
Abstract
Objectives:
Chronic hepatitis B virus (HBV) infection is a lifelong infection that can cause serious liver damage and liver cancer. The last surveillance-based prevalence estimate of chronic HBV infection in New York City was 1.2% in 2008; however, it did not account for persons with undiagnosed infection. The objective of this study was to calculate the prevalence of chronic HBV infection, including undiagnosed infection, for 2016 by using surveillance data and literature-based information.
Methods:
We calculated the number of persons with diagnosed chronic HBV infection (2000-2016) who were alive and living in New York City in 2016 by using routine surveillance data. We estimated the percentage of persons with undiagnosed chronic HBV infection by using birth region–specific percentages from the literature, weighted by the proportion of the New York City population with diagnosed chronic HBV infection from the same birth region. We identified minimum, maximum, and most likely values for the percentage with undiagnosed chronic HBV infection to generate 95% certainty limits (CLs) of the prevalence estimate.
Results:
The prevalence of chronic HBV infection in 2016, including undiagnosed infection, in New York City was 2.7% (95% CL, 2.2%-3.6%), representing approximately 230 000 persons. The prevalence of diagnosed chronic HBV infection was 1.5%. The estimated prevalence among non–US-born residents was 6.9% (95% CL, 5.4%-8.9%).
Conclusions:
The current burden of chronic HBV infection in New York City, especially for non–US-born residents, is substantial. A renewed focus and dedication of resources is required to increase the number of new diagnoses and improve provider capacity to care for the large number of persons with chronic HBV infection.
Chronic hepatitis B virus (HBV) infection is a lifelong, blood-borne infection that can cause liver fibrosis, cirrhosis, and liver cancer. 1 The risk of chronic infection varies substantially by age: 90% of perinatally exposed infants, 25%-50% of children, and 5% of adults develop chronic infection after exposure. 2 Chronic HBV infection can be treated to limit liver damage, but eligibility for treatment depends on infection stage, so not everyone is eligible, and therapy is not curative. 3
The prevalence of chronic HBV infection varies widely throughout the world; the highest prevalence of chronic HBV infection (≥5% of the population) is in sub-Saharan African and East/Southeast Asian countries. 4 The current estimated prevalence of chronic HBV infection in the United States is 0.3%. 4,5 Approximately 70% of persons with chronic HBV infection in the United States were non–US born and acquired the infection in the country from which they emigrated; as a result, recent National Health and Nutrition Examination Survey (NHANES) cycles have oversampled persons of non-Hispanic Asian race. 5,6 However, because the prevalence of chronic HBV infection in a given location likely depends on the proportion of the population born in a high-prevalence, HBV-endemic country, and the distribution of these persons is not even across the United States, the prevalence estimate in the United States is likely lower than in a city such as New York City, where about 40% of all residents in 2016 were non–US born. 6,7
The New York City Department of Health and Mental Hygiene (DOHMH) has found through routine surveillance and enhanced investigation that most persons with chronic HBV infection in New York City were born in countries with a high prevalence of chronic HBV infection. From enhanced investigations in 2009 and 2015, more than 50% of interviewed patients indicated that they were born in China or Taiwan; approximately 7% reported being US born (DOHMH unpublished data). 8 In addition, their providers rarely identified risk factors for hepatitis B transmission, such as injection drug use or sexual contact, suggesting that most persons likely acquired their infection perinatally or as children in their birth countries before immigrating to the United States. 8
The most recent estimate of the prevalence of chronic HBV infection in New York City was 1.2%, based on DOHMH surveillance data on the number of persons reported with a positive hepatitis B test through 2008. 9 However, this number did not take into account an estimate of the number of persons with undiagnosed chronic HBV infection. Many studies indicate that large percentages of persons at risk for chronic HBV infection are unscreened, do not receive a diagnosis, and are unaware of their infection. 5,10 -15
We estimated the prevalence of chronic HBV infection in New York City in 2016 on the basis of the number of persons reported through routine surveillance from 2000 through 2016, excluding persons known to be deceased and estimated to have moved out of New York City, and incorporating an estimate of the number of persons with undiagnosed infection. DOHMH, policy makers, and the clinical community can use this estimate to understand the current burden of chronic HBV infection in New York City and facilitate planning to reduce morbidity and mortality related to chronic HBV infection.
Methods
The prevalence of chronic HBV infection reflects not only the number of persons with diagnosed chronic HBV infection (as available from routine surveillance data) but also the number with undiagnosed infection. Determining how many persons have undiagnosed infection is challenging because there is no record of their infection to review. We used estimates from published studies to inform the percentage of persons with undiagnosed chronic HBV infection in New York City.
New York City DOHMH Chronic HBV Infection Surveillance System
Electronic laboratory reporting was implemented at DOHMH from 2002 through 2008 (required by law beginning in 2006) and was considered complete by 2009. 16 All positive tests for hepatitis B surface antigen (HBsAg), hepatitis B e antigen (HBeAg), core immunoglobulin M (IgM), hepatitis B DNA, and hepatitis B genotype ordered by health care providers from New York City residents are reportable to DOHMH. Reports from persons with unknown addresses but tested by New York City–based health care providers are also reported. Electronic laboratory reporting in New York City is considered comprehensive and complete. 17 Multiple positive tests for the same person are automatically joined by using a deduplication algorithm, such that each person has a unique, complete positive test history. The postal address information for each person reported to DOHMH is updated any time a new address is included in a disease report.
Using Surveillance Data to Estimate the Number of Persons With Diagnosed Chronic HBV Infection
To use surveillance data to estimate the number of persons with diagnosed chronic HBV infection living in New York City at the end of 2016, we adjusted the number of persons reported with a positive test to exclude those known to be deceased by 2016 and those estimated to have moved from New York City since they were last reported to DOHMH.
We included all persons with ≥1 positive test for HBsAg, HBeAg, DNA, or genotype performed from January 1, 2000, through December 31, 2016, and not reported as an acute hepatitis B case (core IgM positive and/or reported with symptoms of acute viral hepatitis) in the initial count of persons with diagnosed chronic HBV infection. We excluded anyone with no evidence of a residential address in New York City (eg, persons who were reported with a missing address but whose provider was in New York City) because we could not be certain they were New York City residents. We also removed all persons who matched to a New York City death certificate record for deaths between January 1, 2000, and December 31, 2016.
Because electronically reported laboratory tests cannot indicate when someone moves from New York City, but the receipt of a test can indicate if someone still resides in New York City, we needed to estimate and exclude persons with chronic HBV infection thought to have moved from New York City by 2016. We estimated the probability that a person was still residing in New York City in 2016 on the basis of 2 factors: (1) year of their last reported hepatitis B test that indicated a residential address in New York City and (2) data from US Internal Revenue Service (IRS) tax returns. Tax return data can be used to calculate an annual probability of outmigration from a given location by comparing the residential address of each household filing a tax return in a given year with the residential address on its previous year’s tax return. 18 Using IRS outmigration estimates for New York City from 2000-2016, we calculated the probability that a person was still residing in New York City in 2016 by multiplying each annual probability of outmigration from the year of the person’s last reported hepatitis B test through 2016. Applying each yearly probability of residing in New York City in 2016 to the number of persons whose last hepatitis B test was in that corresponding year, we calculated the final number of persons estimated to still be residing in New York City in 2016. DOHMH previously used this approach to estimate the prevalence of chronic HBV infection and chronic hepatitis C virus infection. 8,19,20
Estimating the Proportion of Persons With Undiagnosed Chronic HBV Infection
We reviewed the literature to identify studies that calculated the percentage of persons with undiagnosed chronic HBV infection. We searched PubMed for articles describing hepatitis B prevalence or screening, restricted to US estimates (or global studies that included estimates for the United States). We reviewed articles for information on the number of persons in each study who were previously undiagnosed, reported never being previously screened, or reported being unaware of their infection. The study methods varied, but most relied on a technique of testing or reviewing the medical records of a particular population for chronic HBV infection and then surveying those whose tests were positive for chronic HBV infection about whether they had been aware of their diagnosis. 5,10,12 -14 Although being aware of infection is not the same as having a diagnosed infection (ie, an infection can be diagnosed and reported to DOHMH without someone being aware), these estimates are often the only practical way to ascertain underdiagnosis. Most of these studies were performed in specific, primarily non–US-born communities, such as Asian-born residents of various US cities and West African–born pregnant women in New York City. 10,12 -14 Alternatively, using data from the 2013-2014 New York City Health and Nutrition Examination Survey (NYC HANES), a citywide equivalent to NHANES, DOHMH matched 7 survey participants whose tests were positive for HBsAg to the surveillance system and found that 2 had not previously been reported to DOHMH, suggesting a lack of previous diagnosis. 21 Modeling studies have also been used to estimate underdiagnosis globally, including in the United States. 15
We calculated the likely proportion of persons with undiagnosed chronic HBV infection by using percentages from the literature, stratified by region of birth and weighted by the percentage of persons in New York City from the corresponding birth region with diagnosed chronic HBV infection. For underdiagnosis in the Asian-born population in New York City, we used the estimate from a study that tested and interviewed Asian Americans (98.8% of whom were non–US born) at a New York City hepatitis B clinic and found that 34.9% of persons were previously undiagnosed. 12 For underdiagnosis in the African-born population in New York City, we used the estimate from a study that found from medical record review that 46.2% of West African–born women who had recently given birth in the Bronx were undiagnosed. 14 Because we could find no other birth region–specific estimates, we grouped all others with chronic HBV infection as non-Asian, non-African born, with an underdiagnosis estimate from an NHANES follow-up study reporting that 70.1% of non-Asian, non-black NHANES participants testing positive for HBV infection were previously unaware of their diagnosis (Table 1). 5
Inputs used to estimate the percentage of the population with undiagnosed chronic hepatitis B virus infection, by region of birth, New York City, 2016
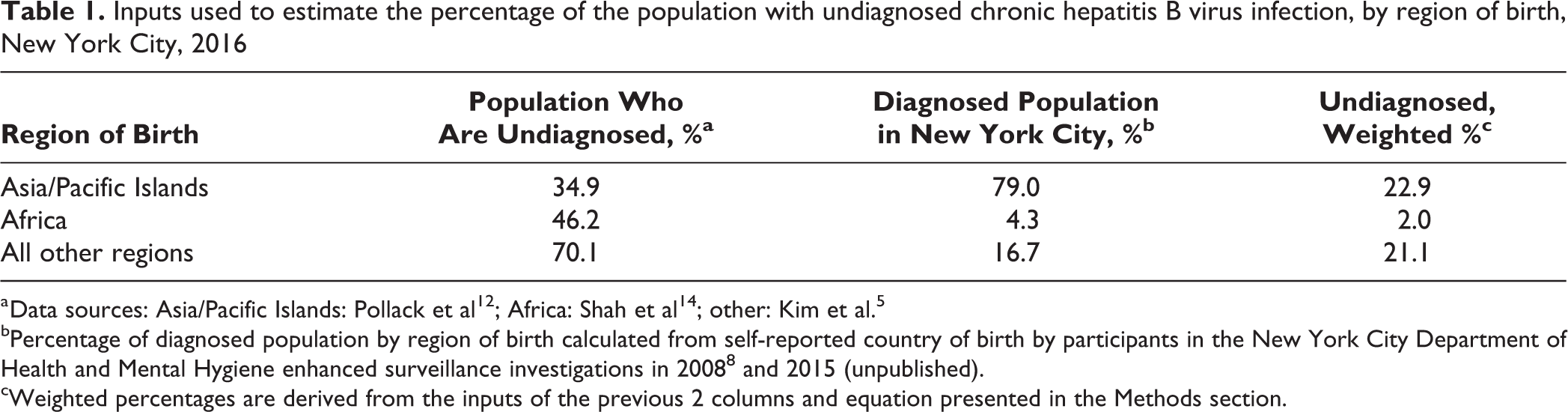
a Data sources: Asia/Pacific Islands: Pollack et al 12 ; Africa: Shah et al 14 ; other: Kim et al. 5
bPercentage of diagnosed population by region of birth calculated from self-reported country of birth by participants in the New York City Department of Health and Mental Hygiene enhanced surveillance investigations in 2008 8 and 2015 (unpublished).
cWeighted percentages are derived from the inputs of the previous 2 columns and equation presented in the Methods section.
We calculated the proportion of the New York City population with diagnosed chronic HBV infection from each birth region by using the results of DOHMH enhanced surveillance investigations. Because of resource constraints and the large volume of chronic HBV infection reports received annually, DOHMH does not investigate most cases of chronic HBV infection. However, periodically, DOHMH staff members interview a random sample of persons with chronic HBV infection. During 2 periods of enhanced HBV surveillance conducted in 2008 and 2015, investigators interviewed randomly selected participants and obtained detailed clinical and epidemiologic data, including data on country of birth (DOHMH unpublished data). 8 Of 348 respondents from these surveys who reported country of birth information, 275 (79.0%) persons indicated birth in an Asian/Pacific Island country, 15 (4.3%) indicated birth in an African country, and 58 (16.7%) reported birth elsewhere (including 23 [6.6%] reporting birth in the United States; Table 1).
Using the percentage of persons with undiagnosed chronic HBV infection by birth region and the proportions of those with diagnosed infection from each birth region, we calculated an overall estimate of the percentage undiagnosed in New York City (Pundiagnosed) by using the following formula:
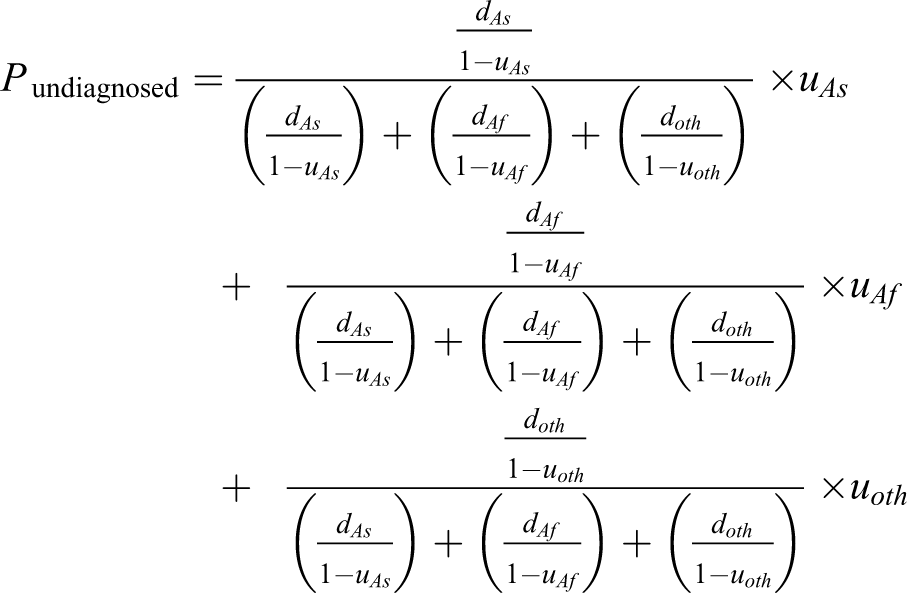
where, for each birth region, Asian born (As), African born (Af), and other (oth), d is the proportion of all persons with diagnosed chronic HBV infection who are from that birth region and u is the proportion of persons from that birth region with chronic HBV infection thought to be undiagnosed. This accounts for the fact that the distribution of chronic HBV infection by birth region was known only among persons with diagnosed infection, not all persons with chronic HBV infection. The final result is the sum of the proportion of New York City residents with chronic HBV infection that is undiagnosed for each of the 3 birth regions. Using the aforementioned equation and the inputs from Table 2, we calculated that 46.0% of New York City residents with chronic HBV infection were likely undiagnosed. We determined that the likely minimum percentage was 28.6%, based on NYC HANES findings, and that the maximum percentage was 65.0%, based on modeling studies. 15
Estimated number of persons with chronic hepatitis B virus infection based on the year of their last hepatitis B test reported to the New York City Department of Health and Mental Hygiene and the probability of still residing in New York City, New York City, 2016a
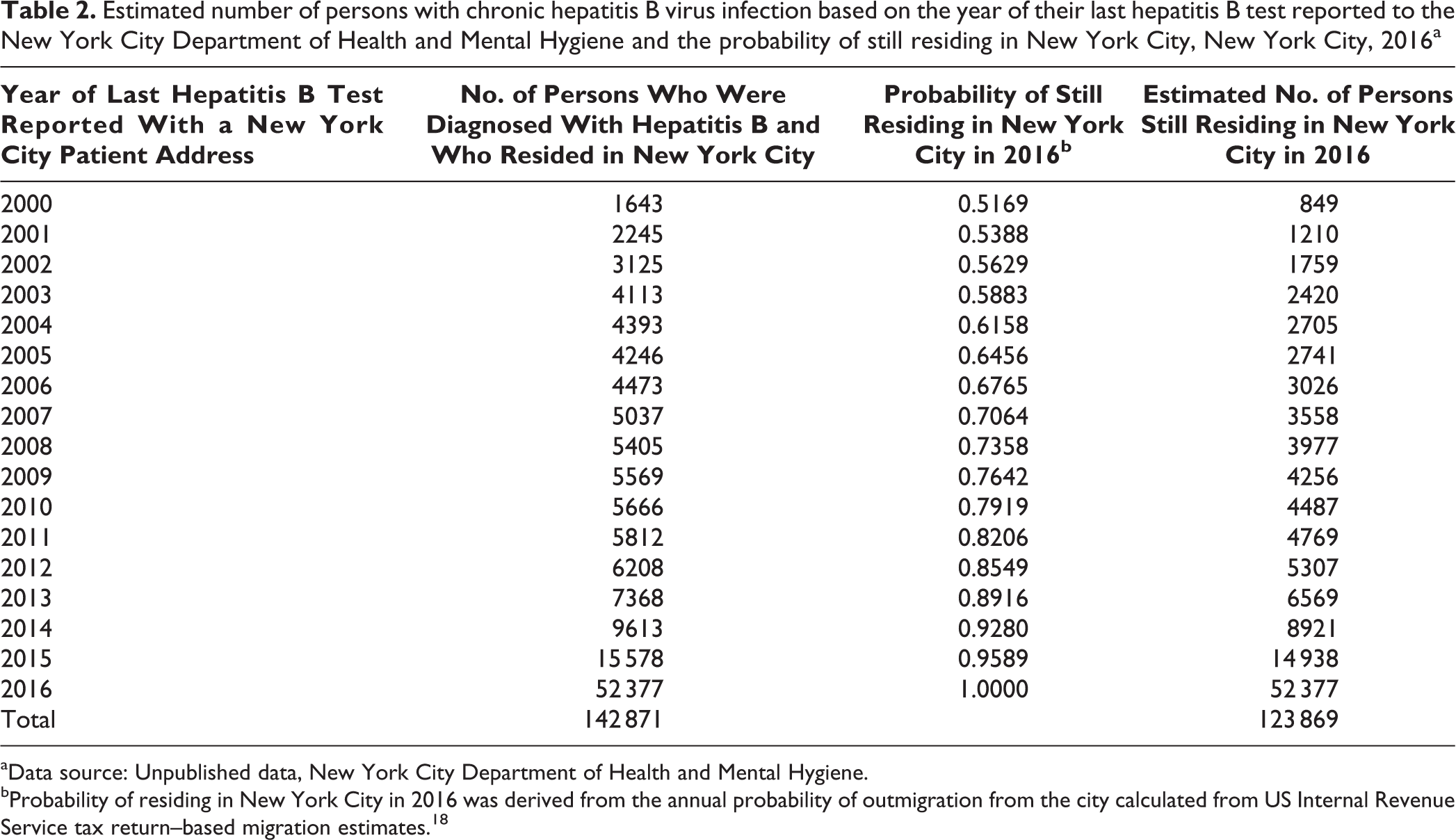
aData source: Unpublished data, New York City Department of Health and Mental Hygiene.
bProbability of residing in New York City in 2016 was derived from the annual probability of outmigration from the city calculated from US Internal Revenue Service tax return–based migration estimates. 18
Incorporating an Estimate of Underdiagnosis to Calculate Prevalence
We calculated the total number of persons in New York City with chronic HBV infection, both diagnosed and undiagnosed, by using the following formula: number of persons alive and residing in New York City in 2016 with a positive hepatitis B test/(1 − percentage of persons with chronic HBV infection who are undiagnosed). We used a betaPERT distribution (ie, a smoothed version of the triangular distribution) using the minimum, maximum, and most likely values identified previously to incorporate uncertainty in the percentage of persons with undiagnosed chronic HBV infection. 22 Using 50 000 trials to randomly draw from the betaPERT distribution by using Latin Hypercube sampling (a method of random sampling of parameter values to generate a final estimate, similar to a Monte Carlo simulation) and the aforementioned formula, we generated an estimate of the total number of persons with chronic HBV infection in New York City, with 95% certainty levels (CLs). 22 We used Oracle Crystal Ball, an Excel add-in, for the analysis. 22 We calculated the final prevalence estimate and 95% CLs by dividing the estimated number of persons with chronic HBV infection by the 2016 intercensal population estimate in New York City (n = 8 537 673; unpublished New York City population estimates, modified from US Census Bureau interpolated intercensal population estimates, 2016; New York City Department of Health and Mental Hygiene).
We also calculated the prevalence of chronic HBV infection in the non–US-born population in New York City by multiplying the total number of persons with chronic HBV infection by 93.4%, using the proportion of persons identified as non–US born from DOHMH-enhanced investigations. We divided this number by the American Community Survey 2016 estimate for the non–US-born population in New York City (n = 3 200 219). 6 This analysis was classified as public health surveillance by the DOHMH Institutional Review Board. As such, it was exempt from review.
Results
From surveillance reports, we identified 166 803 persons with ≥1 positive HBsAg, HBeAg, DNA, or genotype test performed from 2000 through 2016 (Figure). Of these, 9850 (5.9%) persons had died during the study period and were excluded. Of 156 953 living persons with a positive hepatitis B test, 14 082 (9.0%) had no known New York City address from 2000 through 2016, leaving 142 871 persons known to have resided in New York City during the study period. Of these, we estimated that 19 002 (13.3%) had moved from New York City by 2016, leaving 123 869 persons with diagnosed chronic HBV infection alive and residing in New York City in 2016 (Table 2).
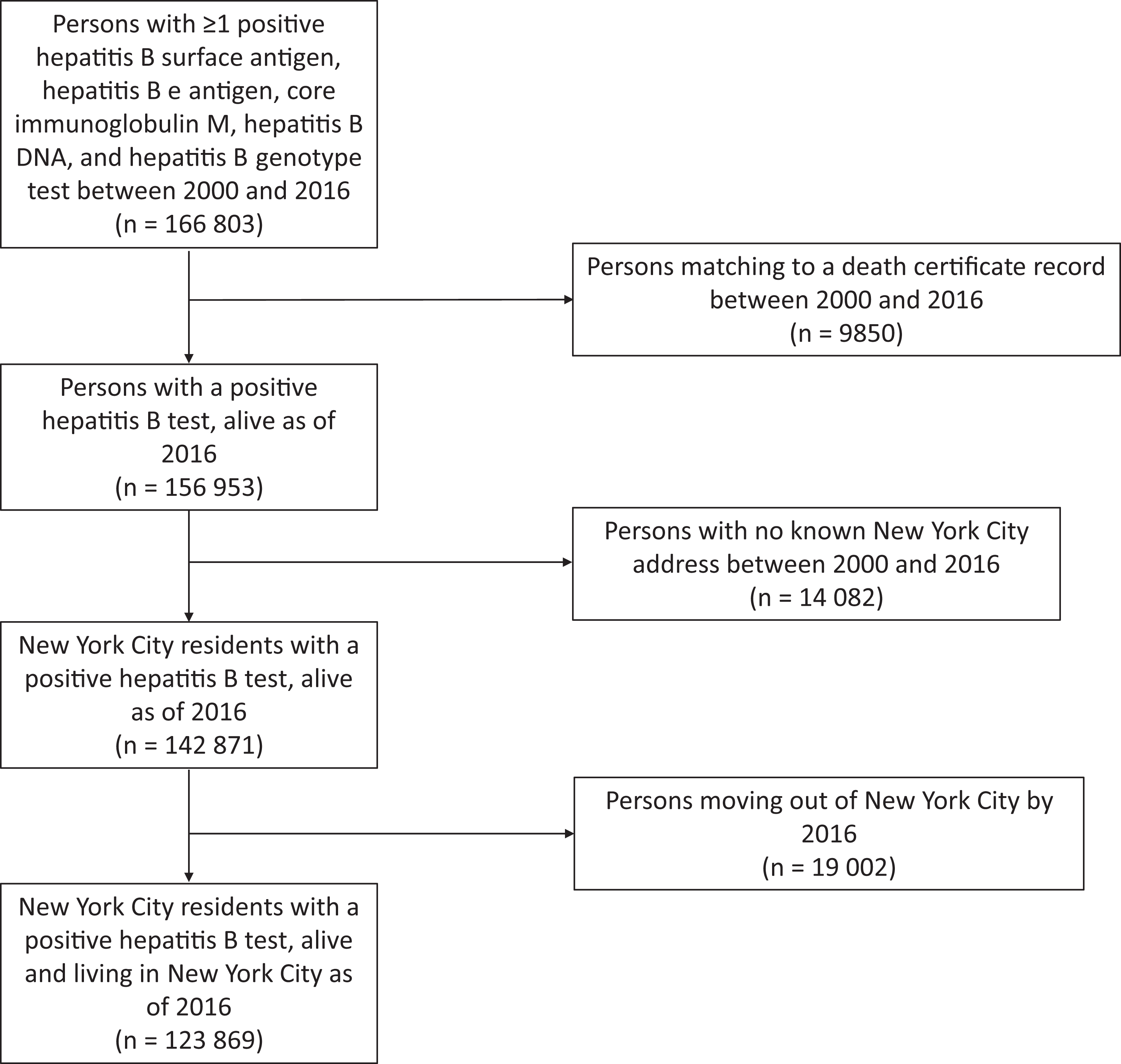
Persons included in the surveillance-derived estimate of diagnosed chronic hepatitis B virus infection, New York City, 2016. Data source: Unpublished data, New York City Department of Health and Mental Hygiene.
From the Crystal Ball simulations, incorporating the distribution of the proportion of persons with undiagnosed infection, we estimated that 230 254 persons (95% CL, 186 474-304 191) with chronic HBV infection resided in New York City in 2016. The estimated prevalence of chronic HBV infection, including undiagnosed infection, was 2.7% (95% CL, 2.2%-3.6%). The prevalence of diagnosed chronic HBV infection was 1.5%.
The estimated total number of non–US-born persons with chronic HBV infection in New York City was 215 057 (95% CL, 174 167-284 114), and the estimated prevalence among all non–US-born residents in New York City in 2016 was 6.9% (95% CL, 5.4%-8.9%).
Discussion
We estimated that the prevalence of chronic HBV infection in New York City in 2016 was 2.7%, representing approximately 230 000 persons, about half of whom had not yet received a diagnosis. Those who did not receive a diagnosis were, by definition, not in care for chronic HBV infection and not receiving recommended services, including assessment for fibrosis or cirrhosis, screening for liver cancer, treatment if indicated, and receipt of health promotion guidance needed to keep them healthy while living with chronic HBV infection.
The estimated prevalence of chronic HBV infection in New York City, even limited to the 1.5% prevalence of diagnosed chronic HBV infection, was higher than the estimate of 0.3% in the United States. 15,23,24 It was also higher than a citywide prevalence estimate of 0.7% with chronic HBV infection from NYC HANES 2013-2014; however, the NYC HANES estimate was considered unreliable because of the small number of participants testing positive for HBsAg. 21 The last surveillance-based prevalence estimate in New York City was 1.2% (about 110 000 persons) in 2008. The authors noted, “If [one-half to two-thirds] of chronically infected persons in New York City remain undiagnosed, the surveillance-based approach indicates the true prevalence of chronic HBV [infection] in New York City might be ≥2.4%.” 9 Both the current estimate of the total prevalence (2.7%) and the estimate of the diagnosed-only prevalence (1.5%) align closely with the 2008 estimate but indicate an increasing proportion of the population with chronic HBV infection. This increase from 2008 to 2016 translates to almost 14 000 additional persons in New York City living with chronic HBV infection tested and reported to DOHMH.
The highest prevalence of chronic HBV infection found in this study was among New York City residents born outside the United States (6.8%), which highlights an uneven distribution of the burden of chronic HBV infection in New York City and emphasizes that the populations most likely to lack access to health care (ie, non–English-speaking, uninsured, and/or undocumented persons) are also at increased risk of chronic HBV infection. 25 -28 The prevalence of chronic HBV infection might be higher still among New York City residents born in particular countries outside of the United States. At the same time, the proportion of persons receiving appropriate monitoring and care for chronic HBV infection in the United States is low; in a 2010 review of hepatitis B care and treatment practices, only 10% of those eligible for treatment were estimated to be receiving treatment. 29 -31 With more than 106 000 persons thought to have undiagnosed chronic HBV infection in New York City, in addition to approximately 124 000 persons with already diagnosed chronic HBV infection, substantial work is needed to screen, diagnose, and link persons with chronic HBV infection in New York City to comprehensive care.
Limitations
This study had several limitations. First, it was not possible to account for the uncertainty in all of the assumptions needed to estimate prevalence. We based the estimate of outmigration only on tax return data, and its accuracy among persons with chronic HBV infection in New York City is not known, specifically whether the probability of filing tax returns differs by non–US-born or US-born status or by other factors that might be associated with chronic HBV infection. However, the association between the probability of filing annual tax returns and migration status (ie, whether those who do not file tax returns are also more likely to move out of the city) is also not known.
Second, although we attempted to identify the most likely estimate for the proportion with undiagnosed infection and to provide a range of possible values, the undiagnosed estimate may not be accurate. The subgroup-specific estimates from the literature likely do not correspond perfectly to the birth regions defined from enhanced surveillance investigations, and countries within a birth region likely vary widely in rates of undiagnosed infection. In addition, 23% of persons selected for interview during enhanced surveillance investigations did not report a country of birth. The literature-based estimates for the percentage of undiagnosed infections are also not current relative to 2016 (estimates from 2005, 12 2004-2008, 14 and 2011-2014 5 ). In 2014, the US Preventive Services Task Force updated the recommendation to screen for hepatitis B in groups with risk factors for infection, including those born in countries with a high prevalence of chronic HBV infection. 32 Changes in US Preventive Services Task Force recommendations can result in changes in insurance reimbursement, and these changes might have increased screening rates and the proportion of persons diagnosed or aware of infection after some of the literature estimates were generated. However, other measures of underdiagnosis or measures to estimate the possible screening changes were not available. Finally, the underdiagnosis estimates might reflect a lack of awareness of infection status rather than undiagnosed infection, thereby inflating the number of undiagnosed infections in New York City.
Third, DOHMH does not routinely receive reports of laboratory tests performed by Veterans Health Administration facilities; therefore, patients with chronic HBV infection who primarily receive care at such facilities would not likely be included in the prevalence estimate. However, the prevalence of chronic HBV infection among US veterans is estimated to be low (<1%). 33
Finally, we might have underestimated the number of persons with diagnosed chronic HBV infection because of the possibility of overmatching laboratory reports and death certificate information in the surveillance system. Matching reports of hepatitis B is more challenging than matching reports for other conditions, primarily because of the high percentage of persons of Asian descent, who often have commonly shared, shorter names that are harder to definitively match than longer, less common names, which could lead to overmatching of reports of chronic HBV infection and overestimating the number of deaths in this population. However, DOHMH has made internal efforts to adjust matching algorithms to account for Asian names to reduce the chance of overmatching.
Conclusions
Most chronic HBV infections in New York City were among residents born in high-prevalence, HBV-endemic countries. Because no cure for chronic HBV infection exists, the prevalence of chronic HBV infection in New York City primarily depends on in-migration from high-prevalence countries, outmigration from New York City, and deaths among those with chronic HBV infection. 4,34 Efforts to prevent perinatal, injection drug use–associated, sexual, and nosocomial transmission of hepatitis B remain essential. However, DOHMH, policy makers, and the clinical community must also increase resources toward improving screening and the diagnosis of HBV infection, building health care provider capacity to care for persons with chronic HBV infection, and facilitating patient awareness of chronic HBV infection and access to health care services, while targeting these efforts toward immigrant populations for whom the barriers to care may be more substantial than for nonimmigrant populations. This updated prevalence estimate will inform planning and advocacy efforts needed to achieve these goals and reduce morbidity and mortality associated with chronic HBV infection in New York City.
Footnotes
Acknowledgments
The authors thank the New York City Department of Health, Bureau of Communicable Disease, Viral Hepatitis Program and Reportable Disease Data, Informatics, and Analysis Unit for their support in maintaining the surveillance data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the following financial support for the research, authorship, and/or publication of this article: This work was funded through city tax levies.