
Abstract
Public safety personnel (PSP) are at increased risk of developing operational stress injuries. Peer-led reintegration programs (RPs) for PSP, evidence-based research is lacking. This study explored the experiences of PSP participating in a Reintegration Program Facilitator Training (RPFT) program. Participant (n = 57) responses were collected from surveys, satisfaction and knowledge questionnaires, and a World Cafe. Four themes emerged: (1) traits of an ideal RF; (2) holistic/complementary workplace reintegration approach; (3) necessary features of the reintegration program; and (4) culture-specific considerations. While RPs hold promise, it is essential that evidence-based research be used to guide RPFT and RP spread and sustainability.
Introduction
Occupational stress injuries in police and public safety personnel
The demands and stressful nature of police work, unpredictability of the calls to which officers respond, and exposure to traumatic events in the line of duty that can include death, violence, and threats to their own lives, can contribute to the development of operational stress injuries (OSIs) (Carleton et al., 2019). OSIs include a broad range of conditions including mental disorders and conditions that interfere with daily functioning in social, work, or family activities (Canadian Institute for Public Safety Research and Treatment, 2019). Police officers also experience increased risk of psychological challenges, including post-traumatic stress disorder (PTSD), depression, anxiety, and anger, which can lead to other challenges such as substance abuse, relationship difficulties, and workplace absenteeism (Beshai and Carleton, 2016). A 2018 study found that 36.7% of surveyed Canadian police officers screened positive for a mental health condition— primarily PTSD (Carleton et al., 2018). Such injuries can leave officers unable to return to work in their required capacity or at all (Beshai and Carleton, 2016). Even with extensive multidisciplinary rehabilitation, only a minority of public safety personnel (PSP; police officers, firefighters, dispatchers, emergency medical workers, corrections officers, etc.) return to pre-accident work levels, and PSPs may be more likely than non-PSP workers to require ongoing wage replacement benefits (Gross et al., 2021).
Despite awareness that OSIs among police officers is a widespread issue, research and services for officers and their families are lacking. Studies related to return-to-work initiatives for police officers and other PSP remain scarce (Beshai and Carleton, 2016). In Canada, a key recommendation of the landmark “Blue Paper” report (Beshai and Carleton, 2016) was to: "Participate in research studies and ongoing evaluations examining the effectiveness of peer support or crisis-focused psychological intervention programs with appropriate sample sizes, empirically supported outcome measures, and using methodologically rigorous designs, such as randomized controlled trials and longitudinal studies. First Responder organizations should seek to have such research conducted with independent, established researchers who have been appropriately vetted by, and are currently explicitly supported by, established and accredited research organizations" (p. 8). Peer-support programs are recognized as a key component of an overall work reintegration strategy for PSP organizations; however, higher quality reintegration program effectiveness studies that incorporate stronger study designs, rigour, validity, and reliability are needed to determine long-term effectiveness (Beshai and Carleton, 2016).
Peer-support programs: Current evidence
Peer support is a benevolent relationship that is based on a shared lived experience, such as similar employment and/or exposure to traumatic events. A peer supporter may provide emotional, spiritual, and/or social support (Sunderland and Mishkin, 2013). Peers with similar experiences are valued for their authenticity as they can relate to the challenge and may have seen success with their own recovery (Sunderland and Mishkin, 2013). As a result, peers may be more likely to trust one another and disclose information that they would not share with healthcare professionals, friends, or family.
A key aspect to the efficacy and “buy-in” of peer support programs is the manner in which peer team members maintain trust, confidentiality, and anonymity for police officer peers who are seeking assistance (Van Hasselt et al., 2019). Page and Jacobs (2011) found that close to three out of four police officers would prefer speaking with another police officer over a mental health therapist. The peer-support process is thought to be effective at reducing psychological distress by identifying and referring those at risk for developing PTSD thus resulting in early appropriate treatment for those experiencing trauma (Watson and Andrews, 2018). Once engaged in intervention, it has been reported that police officers preferred to seek mental health services from professionals who belonged to the police organizations rather than from those who worked outside of the organization (Andersen et al., 2015).
Peer-support programs offer police officers a confidential outlet to share private information without feelings of judgment and encourage a sense of community (Milliard, 2020). Previous research has found that peer-support programs are a way to promote mental health literacy and health-seeking behaviors and are effective in reducing stigma (Andersen et al., 2015; Milliard, 2020; Van Hasselt et al., 2019). A scoping review by Richins et al. (2020) also found that peer support is important in normalizing emotions and reactions. When offered in a group format, peer support was found to facilitate individual recovery and made for a better experience, thus highlighting the role of social support and social cohesion in the psychological processing of traumatic experiences.
A number of PSP peer-support programs exist globally, with varying aims, purposes, and formats across diverse PSP organizations. The objectives of peer-support programs may include critical incident stress debriefing, critical incident stress management, peer support, psychological first aid, and trauma risk management (Anderson et al., 2020). Such programs are delivered in community, clinical, and workplace contexts in both group and one-to-one formats (Sunderland and Mishkin, 2013). Peer-support programs may be introduced prior to, during or upon conclusion of clinical interventions, and the person’s return to work and may be the first step a person takes toward recovery.
Evidence for the effectiveness of peer support programs, although scarce, is noteworthy. In a scoping review by Richins et al. (2020), it was reported that peer-based or peer-led interventions that included peer-group debriefings led to significant reductions in trauma-related absenteeism. Early interventions in a group format found that peer support facilitated recovery. Social support and cohesion were found to be supportive of the psychological processing of traumatic experiences, normalizing emotions and reactions, and potential reintegration into the workplace. While these findings suggest there are many benefits to peer-support programs, the importance of standards and governance of such programs was emphasized in order to ensure risk management and best practices (Milliard, 2020). Although the evidence for the success of peer-support programs is promising, there has been limited investigation into any specific peer-led programs and their efficacy with trauma-affected PSP, as well as others who are returning to work after injury.
Edmonton Police Services Reintegration Program
In 2009, the Edmonton Police Service (EPS) identified a need to assist police officers who were off work following a critical incident such as an officer-involved shooting. Initially, workplace reintegration efforts after critical incidents involved providing officers with peer-supported assistance to help them regain confidence with firearms and staged policing-specific activities that could not be accomplished within a clinical setting. Over time, the EPS Reintegration Program (EPSRP) evolved, inclusive of peer support. Today, the primary goal of EPSRP is to help officers return to work as soon as possible following a critical incident, illness, or injury, while diminishing the potential for long-term psychological injury (Edmonton Police Service, 2018).
EPSRP is delivered by peers through three interrelated components: (1) Reintegration Program Facilitator Training (RPFT) Program; (2) a short-term Critical Incident Reintegration Program (RP); and (3) a long-term Critical Incident RP (Edmonton Police Service, 2018). Inclusive of relationship-building, reintroduction to equipment, skill-building, exposure therapy, and street exposures (Edmonton Police Service, 2018), the participating individual is guided by a trained peer PSP Reintegration Facilitator (RF) through a step-by-step process that addresses the unique stressors that the officer may experience. The pace, scope, depth, and goals of the program are determined by the individual. EPS’s short-term reintegration program includes an initial meeting with the officer, physical dexterity of firearm, acclimation to gunfire, live fire, officer-directed training, reintroduction, and follow-up. To assist officers who have been off work for an extended period, the long-term reintegration program provides them with support and training to return to the work setting. Supports offered by the RFs are complementary to traditional therapies but outside the scope of what officers receive from their healthcare providers (i.e., psychologists, clinicians, or occupational therapists) (Edmonton Police Services, 2018). RPs such as the EPSRP may assist Workers Compensation organizations to facilitate positive outcomes for officers attempting to return to duty after developing an OSI such as PTSD.
Edmonton Police Service offered the 5-day RPFT program on an annual basis for PSP who were interested in becoming RFs and/or implementing an RP within their organization. The training includes both psychoeducational and experiential components. Examples of psychoeducational topics include the physiological effects of trauma, basic neuroanatomy and physiology, mental health disorders, specific counseling drills, and interpersonal skills such as active listening. Examples of hands-on graded activities that may be utilized include firearms exposures on the firing range for police, mock interrogations for border patrol personnel, donning of equipment for firefighters, and specific scenarios in an ambulance for paramedics. This training has been offered within the provinces of Alberta and Ontario in Canada as well as in Wellington, New Zealand. Although the anecdotal reports and current literature regarding peer-supported initiatives are promising, the EPSRP has yet to be rigorously studied.
In April of 2019, a pilot study was initiated with the purpose of evaluating the effectiveness of the EPS RPFT course at increasing mental health knowledge and shifting attitudes of RPFT attendees. The qualitative component of the mixed methods pilot study captured changes in the mental health knowledge, attitudes, and stigma of RPFT participants. In this article, we present the results of the thematic analysis conducted on the open-text qualitative answers to pre-post screening questionnaires, responses to daily questionnaires from the 5 days of training, and field notes captured during a World Cafe on the final day of the RPFT course.
Purpose
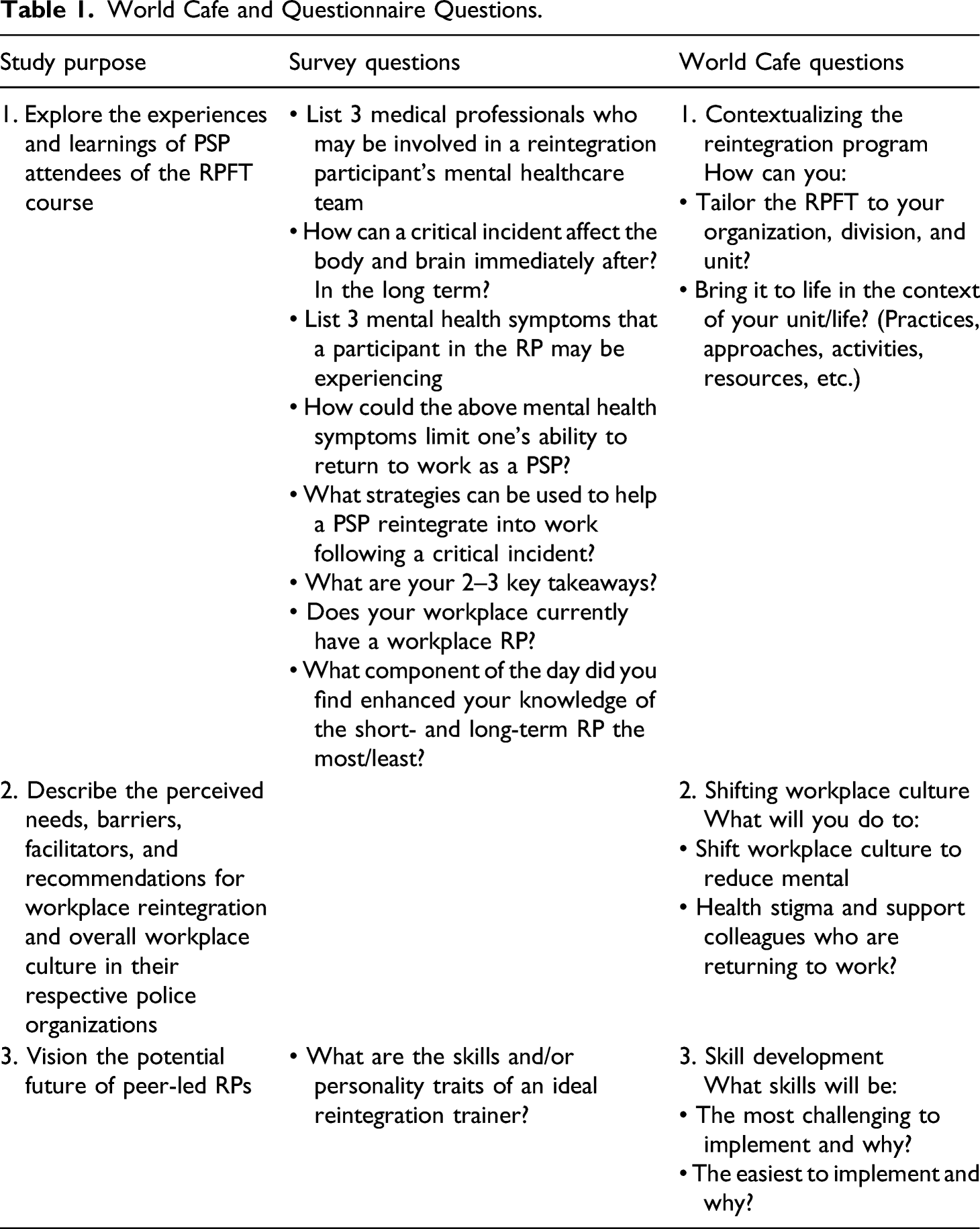
The purpose of the qualitative component of this study was to (1) explore the experiences and learnings of PSP attendees of the RPFT course; (2) describe the perceived needs, barriers, facilitators, and recommendations for workplace reintegration and overall workplace culture in their respective police organizations; and (3) vision the potential future of peer-led RPs. The qualitative findings represent an important part of the RP discourse and contribute to increasing our overall knowledge of the role of peer-support programs.
Methods
Study design
This qualitative study was part of a larger mixed methods pilot project which employed a convergent parallel design. Concurrent collection of quantitative and qualitative data and triangulation occurred once all data were collected. This study received ethical approval from the University of Alberta Research Ethics Board and was supported by the EPS.
Recruitment and sample
Participants (n = 57) included Alberta-based PSP (e.g., RCMP, police, EMS, fire, sheriffs, and corrections officers) and clinicians (psychologists and occupational therapists) working with PSPs who attended the EPS RPFT. The participants voluntarily signed up to attend the 5-day RPFT course and obtained approval to participate from their employers. Recruitment occurred in the week prior to and morning of the start of the RPFT course. Upon registering in the course, attendees were asked by the Course Coordinator if they were interested in participating in the study; those interested were enrolled, and prior to commencing the RPFT, provided written and verbal consent.
Data collection
World Cafe and Questionnaire Questions.
Data analysis
Braun and Clark’s (2006) method of thematic analysis (deductive and inductive) was utilized to analyze the open-ended survey questions and the World Cafe data. Thematic analysis provides a flexible method for identifying, analyzing, and reporting themes in rich detail (Braun and Clarke, 2006). An audit trail allowed the research team to review and examine decision making around themes, as well as maintain credibility and rigor. Informed by the study purpose, data analysis began with all research team members reading and discussing the World Cafe transcripts and open-ended survey responses. Initial open codes were then developed using an inductive approach. The codes were combined into preliminary themes that focused on similarities and differences within and between the World Cafe and qualitative survey questions. Preliminary themes underwent a secondary round of collective analysis by all the authors, with differences resolved through discussion. Final themes aimed to reflect a more nuanced and rich understanding of the data.
Results
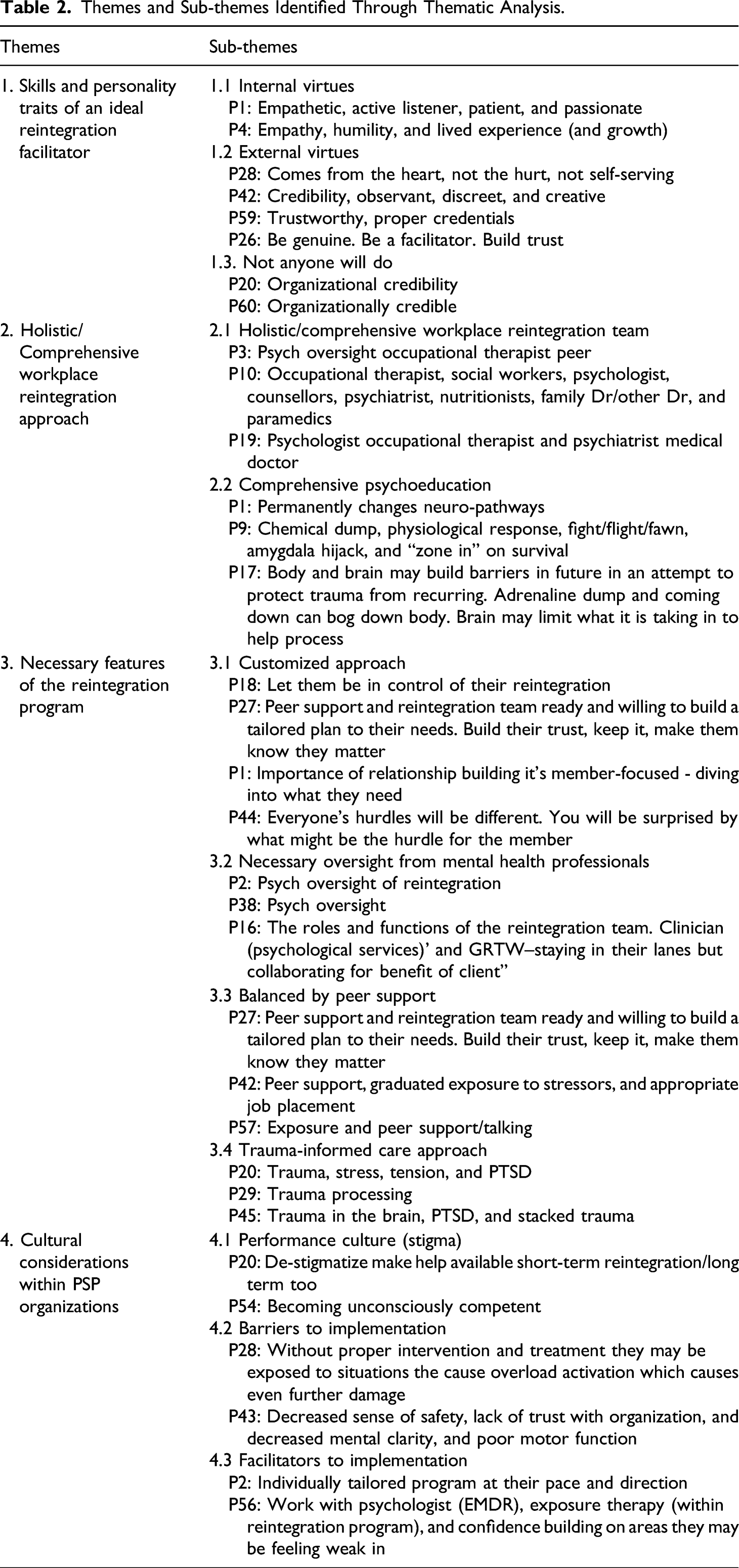
Themes and Sub-themes Identified Through Thematic Analysis.
Theme 1: Skills and personality traits of an ideal reintegration facilitator
Participants identified specific skills and personality traits that make an individual an ideal RF, including the need for strong internal and external virtues. They also clearly asserted that “not anyone will do” as an RF.
Sub-theme 1: Internal virtues
Participants described internal virtues of an ideal RF. These included being “authentic,” “genuine,” “honest,” “patient,” “humble,” “intelligent,” “empathetic,” and “kind-hearted.” Participants felt that these virtues would need to be innate to the RF and could not be “faked” as injured police officers would be able to sense whether their RF possessed these virtues or not. Participants starkly described situations in which these virtues were absent, the relationship between the RF and officer was perceived as less positive, and confidence in the RF’s capacity to demonstrate compassion was diminished.
Sub-theme 2: External virtues
Participants also identified that potential RFs would need to have strong external virtues. In contrast to the needed internal virtues which are necessary for the RF to offer compassionate person-centered care, the focus of external virtues related to an RF’s ability to engage in difficult work and at times do whatever was necessary to protect and support the returning member. Virtues such as “confidence,” “credibility,” “strong,” “courageous,” “intelligent,” “willing to learn,” and “trustworthy” were associated with external virtues. Participants spoke about how these virtues could impact communication, emphatically stating that RFs would need to be comfortable engaging in tough conversations while still being vulnerable; able to engage and build trust (rapport); be approachable, discreet, non-judgmental; able to advocate for the injured officer; and able to engage in conflict management when the needs of the injured member differ from organizational needs or policies. Participants described the RF role as effectively being a “middle man” between the injured member and the organization. As a result, they indicated that it would be important for the RF to be able to effectively engage with both injured officers and PSP organizations.
Sub-theme 3: Not anyone will do
The above two sub-themes strongly informed the final sub-theme that “not anyone will do” as an RF. Participants identified that, in contrast to how positions are normally filled in a paramilitary organization (i.e., seniority or chosen by management), the RF position needs to be filled exclusively on the basis of personal virtues and capacities. For example, participants repeatedly stated that the RF would need to have organizational credibility (e.g., have a strong positive reputation and be respected by peers) to help facilitate buy-in and reduction of fear and stigma. Participants noted the importance of RFs being motivated and driven by a desire to help others and ability to put aside their own ego to advocate for others, regardless of potential discomfort or consequences for themselves. They also noted that an RF needs to be someone who demonstrates self-awareness, positive lifestyle behaviors, and resilience and active listening skills. Participants highlighted that some potential RF candidates may think that supporting injured officers will be easy, not recognizing the cognitive, emotional, and personal load associated with the role.
Theme 2: Holistic/comprehensive workplace reintegration approach
The second theme encompassed a holistic and comprehensive team approach to treatment. This includes recognition of the physical, mental, and spiritual health of individuals.
Sub-theme 1: Holistic/comprehensive workplace reintegration team
Participants described the need for a team-oriented approach to workplace reintegration. In addition to the injured member and RF, a variety of healthcare professionals were identified as being essential to the team, including physicians, occupational therapists, psychiatrists, psychologists, physiotherapists, nutritionists, social workers, peer supports, Workers Compensation Board (WCB) case managers, staff from the Operational Stress Injury Clinic, and colleagues. Participants emphasized that each team member has a specific scope and knowledge that is an asset to workplace reintegration, and that it is important that each team member know their role, communicate with other team members, and “[stay] in their own lane” while working collaboratively. Participants placed great importance on the role of family physicians/medical doctors who have knowledge of injured officers predating the OSI. From the perspective of injured officers, attendees asserted that, “I am not my mental/physical/spiritual health injury - I was someone who existed before.” Participants anticipated that physicians would be in a good position to “see and hear” injured officers from the perspective of prior to and following onset of an OSI. Team oversight was seen as a way to protect injured officers from organizational and WCB demands that may inadvertently impede successful work reintegration.
Sub-theme 2: Comprehensive psychoeducation
The second sub-theme includes the comprehensive and standardized psychoeducational components to treatment that addresses: (1) short and long-term neurological changes; (2) psychological responses and reactions; and (3) physical responses and reactions.
Standardization of the program’s psychoeducational components was reported by participants as being essential to demystifying mental health issues and understanding the short- and long-term effects of the stressful and potentially traumatic events that injured officer’s experience. Improving RFs’ mental health knowledge helped them connect physical health, symptoms, emotions, and thoughts to mental health concerns. This information has the potential to assist participants in understanding the mechanisms that can precede a mental health diagnosis and the interaction of personal, organizational, cultural, spiritual, and internal and external factors that may lead to officer disengagement from the workplace.
Participants were able to identify a number of areas regarding neurological change that they felt important to learn about within the RP. Specifically, individuals thought that psychoeducation should include information on changes in neurological pathways (e.g., basic brain structures, function, and effectiveness). Psychoeducation regarding short-term physiological and physical reactions was also found to be important. Participants appreciated gaining a better understanding of neurological shifts associated with mental health issues, shifting emotions, behavior changes, and discipline issues. Participants reported benefitting from learning about the mind body connection, how trauma can be physically manifested and held in the body, and the short- and long-term effects of prolonged mental health concerns on overall health, including pain, chronic medical conditions, and substance misuse.
Theme 3: Necessary features of the workplace reintegration program
The third identified theme was in relation to the overall qualities of the RP. Participants identified the need for the PRFT to be individually tailored, overseen by mental health professionals, balanced by peer support, and trauma informed.
Sub-theme 1: Customized approach
Participants indicated that an individually tailored RPFT would provide participants with a sense of control and would be uniquely paced and directed based on their individual needs. An outcome of an individually tailored RP would provide PSP with the sense that they matter and that their needs are being heard and responded to. Participants described this process, built on trust, as one of working with individuals on developing a personalized and graduated return to work plan. As a part of this pathway, individuals could discuss their opinions for the most appropriate job placement, wishes for a multifaceted approach, and the integration of graduated exposure therapy.
Sub-theme 2: Necessary oversight from mental health professionals
Participants also discussed the importance of the RPFT being overseen by mental health professionals including psychiatrists and psychologists while encompassing physical, occupational, and trauma therapies. Participants articulated the need for therapy to be long-term to support individuals during their potential ups and downs over time. Additionally, they discussed the importance of the RP in normalizing mental health concerns in trauma-affected populations. Mental health professionals would also assist injured officers in developing self-care strategies to optimize their overall health and well-being.
Sub-theme 3: Balanced by peer support
Participants discussed the importance of peer support in RPs. Peer support, described as an extra yet essential network of support, was associated with empathetic listening, low level mental health support, identification of those who may be at risk to themselves, and facilitating professional help. Participants indicated that peer support can offer injured officers the opportunity to connect with someone with a shared experience and awareness of police culture. Doing so may help them overcome trust issues that they may have with the PSP organization and increase their mental health literacy and health-seeking behaviors.
Sub-theme 4: Trauma-informed care approach to workplace reintegration
Participants indicated that RPs need to utilize trauma-informed care principles. An approach that recognizes the wide prevalence of trauma and acknowledges that trauma affects people in different ways (Alberta Health Services, 2021), principles of trauma-informed care recognize that trauma is complex, specific to the individual, and involves many different experiences (Reeves, 2015). Trauma-informed care fosters physical and emotional safety, providing others with choice and control over decisions that affect them, and providing services that are appropriate to the needs of people affected by trauma (Alberta Health Services, 2021). It also recognizes the potentially cumulative nature of trauma which is a common occurrence in PSP with OSIs. Components of trauma-informed care deemed to be particularly important by the participants included safety, trustworthiness and transparency, peer support, collaboration and mutuality, empowerment and choice, and awareness of cultural and historical issues.
Theme 4: Cultural considerations within PSP organizations
The final theme identified by participants related to the specific cultural and occupational considerations essential for a successful RP program. These included the culture and organizational role in mental health stigma, as well as the barriers and facilitators to successful and sustainable RP implementation within PSP organizations.
Sub-theme 1: Performance culture (stigma)
Participants indicated that one of the primary challenges specific to policing is a culture that is incompatible with mental health help-seeking. This is associated with norms of hegemonic masculinity, authoritarianism, and emotional control. Participants reported that, while significant changes have occurred to address stigma associated with mental health, legitimate and perceived challenges remain. In particular, participants noted that reporting having a mental health challenge can result in a lack of privacy (given the small and insular nature of policing) and that there continues to be career implications associated with admitting to a need for help. A lack of trust in management support, specifically if a person needs a reduced or modified workload, was seen as a significant barrier. Participants acknowledged that this can be exacerbated by the paramilitary structure (i.e., hierarchy) in which there can be tension and conflict between the horizontal and vertical components of the structure.
Sub-theme 2: Barriers to implementation
Participants spoke to systemic organizational barriers which would need to be addressed in order for an RP to be successfully implemented within an organization. Practical challenges to successful implementation include geography (i.e., rural and remote areas), differing divisional geographic needs and experiences, over-tasking, procuring infrastructure for the RP program, and budgetary constraints (i.e., funding for program resourcing or other programs drawing from the same resources). Given current budgetary constraints on police forces, convincing senior leadership and management of the need to develop an RP might be extremely difficult. As such, participants shared that, prior to the commencement of an RP, confirmation of management and member buy-in would be crucial. Equally important would be building a strong business case for the program so as to improve functionality of the organization. This would involve gathering statistics and feedback from participants and establishing an evidence-base. Finally, participants noted that, even if the RP was implemented, there may be ongoing challenges related to finding the right people to act as RFs, as in the first theme, codifying instructor requirements, developing and retaining instructors, ensuring support for the RF, and releasing members to engage in RF positions. Participants also noted that new health and well-being programs are often implemented; however, programs can lose focus and support over time with changing leadership and organizational priorities.
Sub-theme 3: Facilitators to implementation
While participants acknowledged barriers to the implementation of an RP, they also acknowledged that there are a growing number of facilitators that would support the implementation of RPs. For example, participants shared that, despite the continued stigma and career implications of mental health, large public campaigns have been initiated within policing organizations to increase awareness of PSP-specific mental health challenges. Participants noted that there is greater availability of resources for health and wellness programming. Recently, greater access and support has been evident from provincial Occupational and Health and Safety, WCB, and reflected in individual police organization’s health and safety strategic plans and priorities. Participants also noted that, as peer-led RPs expand provincially, nationally, and internationally, there are opportunities for networking, partnerships, and collaboration such that each police organization does not have to solely carry the resource weight of developing and implementing the RP. Sharing training manuals, awareness campaign resources, marketing and promotion material, and lessons-learned with one another can ease the burden of implementation. Finally, participants identified that one of most powerful facilitators would be the endorsement of individual police officers who had gone through and successfully completed the RP. The effectiveness and importance of their testimonials, feedback, and word-of-mouth recommendations and referrals cannot be under-stated nor under-estimated.
Discussion
The purpose of the qualitative component of this mixed-methods pilot study was to: (1) explore the experiences and learnings of PSP attendees of the RPFT course; (2) describe the perceived needs, barriers, facilitators, and recommendations for workplace reintegration and overall workplace culture in their respective police organizations; and (3) vision the potential future of peer-led RPs.
Overall, the attendees of the RPFT program related that the 5 days of training provided them with valuable information that they could use in their respective organizations to fulfill the role of an RF or initiate a conversation around the potential implementation of a peer-led RP. The experience of the PSP was quite positive, and the responses provided through the open-ended questions and World Cafe demonstrated engagement, enthusiasm, empathy, insight, and knowledge into current issues facing PSP. Active steps that can be integrated into personal, cultural, and organizational landscapes to improve overall mental health and facilitate workplace reintegration were also identified. PSP from policing organizations found the short- and long-term EPS RP relevant to their specific workplaces due to the specificity to firearms, while other PSP felt that the long-term RP would be the most useful in their respective professions. Participants found value in both the psychoeducational (e.g., mental health conditions, body–brain connection, and support strategies) and experiential (e.g., specific drills and workplace exposures) components of the training. They were also able to consider needs, barriers and facilitators, and recommendations specific to workplace reintegration in their respective PSP organizations. While these were unique to each organization and profession, similarities were evident across PSP groups, professions, and organizations.
Needs and barriers associated with RPs were identified by the participants. Mental health stigma and resource limitations were prominent barriers, regardless of PSP profession or the stage of RP implementation within a PSP organization. RP needs include buy-in from organizational leaders and resource allocation (e.g., for highly skilled RFs, infrastructure, and time) to initiate, sustain, or spread RPs. For PSP organizations with vast geographic reach (e.g., RCMP, Canadian Border Services, and Alberta Health Services), distance from the RP and access to RFs was identified as a barrier. These organizations would potentially require additional resources to effectively operationalize an RP that could be accessed by PSP in a timely manner. Participants also emphasized that stigma and stereotypes are significant barriers as they perpetuate workplace cultures that are not conducive to recovery and reintegration after an illness or injury.
Reported RP facilitators included media campaigns have improved mental health knowledge, and organizational awareness and priorities aimed at PSP have heightened awareness of OSIs, changed workplace culture, and reduced mental health stigma in the workplace. As PSP RPs become increasingly common, the ability to share resources, anecdotes, and successes was seen as facilitative for implementing, sustaining, and spreading RPs. Participants also noted that the EPS RPFT course is a facilitator and suggested that, with continued uptake of the program, the future of workplace reintegration following an illness or injury is bright.
Recommendations
A number of recommendations from the thematic analysis may be more widely generalized to other PSP organizations who may be implementing peer-led RPs. These recommendations include facilitating strong RPs, clear communication policies and procedures, individualized approaches to peer support, implementation of research initiatives, standardized training and education, utilization of implementation science, and engagement at all levels of PSP organizations.
Integration of effective peer-support initiatives requires the involvement of credible, appropriately trained personnel. The importance of having RFs who are authentic, have strong leadership qualities and abilities, and are recognized and respected within their organizations cannot be understated. They also need to have adequate knowledge and skills and the ability to establish and maintain and build trust and rapport with peers and the multidisciplinary team. Peer-support initiatives are more likely to succeed if stable, desirable, and rewarding RF positions are created that allow peer-support leaders to engage in workplace reintegration as part of their work and not as a voluntary activity that is in addition to their regular duties.
Standardized RPFT training that can be measured and compared for efficacy and effectiveness would be beneficial. The RPFT ideally incorporates both experiential learning and comprehensive mental health education and includes trauma-informed care principles, basic neuroanatomy and physiology, the role and scope of the RF and other members of the multidisciplinary team, and other information related to facilitating mental health and wellness. Standardization of the RPFT would facilitate increased program fidelity, allow for the sharing of validated RP resources, and facilitate streamlining of RP implementation across organizations. Although standardization would be of benefit in some respects, it is also important that newly trained RFs have the flexibility to tailor the RP to the individual needs of PSPs with OSIs within the context of their profession and organizational culture and demands. It would be beneficial for RPFT training to foster divergent thinking and flexibility while also clearly defining RFs’ scope and role. It is also critical that the RP is member-centered, safe, and, with the support and guidance of the multidisciplinary reintegration team, facilitates the rehabilitation and reintegration process.
Communication policies and practices among reintegration team members that respect the confidentiality and privacy requirements of each profession and the RP participant must be established and adhered to. The reintegration team includes, but is not limited to, the multidisciplinary medical team, WBC, peer-support program, and the participant. Ongoing communication between the mental health providers and the RF is especially critical to the success of the RP experience. Ensuring that personal information is not divulged to others within the employing organization is paramount to assuring trust among those in the RP program and avoiding potentially adverse impacts that disclosure of information could have on the person’s reintegration plans.
Engagement at all organizational levels, in cooperation with external stakeholders, is recommended in order to develop and maintain evidence-based best practices for workplace reintegration. Buy-in must be facilitated, communicated, and modeled from the top down to influence sustainable cultural change throughout the ranks of the organization. PSP organizations would likely benefit from allocating resources to initiatives such as the RP. Doing so would assist with reintegrating ill and injured personnel into the workplace, improving workplace culture and attitudes around OSIs, and decreasing mental health stigma. External stakeholders, such as government organizations, may be able to assist with implementation practices and research initiatives, as well as knowledge mobilization and translation.
Future research on PSP workplace reintegration programs
More research is needed to evaluate the effectiveness, efficacy, and safety of peer-led workplace RPs and facilitator training programs. As emphasized in the Blue Paper, research conducted by external stakeholders could lead to the evidence-based validation of programs such as the peer-led EPSRP and RPFT program for PSP (Beshai and Carleton, 2016). Study of organizational and cultural impact, cost benefit, implementation drivers and processes, and knowledge mobilization strategies is also warranted. As this research expands, other populations at elevated risk of OSIs, such as military, veteran, and healthcare professionals, could also be included to examine the overall impact of peer-supported workplace reintegration initiatives. Future research could also explore the experiences of OSI-affected family members and family-specific needs. Favorable research findings would potentially pave the way for more widespread program adoption and integration. Use of effective implementation science approaches would best facilitate sustainable spread and scale, enabling more PSP with OSIs to be supported in recovery and return to work. Development and evaluation of population-specific workplace RP tools and resources (e.g., a repository of videos, apps, online resources, and training material), as well as prevention and intervention strategies, would be invaluable.
Limitations
There were a number of limitations in this study. The data collected in this study were from a single RPFT course specific to a workplace RP created by the EPS in Alberta, Canada. The specificity of the program and sample limits the generalizability of the findings; however, since this program is now seeing international spread, it is important to research it through an evidence-based approach.
Due to the time, infrastructure, and human resource constraints during the RPFT, the World Cafe was one of the selected methods of qualitative data collection. Although engaging, the World Cafe does not allow for anonymity of the participants. This adds bias to the data as participants may not have been as open with their responses with their peers present. The hierarchical nature of PSP organizations means that rank and roles may also affect the participant’s ability to discuss these topics openly. The stigma surrounding issues regarding mental health, reintegration, PSP culture (norms of hegemonic masculinity, authoritarianism, and emotional control), and organizational culture and policies may also hinder PSP’s confidence in sharing ideas and their voices.
Conclusion
Study participants shared a common vision of support for injured PSP, desire to develop peer-supported work RPs, and hope for reduced mental health challenges in PSP organizations. Member-centred, culturally specific, precision-tailored programming was seen as central to the success of RPs and recovery of PSP with OSIs. Participants highlighted the value of having trained peer supporters available to PSP to assist them in their return-to-work efforts. It was evident to participants that RFs would need specific personality traits, skills, and knowledge and intentional collaboration with a multidisciplinary team to effectively support those with OSIs. The RPFT program reportedly equipped them to provide necessary support. While RPs hold much promise, and interest in peer support in PSP organizations is growing, it is essential that a strong standardized evidence-base be used to guide both RF training and RP uptake. Supporting members using the best evidence and practices, supports those who have been injured amidst their efforts and commitment to serving their communities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.