
Abstract

Thanks to assiduous public health efforts, the overall annual rate of perinatal HIV transmission has decreased. In the United States, 44 infants acquired HIV perinatally in 2014, down from 71 in 2012. 1 Mother-to-child (perinatal) HIV transmission is preventable 2 : the risk of perinatal HIV transmission can be reduced to <2% if a woman receives antiretroviral therapy (ART) during pregnancy and avoids breastfeeding and if the infant receives prophylaxis soon after birth. 3 If a mother has HIV diagnosed during labor, treatment as late as the intrapartum period can reduce the rate of transmission from 25.5% to 10.0%. However, beginning prophylaxis 3 or more days after birth does not substantially reduce the risk of contracting HIV. 4 Thus, identifying HIV infection early, through HIV testing of pregnant women and newborns, can help provide essential and timely linkage to care for mother and child. 5
The Centers for Disease Control and Prevention (CDC) recommends that pregnant women undergo opt-out HIV testing as early as possible during each pregnancy. “Opt-out testing” refers to the practice of routinely testing for HIV after informing the woman that the test will occur and that she may decline testing. 6 Consent is inferred unless the patient declines testing. Under CDC’s 2006 recommendations, a second HIV test during the third trimester, preferably before 36 weeks of gestation, may be suggested. A second HIV test during the third trimester is recommended for women who (1) receive health care in jurisdictions with an elevated incidence of HIV or AIDS (≥17 HIV cases per 100 000 women aged 15-45), (2) receive health care in facilities in which at least 1 HIV-infected pregnant woman is identified for each 1000 women screened, (3) are known to be at high risk for acquiring HIV, or (4) have signs or symptoms consistent with acute HIV infection. 6
Moreover, repeat testing during pregnancy is cost-effective in jurisdictions with low and high HIV prevalence. 6,7 A second HIV test identifies recent HIV seroconversion (ie, acute HIV infection during pregnancy) and affords a window of opportunity to provide ART to the mother for her own health and to prevent perinatal HIV transmission. 7 CDC recommends screening of women whose HIV status is unknown at the time of labor. CDC also recommends that women whose HIV status is still unknown at the time of delivery be screened immediately postpartum. If the mother’s HIV status is unknown postpartum, the newborn should undergo HIV testing as soon as possible after birth. 6 Testing the newborn helps identify infants who can benefit from a regimen of 2 or 3 ART drugs. 8
A first step in determining whether perinatal HIV testing laws are associated with reductions in mother-to-child HIV infection is to identify the laws on such testing in each state. Two studies evaluated the consistency of state HIV testing laws with the consent and counseling components of the CDC HIV testing recommendations. 9,10 However, only 1 study focused on repeat HIV testing in pregnancy. That 2016 Maryland study found that only about 28% of pregnant women were retested for HIV during pregnancy. 11 The purpose of our analysis was to determine the consistency between state statutes and regulations on HIV testing of the mother during the third trimester (including initial and repeat tests) and during labor and delivery, and of the newborn, with 9 of the CDC perinatal HIV testing recommendations.
Methods
From September 1, 2016, through November 30, 2016, we searched the online legal research service Westlaw Next (https://next.westlaw.com) by using Boolean terms and connectors (adv: TI, TE(h.i.v. “human immuno-deficiency virus” & pregnan! newborn)) to find any statute or regulation in all 50 states and the District of Columbia that explicitly mentioned HIV testing in pregnant women or in newborns. We consulted a third public health analyst and individually assessed each law for the 9 recommendations. The overall divergence rate, or difference in assessments, was <1%. We calculated the divergence rate by dividing the total number of divergent answers by the total number of answers (2/279 = 0.7%). We resolved discrepancies by consensus.
For this analysis, we grouped state statutes and regulations on perinatal HIV testing into categories corresponding to the CDC perinatal HIV testing recommendations. We categorized statutes and regulations as addressing (1) HIV testing in the newborn if the mother’s HIV status was still unknown at the time of delivery, (2) HIV testing for women with unknown HIV status at labor and delivery, (3) repeat HIV testing in the third trimester, and (4) both HIV testing in the third trimester (repeat) and in the newborn.
We also further categorized statutes and regulations on repeat third-trimester testing into 2 subcategories requiring repeat testing for all women and for women at high risk (Table). We categorized statutes and regulations addressing women at high risk as those addressing (1) repeat testing for women at higher individual risk, (2) repeat testing where HIV prevalence in the patient population was elevated in a care setting or in the entire jurisdiction, and (3) repeat testing for women who had signs or symptoms consistent with acute HIV infection.
Perinatal HIV testing statutes and regulations, by state, as of November 30, 2016
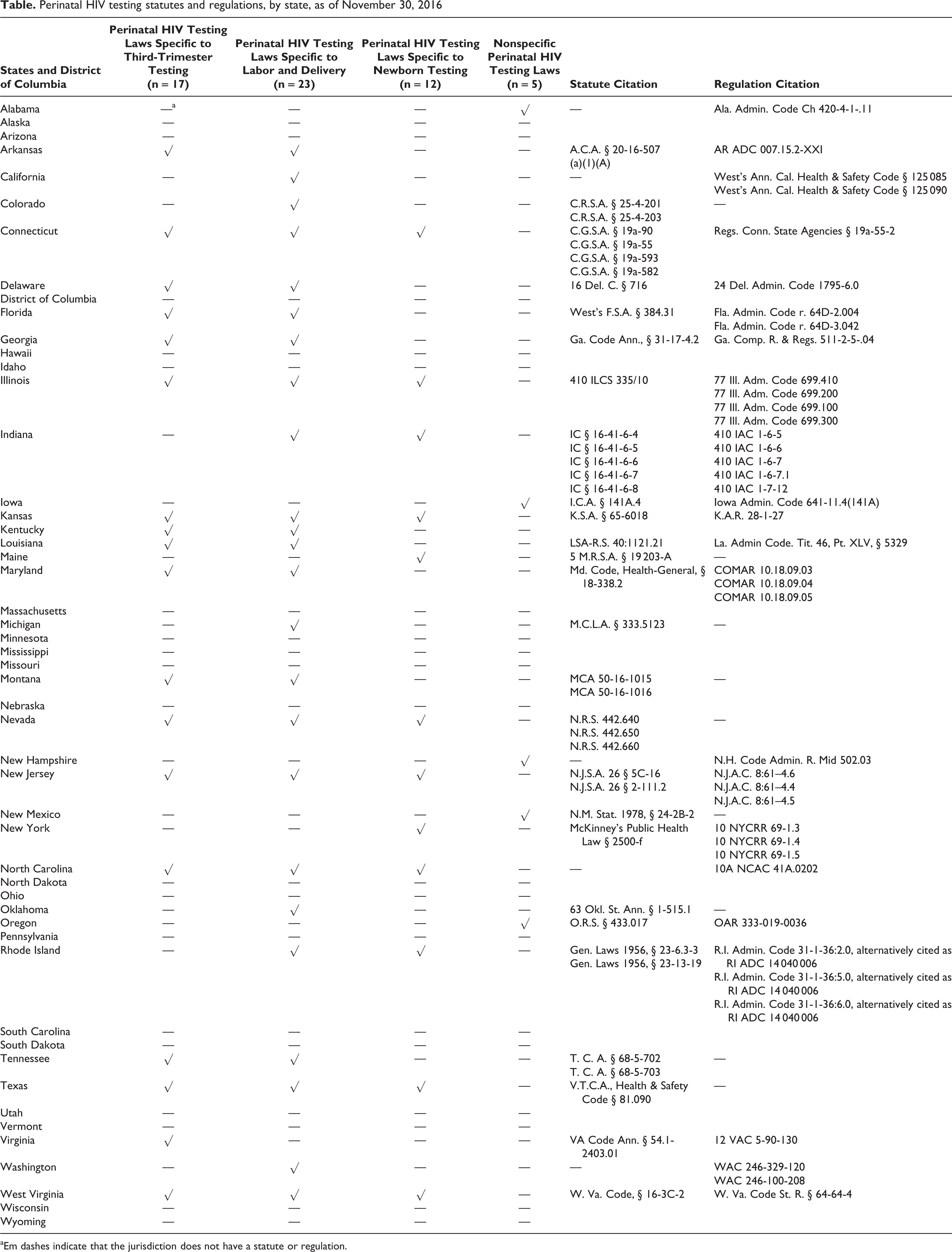
aEm dashes indicate that the jurisdiction does not have a statute or regulation.
We additionally subclassified statutes and regulations on repeat testing where HIV prevalence in the patient population was elevated into those addressing repeat testing where HIV prevalence in the patient population was (1) elevated in a care setting, (2) elevated in the entire jurisdiction, and (3) elevated in a care setting or in the entire jurisdiction.
Following CDC’s recommendations, we identified states with the most comprehensive statutes and regulations on perinatal HIV testing as those addressing testing (1) in the third trimester for all pregnant women or for women at high risk, (2) during labor and delivery for women with an undocumented HIV test, and (3) for newborns if the mother’s HIV status was unknown.
Results
As of November 30, 2016, half of the states (n = 26) had enacted statutes and regulations addressing perinatal HIV testing (Table). Eight states addressed repeat testing in the third trimester, newborn testing when the mother’s HIV status was unknown, and HIV testing for women with no documented HIV test during labor and delivery, making them the states with the most comprehensive statutes and regulations on perinatal HIV testing: Connecticut, Illinois, Kansas, Nevada, New Jersey, North Carolina, Texas, and West Virginia.
Discussion
We found that, as of November 2016, perinatal HIV testing was still not widely incorporated into state statutes and regulations. Only 26 states had enacted statutes and regulations addressing some form of perinatal HIV testing, and only 8 states had comprehensive perinatal HIV testing statutes or regulations. Biomedical advances have helped to greatly reduce the number of perinatal transmissions. However, whether incorporating CDC’s recommendations into more state statutes and regulations would further reduce HIV incidence is unknown.
Implementing CDC’s recommendations is voluntary. Little information is available on whether or how health care providers are implementing recommended perinatal HIV testing. However, statutes and regulations can represent the moral standards of society. Including perinatal HIV testing in state statutes and regulations can signify the importance of stopping the spread of HIV within a given state. However, whether statutes and regulations increase the likelihood of testing is unknown.
The existence of state statutes and regulations on newborn and third-trimester HIV testing does not provide any information on whether newborn or third-trimester HIV testing is actually practiced in care settings. However, the existence of state statutes and regulations on this subject does indicate that state legislatures recognize perinatal HIV screening as a valuable HIV prevention tool and can set the tone for clinical implementation by reinforcing expectations and responsibilities.
Detailed reporting of perinatal HIV testing in the United States can help researchers understand whether this key HIV prevention measure is being widely applied in care settings. Once the needed data on perinatal HIV testing in the United States are available, this legal epidemiology study may help determine whether the existence or lack of perinatal HIV testing statutes and regulations is a factor in perinatal HIV transmission.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. It does not constitute legal advice nor is it intended to support or oppose any proposed or pending federal, state, or other law.
Acknowledgments
The authors thank Lauren FitzHarris and Caitlin Leach for their valuable input.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.