
Abstract
Objective
Infants born to women with hepatitis B virus (HBV) infection are at high risk for chronic HBV infection and premature death. We examined epidemiologic trends among women with HBV infection who gave birth in New York City (NYC) to inform public health prevention activities.
Methods
We obtained data on HBV-infected women residing and giving birth in NYC during 1998-2015 from the NYC Perinatal HBV Prevention Program. We obtained citywide birth data from the NYC Office of Vital Statistics. We calculated the incidence of births to HBV-infected women per 100 000 live births and stratified by maternal race, birthplace, and age. We calculated annual percentage change (APC) in incidence of births to HBV-infected women by using joinpoint regression.
Results
Of 29 896 HBV-infected women included in the study, 28 195 (94.3%) were non–US-born, of whom 16 600 (58.9%) were born in China. Overall incidence of births to HBV-infected women per 100 000 live births increased from 1156 in 1998 to 1573 in 2006 (APC = 3.1%; P < .001) but declined to 1329 in 2015 (APC = –1.4%; P = .02). Incidence among US-born women declined from 1998 to 2015 (330 to 84; APC = –7.3%; P < .001) and among non–US-born women increased from 1998 to 2007 (1877 to 2864; APC = 3.6%; P < .001) but not thereafter. Incidence among women born in China increased from 1998 to 2006 (13 275 to 16 480; APC = 1.8%; P = .02) but decreased to 12 631 through 2015 (APC = –3.3%; P < .001).
Conclusions
The incidence of births to HBV-infected women in NYC declined significantly among US-born women but not among non–US-born women, highlighting the need for successful vaccination programs worldwide.
Hepatitis B virus (HBV) is transmitted through percutaneous or mucosal contact with infectious blood or bodily fluids. HBV infects the liver and can lead to liver cirrhosis, hepatocellular carcinoma, and premature death. Approximately 257 million people are infected with HBV worldwide, and an estimated 887 000 deaths occurred in 2015 as a result of complications of HBV infection. 1,2 The prevalence of HBV infection varies by World Health Organization (WHO) region; the prevalence of HBV infection in the WHO Region of the Americas is estimated at 0.7% of the general population, whereas in the WHO Western Pacific Region and the WHO Africa Region the prevalence of HBV infection is estimated at 6.2% and 6.1%, respectively. 1,2 In the United States, an estimated 850 000 to 2.2 million people are living with chronic HBV infection, and 20 900 acute HBV infections occurred in 2016. 3 -6
The incidence of HBV infection has been declining in the United States since the introduction of HBV vaccination. 7 In 1982, the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) first recommended HBV vaccination for selected people at high risk of HBV infection, including infants born to HBV-infected women. 8 In 1991, ACIP expanded the recommendation to include routine vaccination of all infants, and in 1997, it broadened the recommendation for routine and catch-up vaccination to include all children and adolescents aged <19 years. 9,10 By 1998, estimated coverage of 3-dose HBV vaccination among children aged 19-35 months in the United States was 87.0% (±0.7%). 11 The number of acute HBV infections in the United States has declined dramatically because of these vaccination efforts, most notably among children and adolescents aged <19 years for whom the reported incidence of HBV infection per 100 000 population decreased from 2.6 in 1991 to 0 in 2011. 3,12
HBV-infected pregnant women have a high risk of transmitting HBV to their newborns during birth. Without postexposure prophylaxis (PEP), up to 90% of births to HBV-infected women will result in perinatal HBV infection. 13 -15 Subsequently, 90% of infants infected at birth will develop chronic HBV infection, and up to 25% of people with chronic infection will die from HBV-related complications. 16,17 ACIP recommends PEP for infants born to HBV-positive women with HBV immune globulin and the first dose of HBV vaccine within 12 hours of birth followed by completion of the 3-dose HBV series, which is up to 95% effective in preventing perinatal HBV infection. 18,19 Post-vaccination serologic testing is performed to confirm immunity to HBV infection and to rule out infection.
To prevent perinatal HBV infection, ACIP recommends universal screening of pregnant women for hepatitis B surface antigen (HBsAg) during each pregnancy, case management of HBsAg-positive mothers and their infants, provision of PEP for infants born to HBV-infected mothers, and routine vaccination of all infants with the HBV vaccine series beginning at birth. 19 Since 1986, the New York City Department of Health and Mental Hygiene (DOHMH) has conducted surveillance and case management of HBV-infected pregnant women and their infants. 20 In 1990, the Centers for Disease Control and Prevention established the US Perinatal Hepatitis B Prevention Program (PHBPP) within the National Immunization Program. Since then, the DOHMH’s Bureau of Immunization has supported the New York City PHBPP to conduct perinatal HBV prevention activities. Upon receipt of HBsAg-positive reports among pregnant women, New York City PHBPP staff members contact each patient by telephone or in person to provide HBV-related health education, including how to prevent perinatal disease transmission. Staff members case manage infants born to HBV-infected women to ensure timely receipt of PEP and confirm immunity to HBV after completion of the HBV vaccine series. For many years, the New York City DOHMH had the second-highest annual number of infants born to HBV-infected pregnant women who are managed among US PHBPP grantees (unpublished data, Division of Viral Hepatitis, Centers for Disease Control and Prevention, 2005-2017).
The objective of our analysis was to describe epidemiologic trends among HBV-infected pregnant women who gave birth in New York City during 1998-2015 to inform public health prevention activities. Changes in the demographic characteristics of HBV-infected pregnant women may pose the need for new or updated programmatic activities.
Methods
Identification of HBV-Infected Pregnant Women
By law, health care providers attending to pregnant women who reside in New York City are required to test for HBsAg and report positive results to the DOHMH. 21,22 Clinical laboratories are also required to report HBV-positive results. 23,24 In addition, the HBsAg status of all women giving birth in New York State is recorded on the newborn metabolic blood collection form, and positive results are reported to the health department. 21
Data Sources and Analysis
We obtained routinely collected demographic data, including mother’s race, country of birth, and age at delivery, for HBV-infected pregnant women and their children from the New York City PHBPP Surveillance Database. 25 We enhanced the completeness of demographic data through matches with New York City’s immunization information system, the Citywide Immunization Registry, 26 and the New York City Office of Vital Statistics birth records. 27 We obtained de-identified citywide maternal demographic data for all births to women residing and giving birth in New York City from the New York City Office of Vital Statistics.
We included data on HBV-infected pregnant women in the analysis if they gave birth to a live infant from January 1, 1998, through December 31, 2015; resided in New York City at the time of delivery; and gave birth at a health care facility in New York City or at home. We excluded women with unknown residence or unknown location of delivery from the analysis. Of the 30 596 HBV-infected pregnant women who had a live birth during 1998-2015, 29 896 (97.7%) met the inclusion criteria. Reasons for exclusion were not mutually exclusive; of the 700 women excluded from the analysis, 119 were excluded because of residence outside of New York City at delivery (n = 117) or unknown residence at delivery (n = 2), and 594 were excluded because of delivery outside of New York City (n = 517) or unknown location of delivery (n = 77).
We aggregated data by year of delivery to determine the distribution of HBV-infected pregnant women by race, country of birth, and age at delivery. We categorized race as white, black, Asian (including Asian and Hawaiian/Pacific Islander), or other/unknown (including other, unknown race, and ≥2 races). We categorized country of birth as US-born or non–US-born; we further stratified non–US-born by women born in China (the most frequent country of birth among non–US-born women in our study) vs other non–US countries. We categorized age at delivery as <15, 15-24, 25-34, 35-44, and ≥45 years. We calculated incidence of births to HBV-infected women per 100 000 live births by year and stratified by mother’s race, country of birth, and age at delivery.
We conducted trend analyses using joinpoint regression, a method that describes changing trends in data during successive segments of time and assesses for breakpoints within data series. We calculated the magnitude and significance (α = .05) of data trends as annual percentage change (APC) per year within modeled time segments. We analyzed data by using SAS version 9.4 (SAS Institute, Inc) and Joinpoint version 4.5.0.1 software (Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute). DOHMH deemed this analysis as non-research.
Results
Of the 29 896 births to HBV-infected women, 20 079 (67.2%) women were Asian, 6149 (20.6%) were black, 3055 (10.2%) were white, and 613 (2.1%) were other/unknown race (Table 1). Most (n = 28 195, 94.3%) women were non–US-born, of whom 16 600 (58.9%) were born in China. Most women were aged 25-34 (n = 18 352, 61.3%) or 15-24 (n = 6841, 22.9%) at the time of delivery. The median annual number of births to HBV-infected women was 1670 (range, 1324-1927), and the distribution of births to HBV-infected women by maternal demographic characteristics varied by year (Table 2).
Distribution and incidence of births to HBV-infected women, stratified by maternal race, age at delivery, and country of birth, New York City, 1998-2015 a
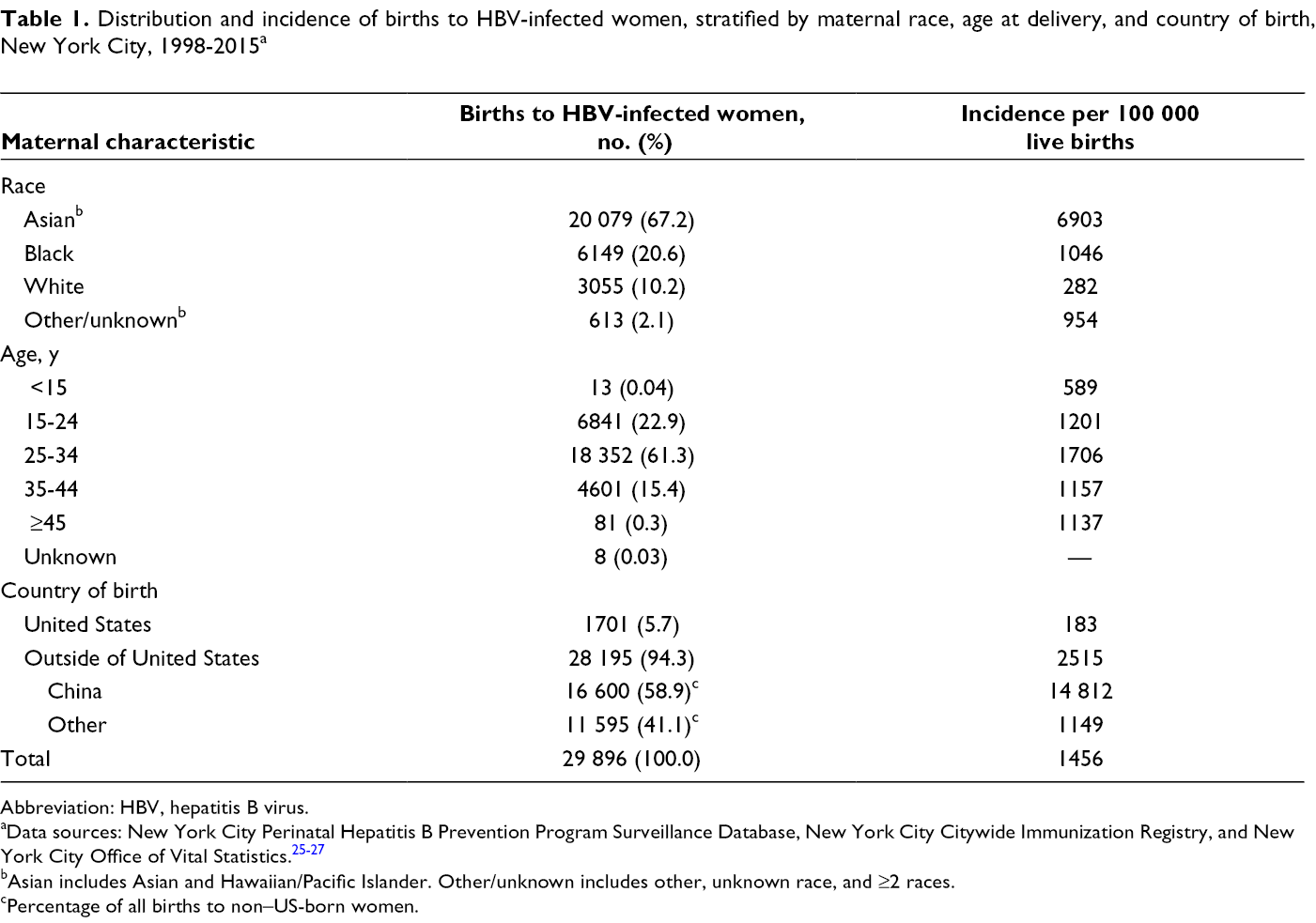
Abbreviation: HBV, hepatitis B virus.
aData sources: New York City Perinatal Hepatitis B Prevention Program Surveillance Database, New York City Citywide Immunization Registry, and New York City Office of Vital Statistics. 25 -27
bAsian includes Asian and Hawaiian/Pacific Islander. Other/unknown includes other, unknown race, and ≥2 races.
cPercentage of all births to non–US-born women.
Number of births to HBV-infected women, by year of birth, stratified by maternal race, age at delivery, and country of birth, New York City, 1998-2015 a
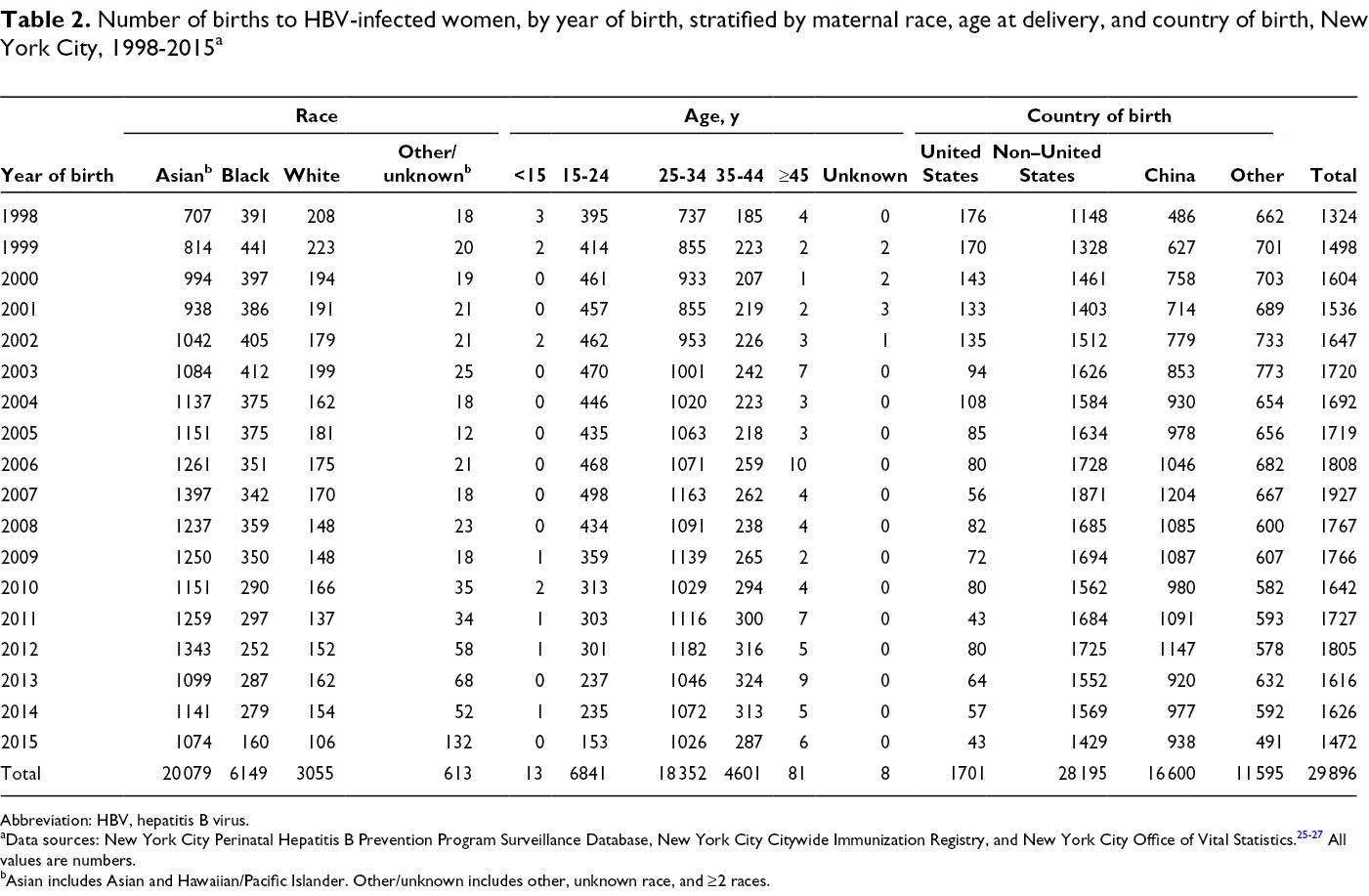
Abbreviation: HBV, hepatitis B virus.
aData sources: New York City Perinatal Hepatitis B Prevention Program Surveillance Database, New York City Citywide Immunization Registry, and New York City Office of Vital Statistics. 25 -27 All values are numbers.
bAsian includes Asian and Hawaiian/Pacific Islander. Other/unknown includes other, unknown race, and ≥2 races.
Trends in Overall Incidence
The median incidence of births to HBV-infected women per 100 000 live births was 1474 (range, 1156 in 1998 to 1633 in 2007) (Figure 1). The incidence of births to HBV-infected women per 100 000 live births increased significantly from 1156 in 1998 to 1573 in 2006 (APC = 3.1%; P < .001). However, the incidence of births to HBV-infected women declined to 1329 in 2015 (APC = –1.4%; P = .02).
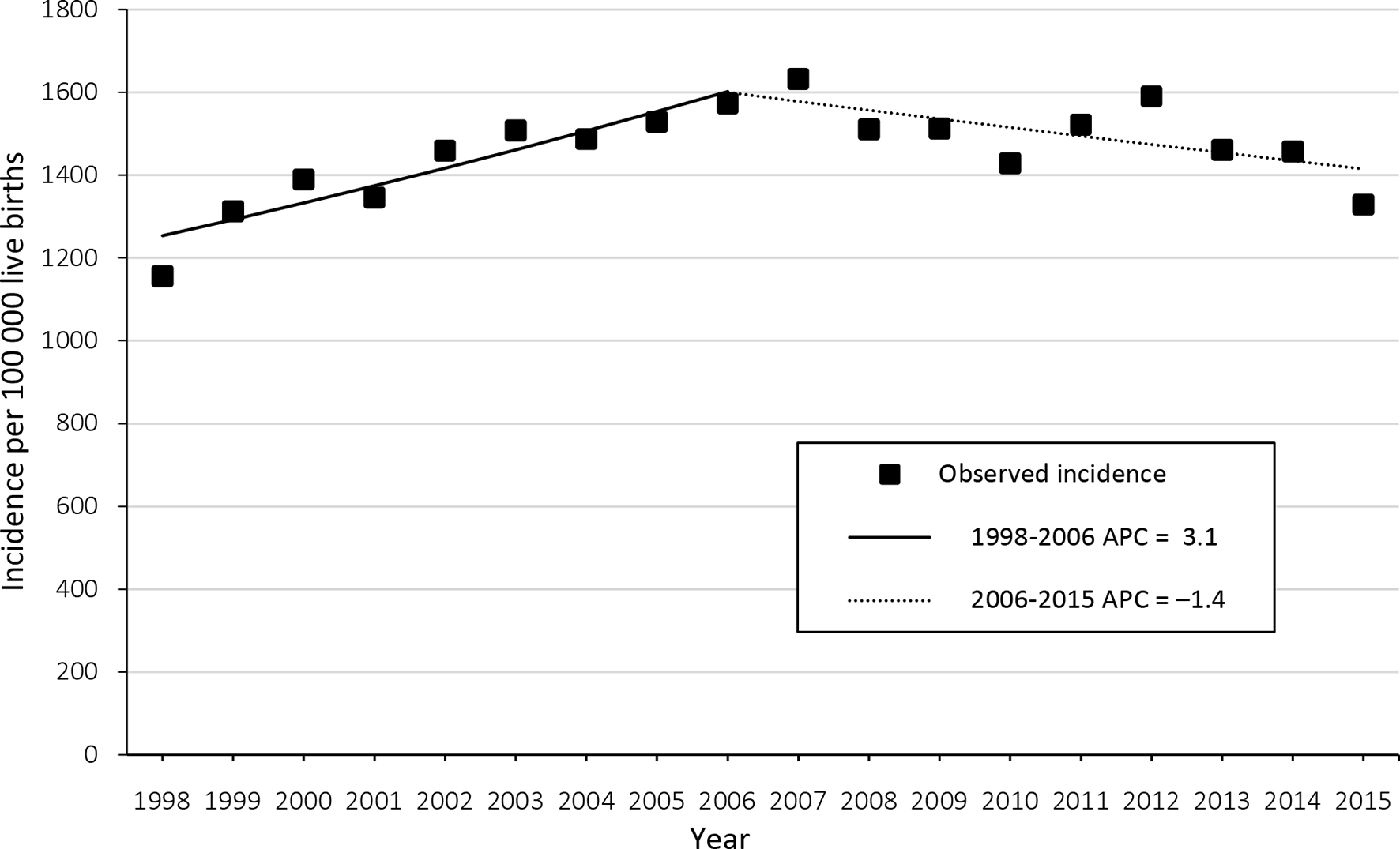
Incidence of births to hepatitis B virus (HBV)–infected women, by year of birth, New York City, 1998-2015. All annual percentage changes (APCs) are significant at α = .05. Data sources: New York City Perinatal Hepatitis B Prevention Program Surveillance Database, New York City Citywide Immunization Registry, and New York City Office of Vital Statistics. 25 -27
Trends in Incidence by Race
Among Asian women, the incidence of births to HBV-infected women per 100 000 live births increased significantly from 7010 in 2000 to 7849 in 2007 (APC = 2.2%; P = .003) but decreased to 5723 in 2015 (APC = –3.8%; P < .001) (Figure 2A). Among white women, the incidence declined significantly from 326 in 1998 to 263 in 2010 (APC = –2.6%; P = .001); however, we found no significant trend thereafter. Among black women, the incidence decreased from 1039 in 1998 to 639 in 2015 (APC = –1.1%; P = .05).
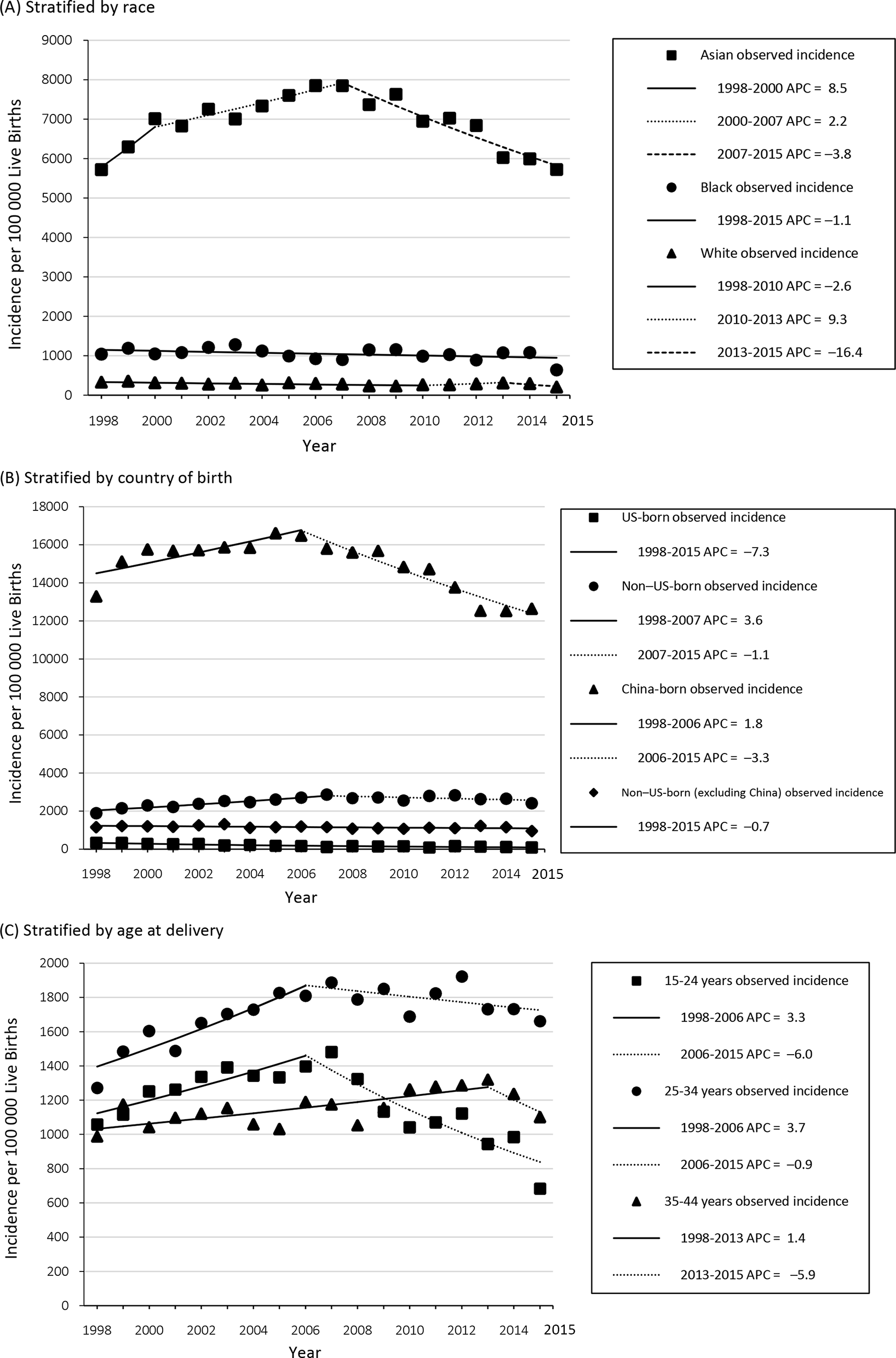
Incidence of births to hepatitis B virus (HBV)–infected women, by year of birth, stratified by maternal (A) race, (B) country of birth, and (C) age at delivery, New York City, 1998-2015. Data sources: New York City Perinatal Hepatitis B Prevention Program Surveillance Database, New York City Citywide Immunization Registry, and New York City Office of Vital Statistics. 25 -27 The following annual percentage changes (APCs) were significant at α = 0.05: Asian (2000-2007, 2007-2015) and white (1998-2010); US-born (1998-2015), non–US-born (1998-2007), China-born (1998-2006, 2006-2015), and non–US-born (excluding China) (1998-2015); age 15-24 years (1998-2006, 2006-2015), 25-34 years (1998-2006), and 35-44 years (1998-2013). Asian includes Asian and Hawaiian/Pacific Islander.
Trends in Incidence by Country of Birth
The incidence of births to HBV-infected women per 100 000 live births among US-born women was lower than among non–US-born women and decreased significantly from 330 in 1998 to 84 in 2015 (APC = –7.3%; P < .001) (Figure 2B). Among non–US-born women, the incidence increased significantly from 1877 in 1998 to 2864 in 2007 (APC = 3.6%; P < .001), but no significant changes occurred thereafter. Among women born in China, the incidence increased significantly from 13 275 in 1998 to 16 480 in 2006 (APC = 1.8%; P = .02). However, incidence among women born in China declined to 12 631 in 2015 (APC = –3.3%; P < .001). Among other non–US-born women not born in China, the incidence declined significantly from 1151 in 1998 to 945 in 2015 (APC = –0.7%; P = .01).
Trends in Incidence by Age at Delivery
Among women aged 15-24 at delivery, the incidence of births to HBV-infected women per 100 000 live births increased significantly from 1057 in 1998 to 1398 in 2006 (APC = 3.3%; P = .003) and then declined to 684 in 2015 (APC = –6.0%; P < .001) (Figure 2C). Among women who were aged 25-34 at delivery, the incidence also increased significantly from 1272 in 1998 to 1809 in 2006 (APC = 3.7%; P < .001), but no significant changes occurred thereafter. Among women aged 35-44 at delivery, incidence increased significantly from 988 in 1998 to 1320 in 2013 (APC = 1.4%; P < .001). Trends in incidence among women aged <15 and ≥45 could not be calculated because of small numbers.
Because the incidence of births to HBV-infected women was higher among non–US-born women from China than among US-born and other non–US-born women, we performed further stratification by age for women born in China (Figure 3). The overall decrease in incidence among women born in China from 1998 to 2015 (Figure 2B) was driven by a reduction in incidence among women aged 15-24; incidence in this age group declined significantly from 23 493 to 19 381 from 1998 to 2010 (APC = –1.5%; P = .001) with a steeper decline to 11 111 from 2010 to 2015 (APC = –9.9%; P < .001).
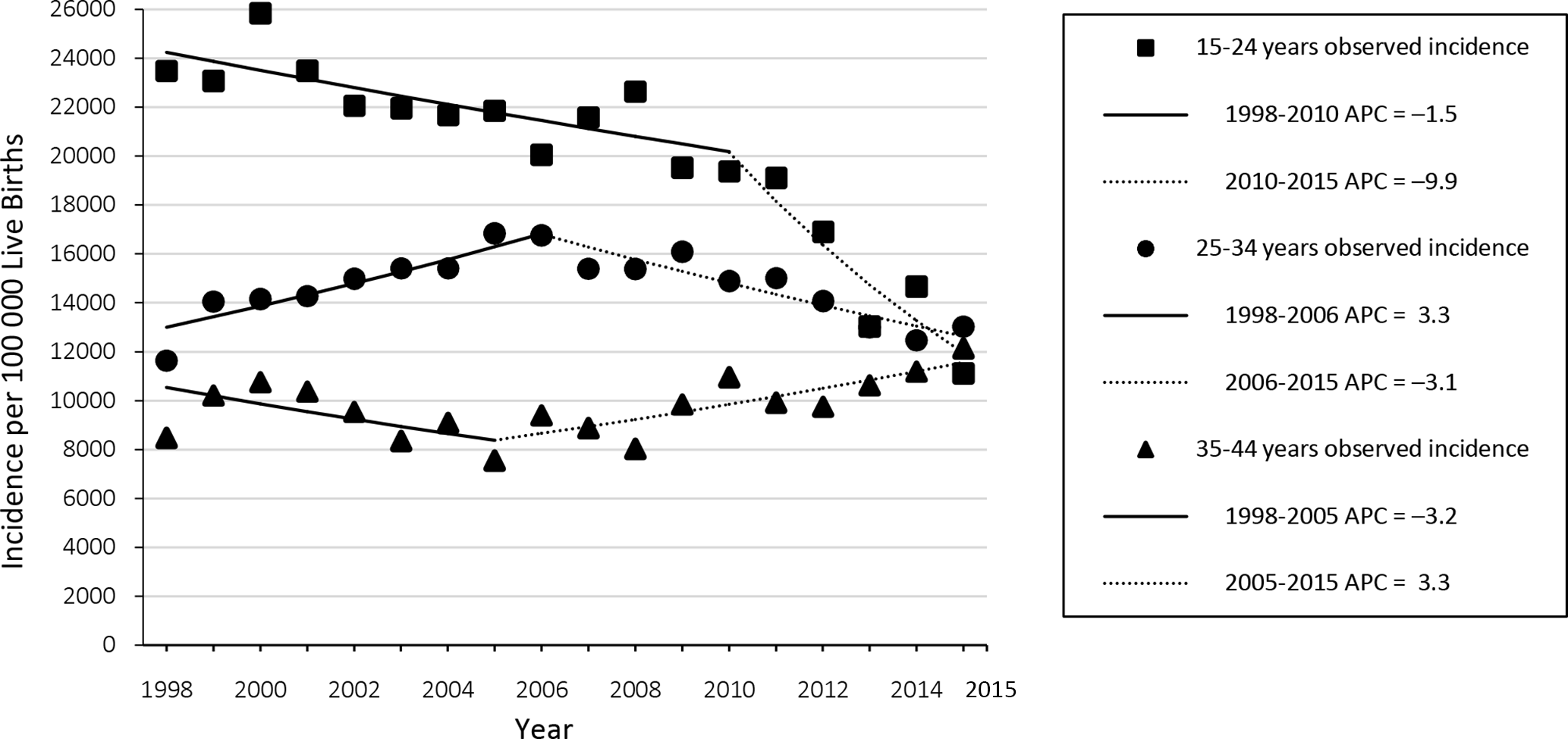
Incidence of births to hepatitis B virus (HBV)–infected women who were born in China, by year, stratified by age at delivery, New York City, 1998-2015. All annual percentage changes (APCs) were significant at α = .05 except age 35-44 (1998-2005). Data sources: New York City Perinatal Hepatitis B Prevention Program Surveillance Database, New York City Citywide Immunization Registry, and New York City Office of Vital Statistics. 25 -27
Discussion
The New York City PHBPP manages a caseload of a median 1670 births to HBV-infected pregnant women in New York City each year. The program also manages cases of women who relocate to New York City after giving birth or who reside in New York City but give birth elsewhere. The high volume of case management by the New York City PHBPP is attributed to the large and diverse population of New York City. New York City has >8.5 million residents, of whom 37% are non–US-born, as compared with 13% of the general US population. 28,29 Furthermore, 51% of all births in New York City are to non–US-born mothers, many of whom emigrated from regions of the world with a high prevalence of HBV infection. 28 Among non–US-born New York City residents, the largest immigrant populations are from the Dominican Republic (12%) and China (11%); however, immigration from China increased by 32% from 2000 to 2011, whereas growth in immigration from the Dominican Republic was 3% for the same period. 28 Such shifts in immigration patterns over time affect the population managed by the New York City PHBPP.
In our study, although the incidence of births to HBV-infected Asian women in New York City has declined since 2007, the incidence was 28 times that of white women as of 2015. The incidence among black women was 3 times that of white women. The differences in incidence among racial groups highlight a continued need for focused prevention activities. Although differences in incidence exist by race (eg, total incidence across the analysis period was 6903 per 100 000 Asian women vs 282 per 100 000 white women), these differences were amplified in comparisons across country of birth (eg, 14 812 per 100 000 women born in China vs 183 per 100 000 US-born women).
The incidence of births to HBV-infected US-born women is low, accounting for just 2% of all cases in the United States in recent years, and a decline in incidence has persisted. The decline in incidence of births to HBV-infected US-born women reflects the success of national vaccination efforts, which help to sustain a low overall prevalence of HBV among the general population of pregnant women in the United States. HBV vaccination has been routinely recommended in the United States for all infants since 1991 and all children since 1997. 9,10 In 2016, estimated coverage of 3-dose HBV vaccination was 90.5% (95% CI, 89.3%-91.5%) among children aged 19-35 months, and the rate of completion of the first dose of HBV vaccination within 3 days of life was 71.1% (95% CI, 69.5%-72.7%). 30
Conversely, the increase in incidence of births to HBV-infected non–US-born women through 2007 and a lack of significant change thereafter highlight a continued need for HBV vaccination programs worldwide, to decrease global HBV prevalence and prevent perinatal HBV infection in countries with high and low HBV prevalence. Ninety-four percent of all births to HBV-infected women in our analysis were to non–US-born women, and women who were born in China accounted for 57%-64% of births to HBV-infected women in recent years. The volume and incidence of births to HBV-infected women who were born in China were higher than among other non–US-born and US-born women in New York City.
However, we found a decline in the incidence of births to HBV-infected women aged <25 born in China who gave birth in New York City. Recent declines may indicate increased immigration from regions in China with a lower HBV prevalence; in China, the prevalence of HBV infection varies by province. 31 The decline in incidence of births among younger HBV-infected women born in China may also be the result of vaccination efforts in China that began with the introduction of hepatitis B vaccine for infants in 1992 and was made free of charge in 2002. 32 Declining incidence of births to HBV-infected women across older age groups may be observed in the future as well, as the cohort eligible to have received routine childhood HBV vaccination ages.
Strengths and Limitations
Our analysis had several strengths. First, the New York City PHBPP surveillance data analyzed have been evaluated and are considered to be almost complete; a capture–recapture analysis estimated that 96.5% of births to HBV-infected women were identified by the program for births from May 1, 2013, to May 1, 2014. 33 Second, we included 18 years of data in the analysis, representing a broader timeframe than in previously published analyses of the New York City program data; the broad timeframe of data included in our analysis increased our ability to detect trends within and across time segments. 34 Third, we enhanced completeness of data through matches with the Citywide Immunization Registry and New York City Office of Vital Statistics.
The study also had several limitations. First, we could not control for inconsistencies in data collection; data collection and completeness of case ascertainment may have improved over time given advancements in electronic disease surveillance systems and laboratory reporting of pregnancy status with hepatitis B test results, as well as improved health care provider knowledge of hepatitis B, HBV screening, and disease reporting requirements. Second, stratification by country of birth for countries other than China and the United States lacked sufficient case counts for analysis. Finally, we were unable to categorize selected maternal demographic data because of nondescript coding (eg, country of birth in the Office of Vital Statistics coded as “other Asia”), which may have affected stratified incidence calculations.
Conclusion
Perinatal hepatitis B prevention is a public health issue of high importance in New York City and requires ongoing public health surveillance and prevention activities. The persistence of HBV-infected pregnant women in New York City and the serious consequences of perinatal HBV transmission among infants indicate a continued need for PHBPP activities. These needs are particularly high among Asian women who were born in China.
Footnotes
Acknowledgments
The authors acknowledge the Perinatal Hepatitis B Prevention Program at the New York City Department of Health and Mental Hygiene for case identification, data collection, case management, health education, and public health prevention activities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists and funded by CDC (cooperative agreement #5U38HM000414-5).