
Abstract
In Australia, voluntary assisted dying (VAD) is now widely legalised, and VAD uptake is on the rise. Thus, the demand for psychological support in the context of VAD is expected to grow. Despite their relevant expertise, psychologists remain underrepresented in end-of-life (EOL) literature and practice. The current in-depth qualitative study examined the perspectives of 20 provisionally registered psychologists in Australia on VAD, using reflexive thematic analysis grounded in social constructionism. Four main themes (‘Values’, ‘Fit-for-Role’, ‘Exposure’, and ‘Contributions’) and 14 sub-themes were generated from the data. Participants supported availing VAD for terminally ill patients and expressed the potential for its use with dementia sufferers. Nevertheless, participants expressed little interest to engage in VAD care. Participants shared concerns about the high-stakes nature of VAD, the emotional strain of EOL practice, and limited exposure to EOL and VAD. Practical implications and directions for further research are discussed.
Keywords
Introduction
Technological advancements, epidemiological developments, medical interventions and evolving attitudes toward end-of-life (EOL) care have changed conceptualisations of death from uncontrollable to the prolongation of life or to voluntary assisted death for people with incurable chronic illnesses (Carr & Luth, 2019). Voluntary assisted dying (VAD) is a legal process allowing terminally ill patients to choose the timing and manner of their death through the administration of a prescribed lethal substance (White et al., 2023). In 2019, Victoria became the first Australian state to implement VAD, followed shortly by Western Australia (2021), Tasmania (2022), South Australia (2023), Queensland (2023), New South Wales (2023) and to be implemented in November 2025 by the Australian Capital Territory (Go Gentle Australia, 2024). The Northern Territory (NT) was the first jurisdiction in Australia to legalise VAD through the Rights of the Terminally III Act 1995; however, this was overturned by federal legislation in 1997. Following the lifting of federal restrictions in December 2022, NT is now considering new legislation to reinstate VAD (VAD Independent Expert Advisory Panel, 2024).
As of 1st March 2023, the average age of VAD applicants across Australian jurisdictions was 73, with nearly 80% having accessed palliative care. VAD deaths make up 1% of all deaths, which is expected to rise (Go Gentle Australia, 2024). The legalisation of VAD brought to the fore diverse cultural and moral perspectives on death, complicating EOL care - particularly in the palliative sector - where patient care overlaps with VAD eligibility (Gire, 2014). Acknowledging diversity of moral positioning, healthcare professionals can exercise conscientious objection (CO) against VAD, which exacerbate existing workforce shortages. This underscores the need for increased investment in the EOL workforce to meet a growing demand for VAD, ensuring safe, high-standard services and effective implementation (Gridley, 2018; Go Gentle Australia, 2024; Palliative Care Australia (PCA), 2022).
With a growing demand for qualified health professionals in the context of VAD, it is timely and relevant to explore the involvement and support provided by mental health professionals in this domain. Despite possessing the skills to support people suffering psychological distress in EOL care, psychologists are underrepresented in this sector. Brook et al. (2023) found that 75% of palliative care services lacked access to a psychologist, and only 1% of psychologists self-reported expertise in palliative care (Gridley, 2018). This limited involvement is partly due to EOL not being considered a priority, and receiving less attention in the education and training of psychologists compared to disciplines such as medicine and nursing (Breen & Ugalde, 2017; Vivekananda et al., 2020).
As VAD is sanctioned in tandem with an aging population, increased life expectancy, and prevalence of chronic illnesses, opportunities for psychologists’ support for dying patients, their families, and other affected stakeholders are projected to rise (Foo et al., 2024; Haley et al., 2003; Morante et al., 2020). Considering this trajectory, the current study investigated the perspectives of provisionally registered psychologists (PRPs) on VAD to understand their motivations and barriers to professional involvement in the area. PRPs are primarily postgraduate students (with the crossover exception of those who completed the now discontinued 4+2 internship pathway) who are upcoming psychologists and are uniquely positioned to provide insights on both curriculum and future career trajectories. The findings of the current study enhance the knowledge base on VAD, advance understanding of the psychologist’s role in VAD care, and inform future VAD policy reforms, curriculum, and research.
Currently, there are no statutory VAD directives for psychologists. VAD guidelines, however, recommend that coordinating and/or consulting medical doctors or specialists refer VAD applicants to psychologists or psychiatrists for mental capacity assessments or undue influence screening if eligibility concerns arise (Peisah et al., 2019). Legal aspects relevant to psychologists include CO (allowing them to decline involvement in VAD), the “gag clause” (inhibiting VAD conversations with clients in certain states, e.g., Western Australia), and a Federal telehealth ban on recommendation of VAD (Waller et al., 2023; WA VAD Board, 2019).
Psychologists possess a unique set of skills and aptitudes rendering them well-suited to contribute to EOL care, including VAD. Their ability to assess cognitive capacities of VAD applicants and provide mental health support for affected stakeholders have been recognised as key aspects of their role (Breen & Ugalde, 2017; Brook et al., 2023). Furthermore, psychologists are capable of developing psychoeducation for the wider community and group-based interventions addressing critical VAD-related issues such as death and dying as well as grief and loss (Foo et al., 2024; Ftanou et al., 2017).
Despite their valuable skill set, several barriers limit the participation of psychologists in VAD support. One significant barrier is ambivalence, whereby VAD is perceived as an area of lesser importance and one that fails to generate interest within the profession (Gridley, 2018; Vivekanada et al., 2020). Additionally, practical challenges such as insufficient training, lack of funding and inadequate remuneration further hinder psychologists’ involvement with VAD (Gridley, 2018; Leonard et al., 2017). These obstacles affect the engagement of psychologists and reflect broader systemic issues within the healthcare system regarding the support and integration of psychological services in VAD-related care.
Overcoming these barriers requires a proactive shift in the training of psychologists to incorporate VAD-related care as a central component of their practice. This includes cultivating greater interest and involvement in VAD policy, practice, education, training, and research (Brook et al., 2023; Trang, 1998). Advocacy is crucial to elevating the role of psychologists in VAD-related care and ensuring they are adequately equipped to meet the growing demand for VAD services. A shift from conventional symptom reduction and behaviour modification to placing importance on quality therapeutic relationships is also recommended for psychologists’ involvement with VAD (Block, 2006; Forbat, 2018; Gridley, 2018).
Existing studies underscore the conceivable contributions and challenges faced by psychologists in VAD-related care. To date, no research specifically examined the views of PRPs’ on VAD, leaving a gap in understanding their perspectives and potential involvement. Recent findings indicate that the sustainability of VAD is threatened by access obstacles including limited numbers of senior VAD-endorsed doctors/specialists positioned as gatekeepers to authorise VAD applications (Rutherford et al., 2023). The involvement of psychologists in such processes and procedures could assist in meeting such challenges. Psychologists are well-equipped to support VAD mental health needs through psychotherapy, capacity assessments, and developing best practices at individual, community, institutional, and government levels, including psychoeducation, policy reform, and advocacy (Gridley, 2018). The current qualitative study gives voice to PRPs, addressing the lack of representation of psychologists in VAD discourse. The research question posed by the current study was: what are the perspectives of provisionally registered psychologists (PRPs) in Australia on voluntary assisted dying (VAD)?
Method
Approach
The epistemology of social constructionism was employed by the current study to explore the subjective views of PRPs on VAD. Data were collected via in-depth semi-structured one-on-one interviews. Reflexive thematic analysis (RTA), a qualitative method grounded in social constructionism, was used for data analysis, which uncovered the meaning of VAD for PRPs based on their personal and professional contexts. This analysis offered in-depth and nuanced insights into PRPs’ engagement with the complex topic of VAD.
Selection and Description of Participants
Overview of PRPs’ Profiles.
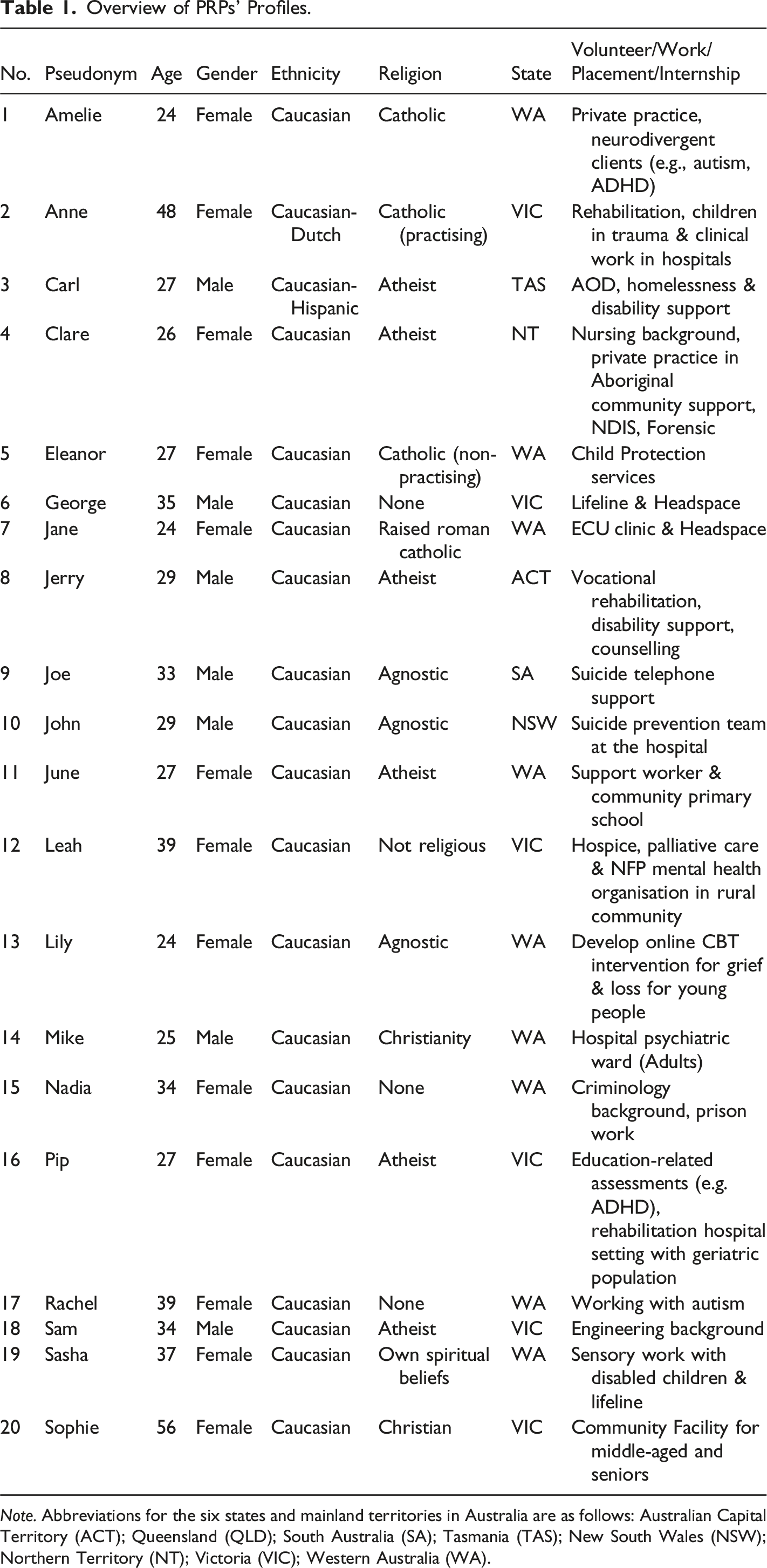
Note. Abbreviations for the six states and mainland territories in Australia are as follows: Australian Capital Territory (ACT); Queensland (QLD); South Australia (SA); Tasmania (TAS); New South Wales (NSW); Northern Territory (NT); Victoria (VIC); Western Australia (WA).
Reflexivity
Aligned with a social constructionist paradigm, this study foregrounded the researcher’s dual identity as both a trainee psychologist and a qualitative inquiry partner. My career trajectory in psychology and focused interest in EOL care and VAD shaped the research questions and data interpretation, as my own experiences provided context for participants’ accounts (Olmos-Vega et al., 2023). Recognising that knowledge is co-constructed in interactions, I consistently reflected on how my professional background influenced interview dynamics, question phrasing, and iterative coding decisions. Sharing the trainee psychologist role with participants fostered mutual trust and enabled deeper dialogue, while regular discussions with the second author and reflective journalling helped bring to light and challenge assumptions. These reflexive practices ensured that participants’ nuanced perspectives on VAD were authentically represented and contextualised within the shared professional milieu.
Data Collection and Procedures
One-on-one online interviews were conducted in English via Microsoft Teams using a semi-structured interview schedule, which comprised six open-ended questions with related probes informed by two similar studies that investigated VAD perspectives of older adults (Gringart et al., 2022) and nurses (Penman et al., 2022). The schedule included questions about participants’ knowledge of VAD, their related perspectives as well as potential professional involvement, and their insights on education and training relevant to VAD practice.
Following ethics approval by the university’s Human Research Ethics Committee (HREC), participants were recruited through emails sent by psychology Master program coordinators to postgraduate students, posting of research recruitment electronic flyers on relevant Facebook communities with a PRP membership base, and a snowballing strategy where recruited participants shared the e-flyer with eligible peers. Potential participants contacted the researcher directly to express their interest. Recruitment and interviews were conducted between 7th May to 10th July 2024. Written and verbal consent were received before interviewing participants. Participants were informed that they could withdraw at any time from the study without any penalty and could decline to answer any questions during the interview.
All interviews were audio recorded for verbatim transcription and data analysis. Each interview commenced with a casual conversation and rapport building, followed by questions about what the participants knew about VAD, their views on it, how VAD might impact their professional practice, and their thoughts about the current education or training for VAD practice. Participants were invited to share additional thoughts related to VAD and were thanked for their time and contribution. The duration of interview per participant was between 1 and 1.5 hours.
Data Analysis
The RTA process was informed by Braun and Clarke (2022). RTA is a recursive process that involves themes being revised, removed, recoded or collapsed for the most meaningful data interpretation to establish the four main themes to address the research question.
Each interview was transcribed verbatim for accuracy and to facilitate engagement as well as familiarisation with the data. To enhance rigor, member checking was conducted with participants to ensure the authenticity of interview transcripts, confirming that the transcribed conversations accurately reflected their intended meanings. Cross-analysis agreement was established in collaboration with a peer who independently analysed two deidentified transcripts. An audit trial and a reflexive journal were kept, which assisted data analysis and minimising potential researchers’ bias.
Results
Four major themes and 14 sub-themes were constructed from the interview data with 20 PRP participants. Figure 1 presents a schematic view of the findings and the conceptual relationship between themes. Each theme and its related subthemes are discussed along with illustrative participants’ quotes and relevant existing sources. Participants’ names were replaced by pseudonyms to maintain confidentiality. Thematic Map: Four Main Themes and 14 Sub-Themes and Their Conceptual Relationship. Note: The positive “+” sign indicates a theme’s positive impact on role contributions and the negative “-“ sign denotes a negative impact.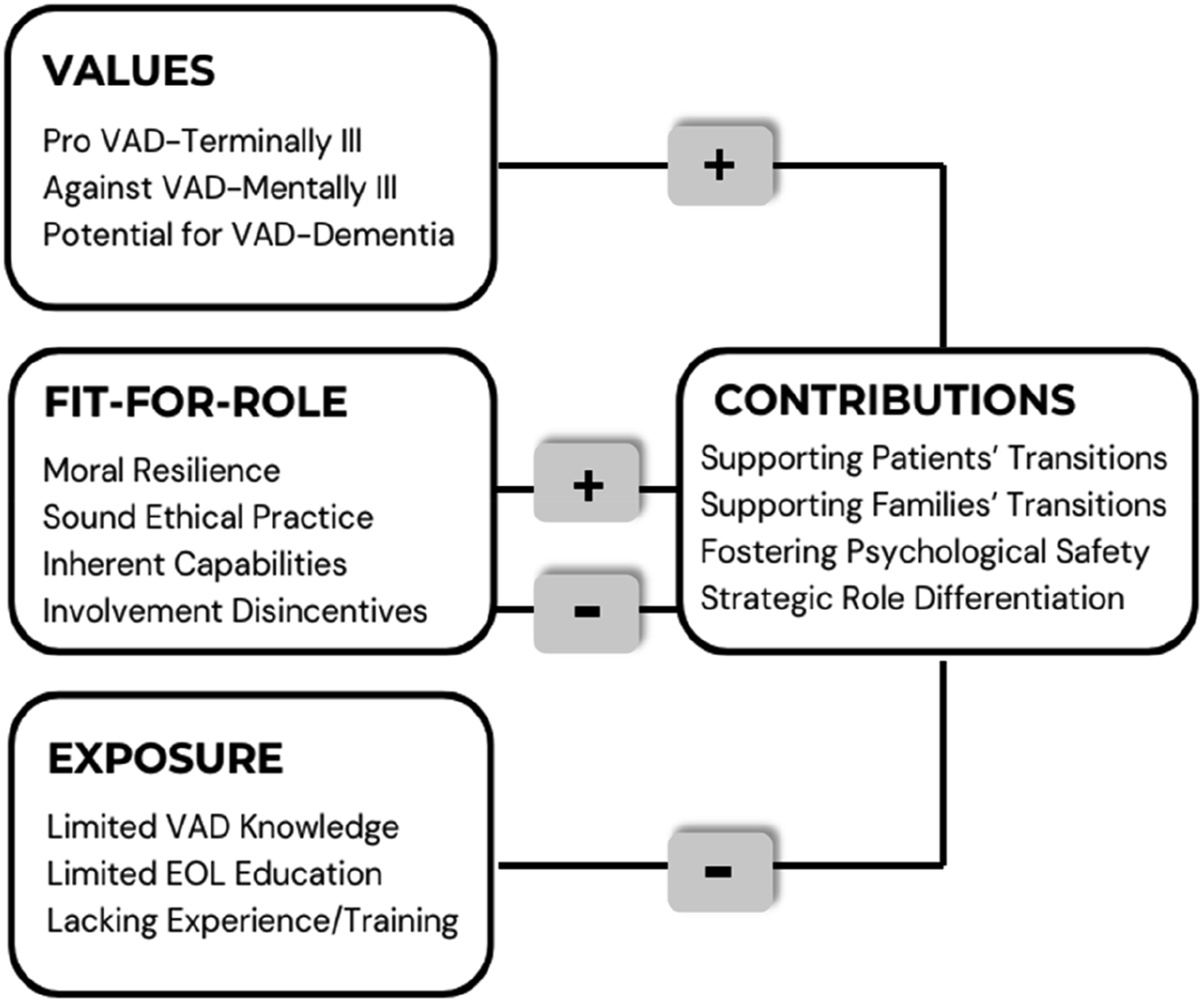
Values
Values guide actions, decision-making, attitudes, and behaviours (Oyserman, 2002; Schwartz et al., 2012). VAD is a construct tied to moral judgments and personal preferences (Thome, 2015), which is examined here through participants’ perspectives on various VAD models shaped by their value-driven stances (Kuczynshi, 2001).
Pro VAD-Terminally Ill
Participants supported VAD for the terminally ill, with their values aligning with key principles of the VAD Act: “valuing life, dignity, autonomy, quality care, accessibility, informed decisions, protecting the vulnerable, and respecting diversity” (State of Queensland Queensland Health, 2022 pp. 8–9). These values are congruent with the Australian Psychological Society’s (APS) Code of Ethics (2007), which outlines “respect for rights and dignity, propriety, and integrity” (p.6). Sophie said, “I feel they should have a say in how they want to go, to keep their dignity”, a view shared by Sasha, “client autonomy is really central to my psychological practice.” Though personal and professional views on VAD were convergent, participants compartmentalised their personal beliefs to respect others with differing opinions on VAD. Leah said, “personally, l am open and favourable towards VAD. I have to be careful and very conscious to make sure I portray any conversations as objective and neutral...because I know that it won’t necessarily be everybody’s experience.”
Furthermore, “being legally and medically sanctioned by law (George)” reinforced pro-stance for VAD because it is death “in a controlled safe way (Leah)”. For Jerry, “terminal cancer, that’s perfectly appropriate, that’s a routine presentation and that’s something the State can eventually get good at dealing with and it’s the quintessential case for VAD.” Jerry’s sentiments model the current VAD-terminally ill framework in Australia where terminal cancer is VAD’s primary diagnosis (72.6%) (Go Gentle Australia, 2024). An interesting pro-stance view emerged from Lily, “if VAD isn’t an option, it just creates more issues against people trying to take their life by other means, which is at risk of not being successful or just being overly distressing to the family.”
Participants highlighted religion as contentious for VAD, reflecting one of the key arguments - religious objection - used by those against VAD legislation (Kresin et al., 2021). Participants who specified a religion in their profile form (see Table 1 in Method section) conveyed being born into the family’s religion, but most were non-practising. They exhibited adaption in their understanding of religious teachings as Jane (Catholic) articulated, “beliefs of the church are quite outdated. When we have medical advancements that give people agency, why not use them when they’re in that much distress.” This finding corresponded with research showing that people’s values shift in a way to accommodate new life situations facilitating better adjustment to life transitions (Bardi et al., 2014).
Against VAD-Mentally Ill
In Australia, VAD is only available to terminally ill patients, yet participants discussed eligibility of VAD for mental illness, legalised in some countries such as Switzerland, Belgium, The Netherlands and Luxembourg (Peereboom, 2023). While participants supported VAD for the terminally ill, they were apprehensive about extending VAD access to those with mental disorders. Participants’ concerns mirrored opponents of the VAD-mentally ill model. Grounded in the principle of beneficence, which obligates healthcare professionals to act in patients’ best interests, participants alluded to the vulnerability of individuals with mental illness, who may lack the capacity for sound decision-making (Dembo et al., 2018). This vulnerability was a key concern for participants, especially given the irrevocable nature of VAD. They also cautioned that some mentally ill individuals may express a desire for death as a plea for help, rather than a genuine wish to die as purported by Pridmore et al. (2021). John contended, People don’t necessarily want to die, but they want the suffering to end…coerced by their own short-term suffering but the ending of life is permanent. For mental disorders, their ability to make rational decisions might be compromised with care-eliciting suicidal behaviour.
The blurred distinction between suicide and VAD is a significant concern in the VAD-mentally ill model given the causes of suicidal thoughts and behaviours are not fully understood. These behaviours result from complex interactions of various factors, driven by different motivations (O’Connor & Nock, 2014). Joe commented, “…how do you differentiate between a person’s VAD attempt as a means to escalate care.”
Although participants acknowledged that mental illness could bring intolerable suffering, they counteracted that mental conditions are not definitive death diagnoses and may be effectively managed or treatable as supported by Peereboom (2023). June questioned, “it’s a slippery slope…where do you draw the line for mental illness?” while Sasha stressed, “when there’s a terminal physical illness, there’s a clear line” and Eleanor asserted, “there’s more research and more treatments that are becoming effective for treating mental health disorders.”
Participants associated VAD for the terminally ill mainly with older adults. They voiced concerns that extending VAD to the mentally ill would broaden access to younger people. The idea of VAD for youths evoked stronger objections. Sophie explained, “…everything is cut short, young life with unfulfilled prophecy.” This sentiment aligns with research suggesting that in Western cultures, younger lives are seen as having greater social value, while elderly deaths are viewed as part of the normal life course (Bolt et al., 2019).
Potential for VAD-Dementia
Current VAD eligibility criteria across all Australian jurisdictions implicitly or explicitly exclude individuals with dementia (Dementia Australia, 2023). This was incongruent with participants’ views that dementia patients may be eligible due to the severe and progressive nature of the condition. As supported by lived experience feedback from carers of dementia patients in VAD WA Annual Report (2023), Eleanor reasoned, “like dementia, I would agree because it’s a degenerative disease and it’s not going to improve…that person is dying because of the way it impacts their brain.”
Fit-For-Role
Role fit theory suggests that optimal outcomes occur when personal aspects (e.g., needs, abilities, values) coincide with environmental factors (e.g., work demands, values, resources) (Van Vianen, 2018). The previous theme showed general coherence between participants’ values and the legislated VAD-terminally ill framework. Findings from the fit-for-role theme indicated that participants are well-suited to provide mental health support for VAD-related issues. However, this suitability does not necessarily concur with their intentions to participate in VAD care due to disincentives, which are discussed further in
Moral Resilience
Healthcare professionals may experience moral injury when involved in or witnessing patient care that conflicts with their personal or professional beliefs (Litam & Balkin, 2021). The Australian Medical Association (AMA) policy states that “doctors should not participate in interventions primarily aimed at ending a person’s life” (Khorshid & Miller, 2022, p. 933), while the APS Code of Ethics requires psychologists to “promote equity and protect human, legal, and moral rights” (APS, 2007, p. 11). The understanding of distinct ethos is captured by Carl, “I think that those (patients’) rights should be upheld” versus June’s perspective that “the whole medical ethos is do-no-harm.”
Participants expressed a degree of separation from the VAD decision and its implementation (e.g., prescription, administration, or witnessing death) compared to authorised medical teams because psychologists are not the primary gatekeepers or front-line providers. Mike noted, “I’m not signing the paper saying this person’s going to go through with VAD. I don’t have to do that. The doctors have to do that.” The contrasting ethos between protecting human rights (APS) and avoiding harm (AMA), in conjunction with the differing roles in VAD care - psychologists’ focus on mental well-being care versus medical teams’ direct involvement in life-ending procedures – may be why psychologists experience enhanced moral resilience.
Sound Ethical Practice
Participants were unwavering in upholding ethical standards in their psychology profession. Their education and training in ethics successfully instilled reflective practices verbalised by Sasha, “I’m aware of some of my prejudices around VAD and trained to reflect and check myself on that”. The ability to maintain clear boundaries between personal and professional viewpoints was articulated by Sam, “different psychologists will have different personal opinions on VAD, but I think that needs to be kept separate in your professional work.”
Participants were attuned to ‘General Principal B.1. Competence, B.2. Record Keeping and B.3. Professional Responsibility’ (APS Code of Ethics, 2007, pp. 18–20). They seemed committed to doing right by clients with informed consent as Nadia stated, “I would feel less comfortable with VAD if someone can’t adequately understand what it means for them to consent”; by taking professional accountability for their competency, as Sam explained, “if I wasn’t competent or capable of being impartial enough to work with that client, then the only ethical thing to do would be to refer them on”; by their willingness to seek appropriate training and referrals, as conveyed by Pip,” my main thing would be making sure I’ve got the appropriate kind of training and supervision to be able to support that person throughout the process”; and by maintaining reporting responsibility as mentioned by Amelia, “there is an ethical responsibility to have VAD noted in the clinical notes on file for legal purposes.”
Inherent Capabilities
The entry requirements for postgraduate psychology programs accredited by APAC are rigorous and highly competitive. These programs demand candidates meet high standards of eligibility, which include demonstrating inherent aptitudes and skills, academic excellence, research competency, and relevant work or volunteer experiences. The stringent vetting process ensures that selected participants for psychology Master programs, or in internships, possess baseline qualifications essential for providing psychological support for VAD-related issues.
Involvement Disincentives
Whilst there appear to be values and role fit, participants seemed reluctant to engage VAD-related work. Participants’ perceptions of “extra stress or workload when working in (VAD) practice (Lily)”, and unfair remuneration by the government seemed to act as barriers. As Jerry described, “there is such a shortage of psychologists, you are not going to find many people to do VAD work as the government doesn’t pay enough for what sounds like a pretty depressing job”. This sentiment is echoed by the medical profession highlighting poor compensation for their time and services in supporting patients through a highly involved and lengthy VAD process (Haining et al., 2023; VAD WA, 2023).
High ethical standards upheld by participants amplified their concerns regarding legal ramifications of “fear of litigation (Clare)” or “malpractice (Mike)” due to perceived ethical complexity in VAD-related practice involving an irremediable outcome and added responsibilities. Rachel contemplated, “from an ethical perspective when we’re treating multiple people from the same family…It means that we then have obligations to those family members.”
Other barriers to VAD participation were “being uncomfortable working with death and (VAD is) not an attractive subject (Leah)”, reinforced by Sasha, “in the Australian culture, we’re not good at death, it’s uncomfortable for people.”
Exposure
VAD access is primarily associated with the older population and functions alongside palliative care services (Go Gentle Australia, 2024). The limited exposure of participants to the EOL sector, including VAD, can be partly attributed to the historically low involvement of psychologists in aged and palliative care. In 2004, APS’s brief on the role of psychologists in aged care services indicated a limited presence of psychologists (APS, 2004). Decades later, in 2023, APS issued a similar position substantiating the findings of the Royal Commission into Aged Care Quality and Safety in 2021, which continually highlighted the unmet psychological needs in aged care (APS, 2023). Despite evidence promoting seniors as a vulnerable population who can benefit from psychological support, less than half of the services were provided by psychologists. Similarly, Brook et al. (2023) drew attention to the scarcity of psychological services in Australian palliative care, urgently calling for psychologists to support patients at EOL and their families.
Limited VAD Knowledge
VAD knowledge was minimal among the participants, with some unaware of its legalisation. Rachel stated, “I do have to warn you, I don’t know a huge amount about the topic”, similarly Jane, “it never got brought up in any course that I was in”, while Sam shared, “I actually didn’t think VAD was legal in Australia yet.”
Participants attributed their lack of VAD exposure to not working with seniors or within aged or palliative care, as Elanor expressed, “no (exposure) because I work with child and adolescent population”, whilst others lamented on why they were not provided VAD information given they are part of allied health. Carl queried, “as a health professional who may be involved in the VAD process, I have not received any information or training in how I support people through that process.”
There was some exposure to VAD. June discovered that a friend’s mother had recently passed by VAD, while Amelia, who was interning at a private practice, encountered two clients who experienced VAD deaths of elderly parents. Upon probing, some participants recalled similar encounters that could be contextually related to VAD, even though the term itself may not have been explicitly mentioned. There is an anecdotal sense that the prevalence of VAD exposure was underestimated because it is not talked about and not typically at the forefront of awareness. Sophie said, “it has been talked about, but it hasn’t.” VAD consciousness seems to be gradually permeating society even though people might not realise it. Rachel recalled her personal encounter, “my dad made it clear if he had an illness that offered him a really significant deterioration of life, he would want to end things there.” George recollected his encounter from crisis support work, “I was kind of confronted with VAD...It was a help seeker, she had decided if things (illness) hadn’t turned around, she was going to end her life by that sort of date.”
Some participants mentioned brief exposure to VAD through a case study during their university education. Participants expressed concerns about the lack of knowledge on VAD legislation for psychology students, particularly regarding ethical issues like the Federal telehealth ban (i.e., only one participant was aware) and the “gag clause” (i.e., none were aware of it). They stressed the need to incorporate VAD legalities in ethical and conduct guidelines for psychologists and suggested more professional development (PD) seminars on VAD, as Lily proposed, “there needs to be education about that kind of legal and ethical considerations and implications of working with VAD patients.” Awareness of VAD is critical because interested PRPs can seek out further PD initiatives. Rachel exclaimed, “…a strange gap to have because even if we are going to be involved (in VAD), like there’s nowhere around that!”
Participants highlighted the importance of community awareness and open public discussions to improve VAD access, service delivery, and processes while informing future reforms. Mike gathered, “being spoken at a public level is necessary…it’s legal so it wouldn’t be a discussion for or against, but for society to discuss future requirements of VAD.” There were also concerns raised about the lack of guidance from governing bodies regarding the practical implementation of VAD for psychologists. Rachel commented, “from my reading, there’s not much emphasis being placed on the psychologist’s role at the moment” and Lily said, “I would want there to be a pretty clear framework for us to follow.”
Medical practitioners must complete VAD training before being endorsed to practice and participants favoured the same endorsement for psychologists. Clare proclaimed, “…endorsement in VAD is almost essential. Like dying is the biggest thing that you go through” and advocated by Jane, “it’s an area that holds so much risk…specialised training and support made available for me to feel safe working in VAD.” Participants’ sentiments were reflected by Breen and Radermacher (2019), “currently, there is no ethical guideline to assist psychologists who work within a context where VAD is legal. Development of such a guideline would be valuable” (InPsych, August, Issue 4).
Limited EOL Education
VAD and palliative care are considered two EOL options for dying patients. Even though EOL is a topic highly relevant to all due to the certainty of death, “people don’t like talking about death (Leah)”. Participants saw death as a topic that people tend to avoid, often associated with discomfort or stigma. Sasha surmised, “we will all experience (death)…it’s ironic that there isn’t more conversation, but it’s uncomfortable for people.”
Butow (2017) highlighted the importance of focusing on death and dying in psychology as existential discussions can enhance EOL well-being. However, participants observed that tertiary psychology education primarily focuses on suicide. Some participants mentioned brief exposure to topics like seniors, grief, and loss within a lifespan development course. John shook his head saying, “very little…the philosophy of psychology behind death is missing these days”, and Anne elaborated, “there is a space for existential education...marrying two worlds of life and death.” Participants demonstrated a basic understanding of the differences between VAD, suicide, and palliative care. However, palliative care was not mentioned in any of their psychology education.
Participants shared that postgraduate psychology courses are intensive with limited capacity for additional content and that VAD is a relatively niche topic. Nadia remarked, “whether be it at the undergrad level or the master’s level, there is just so much information to condense into a program.” However, participants agreed that important EOL topics such as aged care, palliative care, death/dying and grief/loss should be included. Anne observed an education gap in the EOL domain, “in a private clinical setting, you get grief and bereavement a lot but do not get exposure from university education.”
Lacking Experience/Training
Most participants reported no experience working with the elderly, as reflected in published participation statistics. Only 14% of residential aged care facilities directly employ psychologists (APS, 2023), and Brook et al. (2023) found that 75% of palliative care services lack access to a psychologist. Three of the twenty participants had meaningful work or volunteer experience with the aging population, driven by their personal interest in geriatric care. Leah who worked as a volunteer in aged care said, “for a long time I’ve been interested in working with older age demographics, so it is very relevant to my practice.”
Participants suggested that more opportunities to work in the aged and/or EOL sector could increase their willingness to get involved in VAD. Pip highlighted, “I don’t really see it impacting my work that much, but then again maybe it’s because we haven’t had the training or opportunity to kind of recognise where it could impact our work”, and strengthened by Sophie’s feedback, “Look, awareness is the biggest thing. I think for me just that exposure, so with placements for example.”
Participants conveyed that their current placements or internships significantly influence their future career trajectory, often helping them find their “sweet spot” and guiding their career path, as evidenced by Mike, “I got my last placement at a hospital, and now that I’m graduating soon, I’ve asked to stay on because I quite enjoy my placement work and now I’m working at that hospital” and shared by Amelia, “from my internship, I found I gel quite well with females ADHD from 15 to 30. That’s the kind of client group that I’m enjoying working with.”
Contributions
This theme captures participants’ perspectives on the roles of psychologists in addressing the psychological needs of key stakeholders throughout the VAD process—before, during, and after VAD. Existing literature alluded to the potentially valuable role contributions of psychologists in the VAD domain (APS, 2024) and are congruent with the views of participants who are provisionally registered, which are discussed subsequently. The concept of transitions is relevant for data interpretation as contemporary dying role disrupts the traditional living and dying norms (Lowrie et al., 2019).
Supporting Patients’ Transitions
The stress framework is used to understand the impact of life transitions (Haslam et al., 2021). The transition from dying to death can be highly stressful, often leading to adjustment challenges, with disorders like depression, anxiety, and suicidal ideation being prevalent (APA, 2022). Ensuring that a VAD applicant has the capacity to make a sound decision is crucial, and participants believed psychologists should be involved in assessing VAD decision-making capacity. Pip shared, “in our work, there is a lot of assessments as part of what we do to get a formulation of a client.”
Life transitions prompt us to re-evaluate who we are and who we will become, reshaping our personal and social identity (Haslam et al., 2021). Terminally ill patients often inhabit a “living but dying state (Sasha)”, adopting a “living-dead” identity. VAD offers a transitional opportunity for these patients to redefine their identity, ending suffering and embracing autonomy, providing a source of strength and immense relief (McNamara, 2004). Joe imparted, We are giving people support like adopting that identity of transition towards someone who is terminally ill but in a new phase of life. If that is a more positive identity and it's supported and it's safe and you know that if you do need to die, there’s going to be a quick painless way of doing it that’s under your control, it’s less uncertain and it’s less scary, which would probably mean that they would be more willing to adopt the truth that they are terminally ill rather than denying it.
Given the vested involvement in the VAD application process, participants identified the need for psychological support for applicants (and their families) who are rejected from accessing VAD. According to the VAD QLD Annual Report (2023), about 5% of applicants were deemed ineligible in the first assessment, with an additional 1% rejected during the second consulting assessment. Nadia stated, “I think it could elicit a lot of distress. And possibly also suicidal ideation. As well, a chance people start thinking about assisted suicide.”
Social support plays a crucial role as a psychological buffer in mitigating stress caused by adverse life changes (Haslam et al., 2021). Participants emphasised the importance of family members offering practical and emotional support in facilitating VAD, considering the frailty of chronically ill patients. Mike proposed, “not just the individual, bringing the inner circle I think is essential. The family should be brought into the process as soon as VAD is seriously discussed” and Sophie, “people with larger families sort of tend to stick together….collectivist cultures somewhat easier because they are better supported, people with smaller families are not as cohesive.”
Participants maintained that psychological support is paramount for the mental well-being of patients and their families, particularly when faced with stressors like family objections, community disapproval (e.g., religious groups), or complex adjustment disorders. Sophie further explained, The main stakeholder will be the client requesting VAD and then closely second is the family because sometimes the family may not agree with VAD. Psychologists can just be there. Hold the space, listen, try and support reasoning. Include family in conversation.
Participants discussed practical challenges of accessing psychological services, as described by Leah, “my concern with support in the VAD space is knowing how much time and energy all these doctor’s appointments, care and daily tasks take. Seeking psychological support seems to be something that gets kind of left till last.”
Terminally ill patients are navigating and processing their own grief. While there is criticism of the Kubler-Ross model, the sixth stage of finding meaning (Kessler, 2019) is highly relevant for VAD grief. Participants thought existential and acceptance interventions may help VAD users find meaning and come to terms with the act of death. Citing Nadia, “all these really big existential questions that I could imagine would come up as they go through those stages of grief” and Mike suggested, “therapies that explore existentialism…because they explore the meaning behind death, our lives and meaning of suffering.”
Extending on the smoother EOL transition discussion, participants suggested initiating early conversations about EOL issues with healthy older adults to help them prepare and establish peace of mind, as detailed by Sophie, “death doulas placed in palliative care centres and elderly healthcare facilities or community support facilities where they talk to these people and support them in preparing EOL for even people that are not in palliative care.” Reinforcing the potential benefit of a death doula, a family member reflected in the VAD WA Annual Report (2023): In retrospect, I would like to have had the option of a death doula to help us navigate those peri and post-death times…the shock of the final moment, when you know the soul is gone and the vehicle is all that remains is quite profound (p. 10).
Supporting Families’ Transitions
According to the caregiving model, VAD transitions are divided into three stages: role acquisition (patient’s decision to apply for VAD), role enactment (assisting with VAD implementation), and role disengagement (patient’s death), with each stage presenting unique stressors for caregivers who face significant emotional and physical burdens, managing both increasing patient dependency and their own emotional struggles with the impending loss (Waldrop et al., 2005). Participants empathised with the dual challenges of VAD care and general ongoing caregiving, underlining the need for psychological support for families. According to Clare, “supporting the family throughout the process is so important because it is a really confusing space to be in” and Mike, “VAD doesn’t affect just the individual, this affects the entire family system surrounding them.”
Participants identified anticipatory grief, characterised by mourning before an expected loss as particularly relevant in the context of VAD. Anticipatory grief in VAD is distinct due to its time-bound nature, with death occurring at a predetermined date. Participants viewed this as supportive of adaptive grieving, leading to more positive outcomes because of the certainty and control involved (Patinadan et al., 2022). VAD is perceived “as a groomed rather than a shocked death (Jerry)”. John envisaged, “VAD may be less traumatic in that their loved ones are dying with dignity, you know, retaining control over their life and they’re able to make time to say goodbye” Pip added, “…you might have some closure”. Leah shared, “VAD can facilitate an easier grief process, take the unpredictability out of it.”
Participants discerned that as the scheduled VAD date approaches, the need for psychological support may be imminent due to emotional turmoil and second-guessing the decision. According to the VAD VIC Annual Report (2023), 16% of applicants between June 2019 and June 2023, withdrew their applications. Lily thought, “I do imagine that there would probably be a greater sense of anxiety around the upcoming date” and Pip indicated, “there’s always going to be an element of doubt toward VAD choice.”
Disenfranchised grief, a loss unacknowledged by society or hidden due to fear of judgment is also applicable to VAD. Participants felt that limited VAD communication at both personal and community levels, along with the “gag clause,” contribute to social stigma, negatively affecting VAD-related grief and loss experiences. Amelia revisited her experiences with two previous clients whose elderly parents passed by VAD, “there was still just this sense of uncomfortableness, and I think part of the challenge was their families weren’t very open with their communication.” Joe queried, I’m wondering why we (healthcare professionals) can’t bring up VAD (gag clause imposed on some States), but we can actively talk about suicide. Are we not allowed to talk about VAD because we’re increasing the risk of someone doing it? And if that’s the case, are we saying that’s inherently bad? But also, when we don’t talk about something, we know that increases stigma.
The feedback for more open VAD communication was echoed by a VAD contact person’s statement provided in the VAD VIC Annual Report (2023): VAD should be discussed more openly in the community. Healthcare providers can’t mention it unless the patient brings it up. This means people can’t make informed decisions as they don’t have all the information – it’s important for people to know it’s an option (p. 26).
Grief is a process, affecting each person differently and individuals navigate uniquely (Gerber et al., 2020). Participants anticipated that guilt, shame, and anger would be key emotional grieving responses due to the families’ deep involvement in the VAD process, from accessing VAD substance to witnessing death and managing post-death arrangements. Sam articulated, “people may feel guilty in supporting their loved one’s decision to engage VAD and similarly in the other direction, feel ashamed afterwards in not supporting their loved one’s decision” and Mike agreed, “the psychological consequences of bereavement, grief, guilt, shame, anger that other members will experience because of this person’s VAD decision…has a real outflow effect and a psychologist can be really crucial in that.”
There is diagnostic distinction between acute grief and prolonged grief disorder, where prolonged grief is persistent, disabling, and impacts daily functioning (APA, 2022). Participants perceived that family members who opposed or reluctantly accepted a VAD decision might be at higher risk of maladaptive bereavement. Family and community group therapies are recommended as beneficial in resolving family conflicts or supporting post-VAD grief. George stipulated, Makes sense for there to be the option for people to come together in a group whether that’s within their family or with people going through a similar thing and to have that extra social support…helps people to process grief better and to foster resilience.
Participants realised the importance of acknowledging that individuals may experience VAD loss as distinct from other types of death. Leah elaborated, In the grief space, people say you don’t understand unless you’ve experienced it. I’ve never had someone talk about their depression that way or their anxiety that way, or trauma that way…if I was running a group and had some people who experienced death by suicide, others who experienced natural deaths and people who experienced the death of loved ones through VAD, I would have concerns about managing group dynamics and having VAD loss valued equally to the other. I see space for separate group support.
Furthermore, one of the major findings from the VAD WA Annual Report (2023) was the lack of VAD grief and loss support for families as quoted by a family member, “I felt that the system lacked the emotion for those left behind. There was no counselling offered at the time which would be invaluable to me. Nearly 12 months later, I am still struggling with the loss” (p. 10).
Participants also highlighted differences in grieving for older versus younger individuals and the nature of their relationships. While VAD deaths are more common among older adults, terminally ill individuals over 18 also access VAD. In VIC, 5% of applicants were aged under 49 years (VAD VIC, 2023); in WA, 3% (VAD WA, 2023); and in QLD, 7% (VAD QLD, 2023). Sasha explained, “…most commonly it’s the death of a grandparent or a parent, which is still incredibly painful, but you know much more difficult when it’s a sibling, when it’s a child, when it’s a partner.”
Participants commented that societal expectations often dictate how grief is expressed, such as wearing black and being solemn. However, in VAD deaths, families may feel conflicted by these norms because they experience relief and happiness for their loved one’s autonomous decision to end suffering (La Brooy et al., 2024). Psychoeducation seems crucial to dispelling bereavement myths. Psychologists can help differentiate between healthy grief and prolonged grief disorder. As Amelia shared about her ex-clients who have experienced VAD-death of elderly parents, “they feel guilty to not feel as bad. Like it is hard when they feel like happy”, and George expounded, The way we respond to death is partly socially determined in some way or socially influenced, and there’s a lot of stigma around suicide or VAD. I do think that people’s reactions are bound to be different in those situations and general societal attitudes to dying play into it.
Fostering Psychological Safety
Healthcare professionals collaborate in a complex, dynamic environment to ensure patient safety, making psychological safety for staff in healthcare settings critical (O’Donovan & Mcauliffe, 2020). Participants concurred that those involved in the VAD process should have access to Employee Assistance Programs (EAP), like other high-stakes professions, as June mentioned, “like EAP where psychologists can put together an assistance program to help support the medical team.”
The VAD phenomenon is sensitive and emotionally charged, sparking diverse views and feelings (Auret et al., 2022; Digby et al., 2022). VAD legislation acknowledges this moral diversity by granting healthcare providers the right to opt out of VAD participation (i.e., conscientious objection). This has led to potential division within institutions, as some professionals choose to practice VAD while others, including entire organisations, may oppose it, creating tension within VAD practice. Key psychological safety enablers like organisational support programs, non-punitive culture and strong team working relationships may be hampered when opinions on VAD diverge, compromising a conducive work environment. Restricted communication or fear of backlash for one’s stance or practice can undermine psychological safety, making professionals less comfortable speaking up or sharing knowledge (Ito et al., 2022; Newman et al., 2017). Participants viewed a psychologically safe workplace as fundamental to fostering high-quality patient care and well-being of medical practitioners. Misalignment of VAD values within institutions, coupled with differing individual moral views, can fragment work culture, lowering staff morale and impacting the quality of patient care.
Additionally, for medical doctors, specialists and nurses, VAD decisions involve ending a life, which can have significant mental health repercussions. Pip observed, Making sure that the medical professionals who are administering the lethal substance have the proper mental health support given the backlash that they might get from colleagues, from friends and family, from general people in the community passing judgement as this person who kills people, like “Dr Death”, but that’s your job. And making sure that the person has the appropriate support to be able to carry the emotional demands of this important role.
Participants recognised moral injury as a well-being threat for VAD healthcare providers, which occurs when actions or witnessing events violate one’s moral or ethical beliefs (DeBeer et al., 2023). VAD is perceived to conflict with the “do no harm” ethos central to the medical profession. Spirituality and religiosity are strongly linked to moral injury, as medical teams struggle with their beliefs while feeling obligated to serve patients. Emotional consequences of this include burnout and trauma (Thibodeau et al., 2023) accentuating the need for targeted psychological support.
VAD medical practitioners may encounter displaced blame or anger from patients and their families. Fiduciary trust is crucial as patients depend on healthcare professionals in their vulnerable state. Institutional betrayal occurs when perceived harm is done by entities that individuals trust, either through action or inaction. Trust between doctors and the broader healthcare system is interconnected, and betrayal can flow between them (Smith, 2017). VAD applicants experienced barriers such as facilities refusing to cooperate or allowing VAD administration on-site (VAD VIC, 2023). VAD rejections and related complications can also cause VAD applicants/users and families to feel betrayed by both the system and medical practitioners. Jerry espoused, “you’ve got someone to blame, you can be angry at the doctors to vent…it creates an opportunity for displacement.”
Participants saw psychologists as valuable mental health contributors who are capable of sharing VAD support workload with the authorised medical practitioners to reduce their risk of burnout, errors, and attrition in VAD practice. Joe promoted, Psychologists could have a role in being included in VAD conversations to help the person, with their family and their partners. GPs (general practitioners) can be supported by psychologists who have intimate knowledge of the family dynamics and the person’s thinking, whereas GPs do not have the time because they see up to 20 people a day.
Strategic Role Differentiation
Participants argued that while social workers can offer general VAD well-being support, psychologists are uniquely suited for the strategic role. This includes research, developing specialised programs, and training social workers, carers and families to improve patient-centred care. Psychologists are key to creating evidence-based programs that integrate mental healthcare into VAD services and for leading community-based psychoeducation to educate the public and advocate for future VAD reforms. Jerry concluded, I think in most instances, social workers and counsellors are as good and less expensive providers. I think psychologists might have something to do with designing the health care system. This is the appropriate role for psychologists when we’re trying to figure out what the (VAD) system should be because we’re able to use measurements to measure if an intervention or system is working effectively.
Discussion
Exploring and understanding the perspectives of PRPs on VAD are important in the early phase of VAD implementation in Australia to address gaps in psychological support for key VAD stakeholders. The four main themes identified are ‘Values’, ‘Fit-for-Role’, ‘Exposure’, and ‘Contributions’. The study revealed participants’ pro-stance on VAD for the terminally ill, aligning with the “good death” ideology, which respects dying patients’ autonomy to die as they choose (McNamara, 2004). They also expressed being in favour of VAD for dementia patients. Concerns arose about extending VAD to mentally ill individuals, due to their vulnerability and potentially challenged decision-making capacity, reflecting a generally cautious approach toward the VAD eligibility safeguards.
Additionally, the study found that while participants’ values and qualifications were suitable for providing psychological support for VAD-related issues, disincentives such as stress, workload, and inadequate remuneration negatively impact their intentions to participate. Ethical concerns, including fear of litigation and discomfort with death, further discouraged involvement. Despite their fit for VAD roles, participants highlighted the need for relevant training and clear ethical guidelines to mitigate VAD involvement barriers and to ensure sound professional practice.
Participants reported limited exposure to EOL care due to the psychology sector’s historically low involvement in aged and palliative care. Limited VAD knowledge further encumbered engagement. Participants stressed the need for psychoeducation, training and PD to promote psychologists’ involvement with VAD and underscored the importance of addressing gaps in exposure and practice guidelines for psychologists to competently and confidently participate in VAD.
The valuable role psychologists could play in supporting patients, families, and healthcare professionals throughout the VAD process and beyond was reinforced by participants who highlighted that major participation obstacles include a lack of formal training and operational guidance for VAD practice. Participants emphasised the importance and necessity for psychological services in navigating life transitions, managing grief, and fostering mental well-being for key VAD stakeholders, suggesting the need for improved education and increased placement opportunities for formalised training as well as the systemic investment and integration of psychology into the VAD domain.
Limitations and Strengths
The findings of this study are contextually situated and may be transferable only to populations similar in nature to the sample. While participants had limited direct experience with VAD, their perspectives provide valuable insight into how PRPs engage with complex EOL issues at an early stage in their careers. The relatively large sample for qualitative research and the use of in-depth, one-on-one interviews enabled the collection of rich, detailed narratives. A key strength of this study lies in the shared professional background between the researcher and participants, which likely fostered rapport and deeper reflection during interviews. This reflexive positioning contributed to the richness and authenticity of the data.
Implications and Future Research Directions
The findings of the study suggest that psychologists can play a critical role in providing mental health support throughout the VAD process. However, the limited exposure to VAD education, training and insufficient involvement highlights a need for curriculum review, more placement and PD opportunities as well as systemic inclusion of psychologists in VAD-related services. Addressing psychological support requirements for VAD applicants/users, families and healthcare providers (including medical practitioners) are paramount, and increasing government support and stipulating clear ethical guidelines can foster better integration of psychologists into this expanding field.
Future research could triangulate psychologists’ insights with those of other key stakeholders such as social workers, medical team, and VAD coordinators to uncover both shared and differing views on psychological support needs. In-depth qualitative work with VAD recipients and their significant others, including younger applicants and individuals from diverse cultural backgrounds, would help illuminate patient-centred requirements. Additionally, examining the experiences of psychologists already engaged in VAD practice may clarify training needs and optimal service models.
Considering the inevitable aging of the Australian population and rise in chronic illnesses, the demand for VAD is expected to rise. Hence, engaging psychology’s curriculum and psychologists’ exposure to and training in VAD-related issues are both timely and essential to meet future VAD-related mental health needs effectively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.