for Measuring Hazards of Undetectable Viral Load among Hepatitis C Antibody Positive Residents of a Large Southern California County by Sara Goodman, Matthew Zahn, Tim Bruckner, Bernadette Boden-Albala and Cynthia M. Lakon in Health Services Research and Managerial Epidemiology
Supplemental Material
sj-jpeg-2-hme-10.1177_23333928211066181 - Supplemental material for Measuring Hazards of Undetectable Viral Load among Hepatitis C Antibody Positive Residents of a Large Southern California County
Supplemental material, sj-jpeg-2-hme-10.1177_23333928211066181 for Measuring Hazards of Undetectable Viral Load among Hepatitis C Antibody Positive Residents of a Large Southern California County by Sara Goodman, Matthew Zahn, Tim Bruckner, Bernadette Boden-Albala and Cynthia M. Lakon in Health Services Research and Managerial Epidemiology
Footnotes
Acknowledgments
The authors would like to thank the entire Orange County Health Care Agency Communicable Disease Control Team, including Stephen Klish, Patrick Pham, and Joshua Jacobs, for their assistance in helping access and extract these data.
Authors’ Contributions
SG was responsible for extracting and coding the data, performing the analysis, drafting, and writing the manuscript, MZ provided technical expertise, TB was responsible for reviewing and editing the manuscript and helping to create the analysis plan. BBA and CL also provided technical and writing advice for this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the California Department of Public Health CalREDIE data warehouse, but restrictions apply to the availability of these data, which were used under data sharing agreements for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the California Department of Public Health (CDPH). CDPH can be reached by phone or email: Point of contact: +1 866-866-1428 or CalREDIEHelp@cdph.ca.gov
Statement of Permission
As part of routine infectious disease surveillance under California State Health Code Title 17 a §2500, §2593, §2641.5 to 2643.20, and §2800 to 2812 Reportable Diseases and Conditions this data is collected regularly and may be used for enhanced surveillance. Ms. Goodman's role as a intern epidemiologist at the Orange County Health Care Agency, the director of the communicable disease control branch, Dr. Matthew Zahn (a co-author on this paper), through the California Department of Public Health granted permission for Ms. Goodman to use this anonymized data for analysis as part of her doctoral dissertation. See attached documentation from the Orange County Health Care Agency IRB application and approval letter.
Ethics approval and consent to participate
This research was approved by the Institutional Review Boards of the University of California, Irvine protocol H.S. # 2019-548 and the Orange County Health Care Agency (Research Project 2020-03). No consent was obtained as this is routinely collected public health data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of California, Irvine Program in Public Health Dissertation Writing Fellowship.
Supplemental material
Supplemental material for this article is available online
Author Biographies
Appendix A: Sample Diagram
See Figure 3.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.