
Abstract
Objectives:
The Care and Prevention in the United States Demonstration Project aimed to reduce HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in 8 states. We evaluated Health Models, a pay-for-performance program piloted by the Louisiana Department of Health that used financial incentives to improve rates of engagement in HIV medical care and viral suppression among people with HIV.
Methods:
We enrolled 2076 patients of 3 urban HIV specialty clinics in Louisiana in the Health Models pay-for-performance program on a rolling basis from September 2013 through September 2016 and gave patients cash incentives to attend HIV medical appointments, achieve or maintain viral suppression, and link to supportive services. We used laboratory data collected from Louisiana’s HIV surveillance database to calculate rates of engagement in care and viral suppression during the first 24 months of enrollment.
Results:
Of the 2076 patients who enrolled, 1400 (67.4%) were non-Hispanic black, 1480 (71.3%) were male, 1175 (56.6%) were men who have sex with men, and 1371 (66.0%) reported an annual income of <$15 000. At enrollment, 1456 (70.1%) patients were engaged in HIV care, and 1197 (57.7%) patients were virally suppressed. After 12 months of enrollment, 1474 of 1783 (82.7%) patients were virally suppressed. Of enrolled patients with at least 12 or 24 months of follow-up data, 1299 of 1317 (98.6%) patients were engaged in care during their first 12 months of enrollment, and 995 of 1033 (96.3%) patients were engaged in care between 12 and 24 months of enrollment.
Conclusions:
During the implementation of Health Models, enrolled patients had increases in rates of viral suppression and achieved rates of engagement in care and viral suppression that were higher than national levels; however, additional supportive services may be needed to further reduce socioeconomic disparities in the rates of viral suppression.
The National HIV/AIDS Strategy aims to improve health outcomes among people with HIV (PWH) and prevent new HIV infections by supporting strategies that help PWH maintain viral suppression through sustained engagement in HIV care and adherence to antiretroviral therapy (ART). 1 Maintaining viral suppression can prevent the onset of AIDS-related complications, such as opportunistic infections and death, and reduce the risk of HIV transmission to HIV-seronegative people. 2 -13 The Centers for Disease Control and Prevention (CDC) estimated that only 58% of PWH in the United States were virally suppressed in 2014. 14 Many PWH encounter socioeconomic barriers that prevent them from staying engaged in HIV care, adhering to ART, and maintaining viral suppression. 15 -19 Because HIV prevalence rates are highest among black people, gay or bisexual men, and transgender women, many barriers are highly correlated with social inequities and injustices that prevent these groups from achieving positive socioeconomic outcomes. Barriers include, but are not limited to, poverty, distrust of the health care system, and stigma tied to race, HIV status, sexual orientation, and gender nonconformity. 15 -27
Since the early 1990s, Louisiana has provided social support services and emergency direct assistance to PWH primarily through Ryan White HIV/AIDS Program federal funding to address these barriers and ensure access to HIV care and medication. Despite these efforts, 5303 of 18 533 (29%) PWH in Louisiana were not engaged in HIV care, and 3990 of 13 230 (30%) of those engaged in care were not virally suppressed in 2014. 28 These trends suggest that the barriers to sustained engagement in HIV care and adherence to ART in Louisiana are complex, and additional approaches are needed to increase the proportion of PWH who achieve and maintain viral suppression.
Research shows that pay-for-performance interventions, which provide financial incentives to people for modifying their health behavior and achieving positive health outcomes, may promote engagement in HIV care and adherence to ART among some PWH. 29 Financial incentives have been used to promote a range of healthy behaviors, including immunizations, screenings, smoking cessation, exercise, weight loss, and treatment plan adherence. 30 -35 Financial incentives primarily operate by providing a timely reward to reinforce the desired behavior and diminish the effects of opportunity costs associated with that behavior. 36,37 Opportunity costs are additional costs associated with choosing a desired healthy behavior rather than an undesired healthy behavior, such as paying for public transportation to attend an HIV care visit. In addition, financial incentives may directly address some poverty-related barriers to care and treatment adherence by helping recipients pay for transportation, medication copayments, meals, and lost wages incurred from taking unpaid leave from work to attend appointments. After repeatedly receiving financial incentives and showing improvements in HIV-related indicators (ie, achieving viral suppression), PWH may develop a greater sense of self-efficacy and establish new engagement-in-care and treatment adherence habits. 33
In November 2016, we identified 7 studies in the United States that had investigated the use of financial incentives to promote engagement in HIV care, adherence to ART, and viral suppression among PWH. Five of these studies provided financial incentives for attending appointments alongside patient navigation services (ie, limited case management and assistance with accessing other social services) and/or treatment adherence counseling, 2 concentrated solely on PWH who had substance use issues, and 4 were conducted as randomized controlled trials. 38 -45 In 4 studies, financial incentives had a positive effect on engagement in HIV care and adherence to ART. 35,40,43,44 Evidence to support the effect of financial incentives on viral suppression has been mixed. 38 -45 Five programs reported either no change in rates of viral suppression or unsustained, short-term increases in rates of viral suppression. 38,39,40,42,44 In one study, financial incentives had no overall effect on viral suppression for the study population but had a positive effect among subgroups that had the lowest rates of viral suppression before the program started. 39 However, the duration of these programs ranged from 16 weeks to 15 months, and the full effect of financial incentives on viral suppression may have occurred outside the data-collection periods. Furthermore, site-specific factors, such as the quality of care and other services provided at the clinic sites and the characteristics of the study population, may also have influenced the observed effectiveness of financial incentives in these studies. 38,39,42
In 2012, the Louisiana Department of Health, Office of Public Health, STD/HIV Program was awarded funding through the Care and Prevention in the United States Demonstration Project by CDC (PS12-1210) to develop and pilot innovative HIV prevention and care strategies that address HIV-related disparities among racial/ethnic minority groups. 46 We developed 6 such strategies, including Health Models, a demonstration pay-for-performance program (ie, a program that provides financial incentives for meeting certain performance measures) that evaluated the use of financial incentives to improve rates of engagement in HIV care and viral suppression among patients receiving care at 3 urban primarily Ryan White HIV/AIDS Program–funded HIV specialty clinics in New Orleans and Baton Rouge, Louisiana. We discuss findings from the first 3 years of Health Models implementation.
Program Description
The Health Models program was initially part of a multistrategy effort funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund for Care and Prevention in the United States Demonstration Project grant, which aimed to reduce HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in 8 states. 46 Implementation began in September 2013 and is ongoing. Patients are enrolled on a rolling basis as they visit clinics for HIV care. Patients receive financial incentives for initial or reengagement appointments, retention-related processes (ie, attending appointments and completing laboratory work), and most heavily for achieving and maintaining viral suppression (Table 1). Financial incentives are given as cash payments that are loaded onto reloadable debit cards. Health Models coordinators employed by each clinic manage and administer financial incentives; one clinic subsequently transferred these duties to nursing staff members. Health Models coordinators also provide enrollees with patient navigation services, treatment adherence counseling, and HIV health education. All HIV medical care patients aged >13 are eligible to enroll. Before implementation, the largest of the 3 clinics determined that it would have enough funding only to enroll half of its clinic population. In November 2013, Health Models staff members at this clinic began reviewing the electronic health records of patients with upcoming scheduled medical care appointments and targeting enrollment efforts to patients who had a history of missed appointments, treatment adherence issues, or other known barriers to staying engaged in care and maintaining viral suppression.
Incentive schedule for patients enrolled in the Health Models pay-for-performance programa at 3 urban HIV clinics, New Orleans and Baton Rouge, Louisiana, September 2013–September 2016
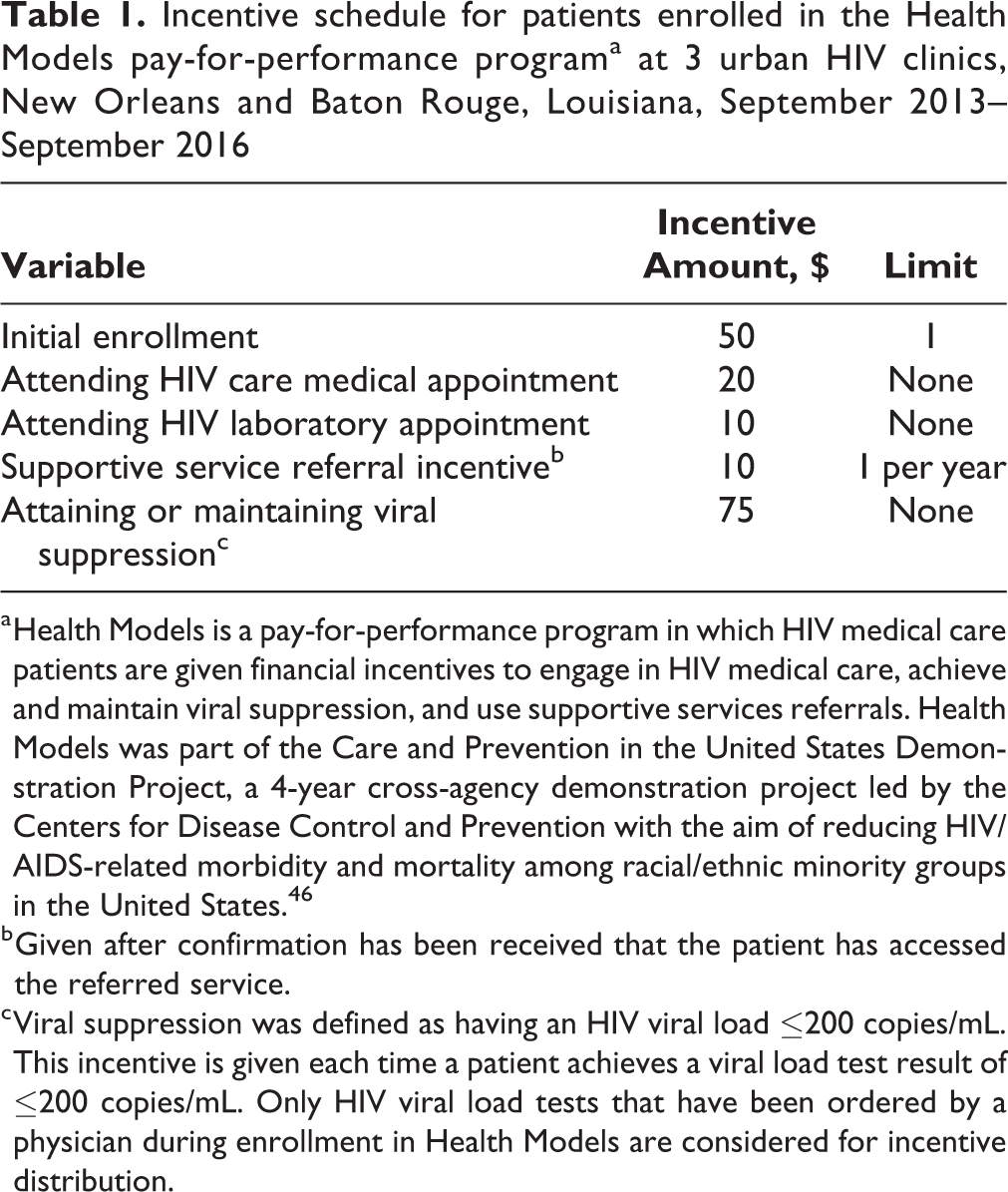
a Health Models is a pay-for-performance program in which HIV medical care patients are given financial incentives to engage in HIV medical care, achieve and maintain viral suppression, and use supportive services referrals. Health Models was part of the Care and Prevention in the United States Demonstration Project, a 4-year cross-agency demonstration project led by the Centers for Disease Control and Prevention with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 46
b Given after confirmation has been received that the patient has accessed the referred service.
c Viral suppression was defined as having an HIV viral load ≤200 copies/mL. This incentive is given each time a patient achieves a viral load test result of ≤200 copies/mL. Only HIV viral load tests that have been ordered by a physician during enrollment in Health Models are considered for incentive distribution.
The primary purpose of the evaluation was to assess the overall value and feasibility of the Health Models program by examining trends and disparities in rates of engagement in care and viral suppression, as well as the average dollar amount of financial incentives distributed per client, among patients enrolled in Health Models.
Methods
We collected data from September 30, 2013, through September 29, 2016, on demographic characteristics, including age (13-29, 30-39, 40-49, ≥50), sex (male, female, transgender female), and race/ethnicity (non-Hispanic black, non-Hispanic white, Hispanic/Latino, Asian, and non-Hispanic other/unknown); HIV transmission risk (ie, transmission between men who have sex with men [MSM], injection drug use [IDU], MSM/IDU, high-risk heterosexual contact, and other [eg, perinatal transmission, transmission from blood transfusion]); time since HIV diagnosis (<1 year, 1-4 years, ≥5 years); and results from HIV-related laboratory tests (CD4 count and HIV viral load) taken during the data-collection period from Louisiana’s HIV surveillance database (data frozen on December 9, 2016) to establish viral suppression and care engagement status. 47 We defined viral suppression as achieving a viral load ≤200 copies/mL, and we defined engagement in care as having at least 1 CD4 count or HIV viral load taken within a 12-month period before a specified date. We gathered self-reported data on ART use, personal annual gross income ($0-$14 999, $15 000-$29 999, ≥$30 000), and education (<high school degree, high school degree, some college, college degree) from the intake forms that clinic staff members completed for each patient during enrollment in Health Models.
The analysis included patients enrolled in Health Models during the data-collection period and nonenrolled patients who had at least 1 HIV-related laboratory test drawn at 1 of the participating clinics during the data-collection period. Patients were classified as nonenrolled if they received care at 1 of the participating clinics during the data-collection period but refused to go to the initial enrollment meeting with a Health Models coordinator, were offered an opportunity to enroll but refused the offer, or were not offered an opportunity to enroll (eg, the largest clinic prioritized patients who had a history of missed appointments, treatment adherence issues, or other known barriers because the clinic only had sufficient funding to enroll approximately half of its clinic population). To determine the degree to which the enrolled population represented the nonenrolled population, we compared demographic characteristics and baseline rates of viral suppression and engagement in care of both groups. We defined baseline as the initial enrollment date or the date of first laboratory test during the data-collection period for enrolled and nonenrolled patients, respectively. We used cumulative time since enrollment or time since first laboratory test during the data-collection period to calculate rates of viral suppression and engagement in care for enrolled and nonenrolled patients, respectively.
We used the Wald χ2 test to compare enrolled patients and nonenrolled patients by demographic characteristics, HIV transmission risk distribution, and baseline rates of engagement in care and viral suppression. We considered P < .05 to be significant. We restricted the numerator and denominator of the viral suppression rate to patients with viral loads taken within 12 months before baseline. We analyzed data by using SAS version 9.3. 48
We calculated rates of viral suppression after 6 months, 12 months, and 24 months of enrollment for enrolled patients using the results of the last viral load test taken within 12 months before the specified time points. We used the total number of enrolled patients who had at least 1 viral load test taken within 12 months before or on the specified time points as the denominators. We used the Wald χ2 test to detect significant differences in rates of viral suppression between subgroups at each time point. We calculated percentage-point differences for the enrolled population and for each subgroup to assess changes in rates of viral suppression after 6 months of enrollment, from 6 months to 12 months of enrollment, and from 12 months to 24 months of enrollment.
We determined rates of engagement in care for enrolled patients during 0 to 12 months of enrollment and during 12 to 24 months of enrollment by using all enrolled patients who were retained for at least 12 months and 24 months, respectively, as the denominators. We used the Wald χ2 test to determine significant differences in rates of engagement in care among enrolled patients by various subgroups. We considered P < .05 to be significant.
To calculate the average amount of financial incentives (in dollars) distributed per enrolled patient during the data-collection period and for each year during the data-collection period, we divided the total amount of financial incentives that were disseminated to enrolled patients during the respective time periods by the total number of patients who were retained by the end of the time periods. The Louisiana Department of Health Institutional Review Board approved this study.
Results
From September 30, 2013, through September 29, 2016, a total of 3934 patients with HIV received a CD4 count or an HIV viral load test from the participating Health Models clinics. Of these patients, 2076 (53%) enrolled in Health Models and 1858 (47%) did not enroll in Health Models because they were either not offered an opportunity to enroll or refused enrollment. Of the 2076 patients enrolled in Health Models, 1400 (67.4%) were non-Hispanic black, 1480 (71.3%) were male, 1150 (56.9%) were aged <40, 1175 (56.6%) were MSM, 1371 (67.8%) had an annual personal income <$15 000, and 1402 (67.5%) had ≤high school education (Table 2). At baseline, 1162 (56.0%) enrolled patients had been living with HIV for ≥5 years, 1456 (70.1%) were engaged in HIV care, 1385 (66.7%) were taking ART, and 1197 (57.7%) were virally suppressed. Enrollees were more likely than nonenrollees to be non-Hispanic black, transgender, aged <50, engaged in HIV care at baseline (all P < .001), and not virally suppressed at baseline (P = .01).
Characteristics of patients enrolled in the Health Models pay-for-performance programa at 3 urban HIV clinics, New Orleans and Baton Rouge, Louisiana, September 2013–September 2016

Abbreviations: —, not collected; IDU, injection drug use; IQR, interquartile range; MSM, men who have sex with men.
aHealth Models is a pay-for-performance program in which HIV medical care patients are given financial incentives to engage in HIV medical care, achieve and maintain viral suppression, and use supportive services referrals. Health Models was part of the Care and Prevention in the United States Demonstration Project, a 4-year cross-agency demonstration project led by the Centers for Disease Control and Prevention with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 46
bPatients who had a CD4 count or HIV viral load taken at a Health Models clinic during the study period but did not enroll in Health Models.
cThe Wald χ2 test was used to compare patients who enrolled in Health Models and those who did not. P < .05 was considered significant.
dOther risk is defined as risk of HIV transmission through perinatal transmission or transmission from blood transfusion. Unknown risk is defined as people with no reported HIV transmission risk in Louisiana’s HIV surveillance database. 47
eBaseline viral suppression status was determined by using the results of viral load tests taken closest to the enrollment date (within 12 months before through 12 months after initial enrollment) for enrolled patients and viral load tests taken nearest to the date of the first HIV laboratory test taken during the study period for nonenrolled patients. Baseline engagement-in-care status was determined by using HIV laboratory tests reported to the surveillance database that were taken within 12 months before the enrollment date for enrolled patients and HIV laboratory tests taken within 12 months before the date of the first HIV laboratory test taken during the study period for nonenrolled patients. 47
fOnly CD4 counts and HIV viral loads reported to Louisiana’s HIV surveillance database were considered when determining care engagement and viral suppression status. 47
gEnrolled patients with data on at least 1 HIV viral load or CD4 count taken during the 9 months before enrollment, or nonenrolled patients with data on at least 1 HIV viral load or CD4 count taken during the 9 months before the date of the first HIV laboratory test taken during the study period.
hEnrolled patients diagnosed with HIV within 9 months before enrollment who had no data on reported CD4 count or HIV viral load or nonenrolled patients diagnosed with HIV within 9 months before the date of the first HIV laboratory test taken during the study period who had no data on reported CD4 count or HIV viral load.
iEnrolled patients diagnosed with HIV more than 9 months before enrollment who had no data on reported HIV viral load or CD4 count within 9 months before enrollment, or nonenrolled patients diagnosed with HIV more than 9 months before the date of the first HIV laboratory test taken during the study period who had no data on reported HIV viral load or CD4 count within 9 months before the date of the first HIV laboratory test taken during the study period.
jMissing data for 40 enrollees. Data on use of antiretroviral medication at intake were not available for nonenrolled patients because data were captured during the intake process at the time of enrollment for enrolled patients, and non-enrolled patients did not undergo any intake process.
kViral suppression is defined as having an HIV viral load ≤200 copies/mL at last viral load taken within a 12-month period.
lTwo enrollees and 51 nonenrollees did not have data on HIV viral load taken at enrollment.
mMissing data for 54 enrollees. Data on personal income and education were not available for enrolled patients, because data were captured during the intake process at the time of enrollment for enrolled patients, and non enrolled patients did not undergo any intake process.
nPercentages do not total to 100 because of rounding. Data on highest education level were not available for nonenrolled patients because data were captured during the intake process at the time of enrollment for enrolled patients, and nonenrolled patients did not undergo any intake process.
Follow-up
By September 2016, 1968 of 2076 (94.8%) enrolled patients had been retained in Health Models for at least 6 months, 1827 (88.0%) for at least 12 months, and 1347 (64.9%) for at least 24 months (Figure). Compared with patients retained in Health Models for <6 months, patients retained for at least 6 months or at least 12 months were more likely to be aged ≥30 (P = .02, P = .01), not be MSM (P < .001 for both), engaged in care at baseline (P < .001 for both), taking ART at baseline (P < .001 for both), virally suppressed at baseline (P < .001, P = .009), and have an annual income ≥$15 000 (P = .02, P = .003). Compared with patients retained in Health Models for <24 months, patients retained for 24 months were more likely to be aged ≥30 (P = .003), be female (P = .03), be high-risk heterosexual or IDU (P = .005), be engaged in care at baseline (P < .001), be taking ART at baseline (P < .001), be virally suppressed at baseline (P < .001), have an annual income ≥$15 000 (P < .001), and have a high school diploma (P = .005).
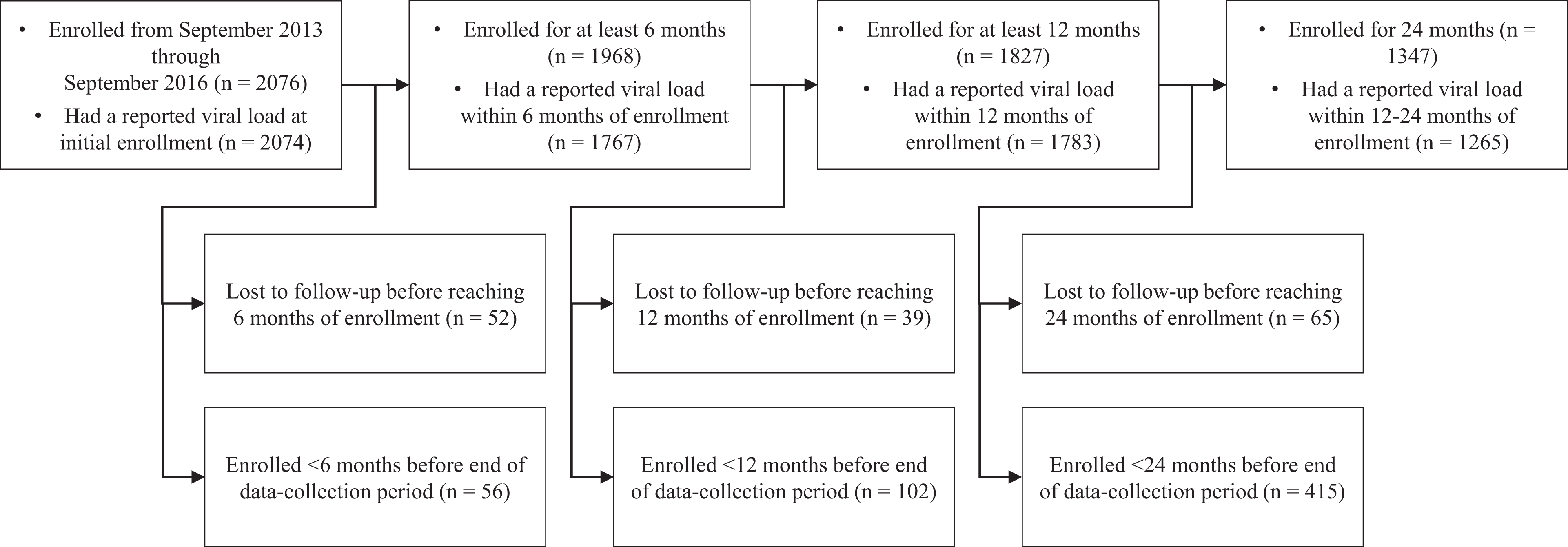
Follow-up outcomes for patients enrolled in the Health Models pay-for-performance program at 3 urban HIV clinics, New Orleans and Baton Rouge, Louisiana, September 2013–September 2016. Health Models is a pay-for-performance program in which HIV medical care patients are given financial incentives to engage in HIV medical care, achieve and maintain viral suppression, and use supportive services referrals. Health Models was part of the Care and Prevention in the United States Demonstration Project, a 4-year cross-agency demonstration project led by the Centers for Disease Control and Prevention with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 46
Incentives
Enrolled patients received 27 258 financial incentives from 2013 through 2016 totaling $850 855. The mean total financial incentive per client was $160.81. The mean annual total financial incentive per client increased by 15% from 2013-2014 ($155.24) to 2014-2015 ($183.68) and decreased by 28% from 2014-2015 to 2015-2016 ($143.52).
Viral Suppression
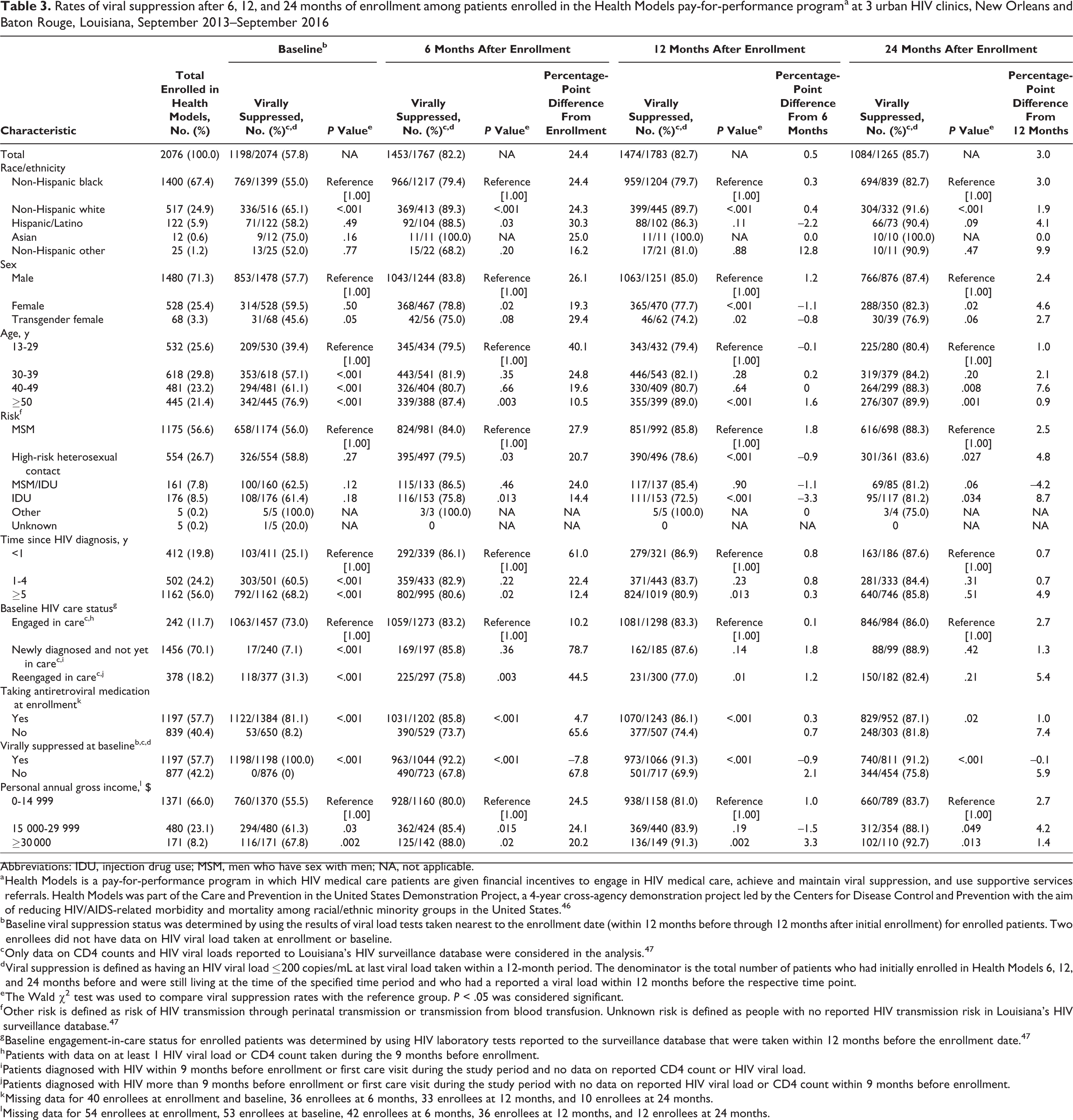
After 12 months of enrollment, the percentage of enrolled patients who were virally suppressed increased from 57.8% (1198 of 2074) to 82.7% (1474 of 1783; percentage-point difference = 24.9%, P < .001, Table 3). Every subgroup, except patients who were virally suppressed at baseline, had a substantial increase in rate of viral suppression during this interval (percentage-point difference range: 5.0%-80.5%). Subgroups with the greatest increases in rates of viral suppression included Hispanic/Latino people, transgender females, patients aged 13-29, MSM, patients diagnosed <1 year at baseline, patients not taking ART at baseline, and patients with an annual income <$15 000.
Rates of viral suppression after 6, 12, and 24 months of enrollment among patients enrolled in the Health Models pay-for-performance programa at 3 urban HIV clinics, New Orleans and Baton Rouge, Louisiana, September 2013–September 2016
Abbreviations: IDU, injection drug use; MSM, men who have sex with men; NA, not applicable.
a Health Models is a pay-for-performance program in which HIV medical care patients are given financial incentives to engage in HIV medical care, achieve and maintain viral suppression, and use supportive services referrals. Health Models was part of the Care and Prevention in the United States Demonstration Project, a 4-year cross-agency demonstration project led by the Centers for Disease Control and Prevention with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 46
b Baseline viral suppression status was determined by using the results of viral load tests taken nearest to the enrollment date (within 12 months before through 12 months after initial enrollment) for enrolled patients. Two enrollees did not have data on HIV viral load taken at enrollment or baseline.
c Only data on CD4 counts and HIV viral loads reported to Louisiana’s HIV surveillance database were considered in the analysis. 47
d Viral suppression is defined as having an HIV viral load ≤200 copies/mL at last viral load taken within a 12-month period. The denominator is the total number of patients who had initially enrolled in Health Models 6, 12, and 24 months before and were still living at the time of the specified time period and who had a reported a viral load within 12 months before the respective time point.
e The Wald χ2 test was used to compare viral suppression rates with the reference group. P < .05 was considered significant.
f Other risk is defined as risk of HIV transmission through perinatal transmission or transmission from blood transfusion. Unknown risk is defined as people with no reported HIV transmission risk in Louisiana’s HIV surveillance database. 47
g Baseline engagement-in-care status for enrolled patients was determined by using HIV laboratory tests reported to the surveillance database that were taken within 12 months before the enrollment date. 47
h Patients with data on at least 1 HIV viral load or CD4 count taken during the 9 months before enrollment.
i Patients diagnosed with HIV within 9 months before enrollment or first care visit during the study period and no data on reported CD4 count or HIV viral load.
j Patients diagnosed with HIV more than 9 months before enrollment or first care visit during the study period with no data on reported HIV viral load or CD4 count within 9 months before enrollment.
k Missing data for 40 enrollees at enrollment and baseline, 36 enrollees at 6 months, 33 enrollees at 12 months, and 10 enrollees at 24 months.
l Missing data for 54 enrollees at enrollment, 53 enrollees at baseline, 42 enrollees at 6 months, 36 enrollees at 12 months, and 12 enrollees at 24 months.
Subgroups with lower rates of viral suppression after 12 months of enrollment included non-Hispanic black patients compared with non-Hispanic white and Hispanic/Latino patients (both P < .001), female (P < .001) and transgender female (P = .02) patients compared with male patients, patients aged 13-29 compared with patients aged ≥50 (P < .001), high-risk heterosexual and IDU patients (both P < .001) compared with MSM, patients diagnosed with HIV ≥5 years before enrollment compared with patients diagnosed <1 year before enrollment (P = .013), patients reengaged in care at baseline compared with patients already engaged in care at baseline (P = .01), patients not on ART at baseline compared with patients on ART at baseline (P < .001), patients not virally suppressed at baseline compared with patients virally suppressed at baseline (P < .001), and patients with an annual income <$15 000 compared with patients with an annual income ≥$30 000 (P = .002). Almost all of the changes in rates of viral suppression during the first 12 months of enrollment occurred within the first 6 months of enrollment; overall rates of viral suppression did not change significantly from 6 to 12 months of enrollment or from 12 to 24 months of enrollment (Table 3).
Engagement in Care
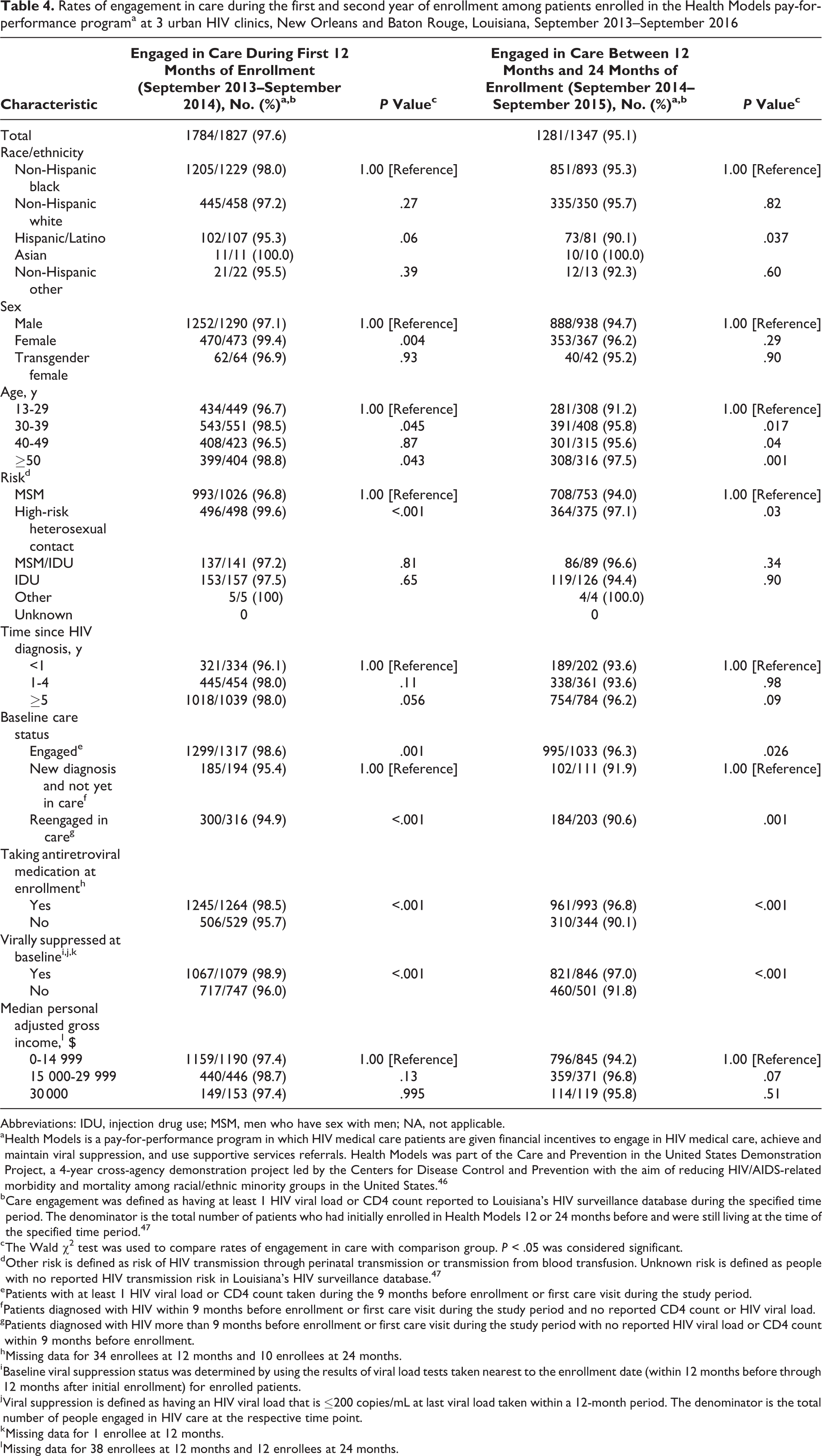
Of 1827 patients who were retained in care after 12 months of enrollment, 1784 (97.6%) had at least 1 CD4 count or HIV viral load during their first year of enrollment (Table 4). Of 1347 patients who were retained in care after 24 months of enrollment, 1281 (95.1%) were engaged in care between the first 12 and 24 months of enrollment. The rate of engagement in care for all subgroups was at least 90% between the first 12 and 24 months of enrollment.
Rates of engagement in care during the first and second year of enrollment among patients enrolled in the Health Models pay-for-performance programa at 3 urban HIV clinics, New Orleans and Baton Rouge, Louisiana, September 2013–September 2016
Abbreviations: IDU, injection drug use; MSM, men who have sex with men; NA, not applicable.
a Health Models is a pay-for-performance program in which HIV medical care patients are given financial incentives to engage in HIV medical care, achieve and maintain viral suppression, and use supportive services referrals. Health Models was part of the Care and Prevention in the United States Demonstration Project, a 4-year cross-agency demonstration project led by the Centers for Disease Control and Prevention with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 46
b Care engagement was defined as having at least 1 HIV viral load or CD4 count reported to Louisiana’s HIV surveillance database during the specified time period. The denominator is the total number of patients who had initially enrolled in Health Models 12 or 24 months before and were still living at the time of the specified time period. 47
c The Wald χ2 test was used to compare rates of engagement in care with comparison group. P < .05 was considered significant.
d Other risk is defined as risk of HIV transmission through perinatal transmission or transmission from blood transfusion. Unknown risk is defined as people with no reported HIV transmission risk in Louisiana’s HIV surveillance database. 47
e Patients with at least 1 HIV viral load or CD4 count taken during the 9 months before enrollment or first care visit during the study period.
f Patients diagnosed with HIV within 9 months before enrollment or first care visit during the study period and no reported CD4 count or HIV viral load.
g Patients diagnosed with HIV more than 9 months before enrollment or first care visit during the study period with no reported HIV viral load or CD4 count within 9 months before enrollment.
h Missing data for 34 enrollees at 12 months and 10 enrollees at 24 months.
i Baseline viral suppression status was determined by using the results of viral load tests taken nearest to the enrollment date (within 12 months before through 12 months after initial enrollment) for enrolled patients.
j Viral suppression is defined as having an HIV viral load that is ≤200 copies/mL at last viral load taken within a 12-month period. The denominator is the total number of people engaged in HIV care at the respective time point.
k Missing data for 1 enrollee at 12 months.
l Missing data for 38 enrollees at 12 months and 12 enrollees at 24 months.
Lessons Learned
Rates of viral suppression among Health Models enrollees increased during the first 12 months of enrollment in the program for all subgroups, although most increases occurred within the first 6 months of enrollment. The initial increase in rates of viral suppression was sustained through 24 months of enrollment for all subgroups. This finding is consistent with findings from other pay-for-performance programs that found most of the benefit in behavior modification attributed to financial incentives occurred within a relatively short period after enrollment. 30,31,42 In a separate qualitative analysis of staff member and provider attitudes and impressions of the program, staff members and providers at the participating clinics overwhelmingly reported improvements in rates of adherence to treatment and viral suppression and that clients generally seemed invested in their HIV management and motivated to achieve positive HIV health outcomes, such as viral suppression. 49
Most social disparities in rates of viral suppression that existed before enrollment persisted through 24 months of enrollment. However, some subgroups with disparately low rates of viral suppression at baseline had the largest gains in viral suppression through 24 months of enrollment in Health Models, including Hispanic/Latino people, transgender females, patients aged 13-29, patients diagnosed <1 year at baseline, patients not taking ART at baseline, and patients with an annual income <$15 000. We observed a similar trend in the results of a large randomized trial examining the effects of incentives on viral suppression among PWH in New York City and Washington, DC (HPTN 065). In that 2011-2013 study, compared with the control group, only subgroups with the lowest baseline rates of viral suppression had significantly higher increases in rates of viral suppression after receiving financial incentives. 39
Rates of viral suppression observed in Health Models patients through 24 months of enrollment were similar to or higher than rates of viral suppression found in national data. In 2017, CDC released surveillance data from 32 states and the District of Columbia and found that 80% of PWH who had at least 1 viral load in 2014 were virally suppressed 14 (compared with rates of viral suppression in our study of 57.8% at baseline, 82.2% at 6 months, 82.7% at 12 months, and 85.7% at 24 months).
Health Models patients had relatively high rates of engagement in care during the first 12 months and 24 months of enrollment (98% and 95%, respectively). These rates were higher than the engagement-in-care rate seen in the CDC study, in which only 73% of PWH who were diagnosed before or during the previous year were engaged in care. 14 In addition, during implementation of Health Models, clinic staff members reported that rates of missed appointments declined, clients developed relationships with staff members at the clinic for the first time, and clients became more invested in their HIV health. 49
Health Models was not designed as a research study with an appropriate control group or a randomized enrollment population because the US Department of Health and Human Services has a longstanding policy of not using the Secretary’s Minority AIDS Initiative Fund to fund research projects; consequently, a limitation of this evaluation was that the effects of Health Models on rates of viral suppression or engagement-in-care outcomes could not be determined, and other external factors may have influenced the observed results. However, all subgroups saw a significant increase in rates of viral suppression within 6 months of enrollment, and the improvement was sustained through 24 months of enrollment, including patients who were already engaged in care at enrollment. Another limitation of the study design was that the enrolled population did not represent the combined patient population of the participating clinics and may not represent PWH populations at other clinics. Patients enrolled in Health Models were significantly more likely than nonenrollees who received care at the same clinics to be non-Hispanic black, transgender, aged <50, engaged in HIV care at baseline (all P < .001), and not virally suppressed at baseline (P = .01). Therefore, the results observed during the Health Models program may not be generalizable to other clinics that provide HIV medical care.
Providing financial incentives for engagement-in-care and viral suppression outcomes was a valuable addition to the services provided at the clinics. During Health Models enrollment, enrolled patients had increases in rates of viral suppression and achieved rates of engagement in care and viral suppression that were higher than national levels. Additional supportive services may be needed to further reduce social disparities in rates of viral suppression. Although the effect that discontinuation of the financial incentives would have on participants’ HIV care outcomes is unknown, the per-patient investment was relatively low and potentially allowed for long-term operation of the program in a similar fashion to other long-standing, federally funded supportive services offered to PWH.
Because of additional funding sources, the program is ongoing at the original 3 HIV care clinics and has expanded to 1 additional site in New Orleans. Viral suppression and engagement-in-care outcomes will continue to be monitored.
Footnotes
Acknowledgments
The authors thank the current and former staff members of the Louisiana Department of Health, Office of Public Health, STD/HIV Program, and the clinic sites that played an integral role in the implementation of Health Models, including Karen Bennett, Lara Jackson, Jessica Scott, Pacience Smith, and Tammy Wells. The authors also acknowledge the assistance of the Care and Prevention in the United States Louisiana site team: Ted Duncan, Laura Kearns, Mesfin Mulatu, Alexandra Oster, Thomas Painter, Raekiela Taylor, and Kim Williams (CDC site team members); Kirk James (Substance Abuse and Mental Health Services Administration site team member); and William Bryant (Health Resources and Services Administration site team member).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Care and Prevention in the United States (CAPUS) Demonstration Project was led by the Centers for Disease Control and Prevention (CDC; PS12-1210) and supported by the US Department of Health and Human Services (HHS) Secretary’s Minority AIDS Initiative Fund in the amount of $1 947 670 awarded to the Louisiana Department of Health, Office of Public Health, STD/HIV Program. The information or content and conclusions of this article are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by, HHS, CDC, or the US government.