
Abstract
This qualitative, phenomenological study described ICU nurses’ lived experiences caring for patients with COVID-19 while trying to engage in self-care and care for their families. Eleven ICU nurses shared their individual experiences working in a hospital ICU. Watson's theory of Caring Science guided the study to ensure a holistic interpretation of the data. Six themes and fifteen subthemes emerged, which revealed that ICU nurses faced barriers to self-care. The conclusion of the data analysis was that hospital leaders need to make Caring Science evident to ICU nurses during crises by trained Caritas coaches to build resilient frontline nurses through compassion.
Background
ICU nurses faced challenges to self-care such as caring for patients with COVID-19, compassion fatigue, inadequate staffing, and inadequate supplies. Other concerns, including the health of ICU nurses, ICU nurse's self-care, mindfulness, resilience, and ICU nurses caring for their families, were identified in the literature (Carbajal et al. 2020; Shen et al. 2020). However, conclusions about what ICU nurses experienced while caring for patients with COVID-19 were inconsistent and possibly misunderstood.
The stress ICU nurses generally experience while caring for patients was exacerbated by the COVID-19 pandemic (Sperling 2021). While ICU nurses struggled to provide care for increasing numbers of patients with COVID-19 throughout the initial pandemic the nurses dealt with their own fears of contracting the virus (Sadang 2021). ICU nurses may not have had the tools and support needed to do their job (Sperling 2021), care for themselves, and care for their families.
The stressors stemming from their roles, both clinical and personal, tended to overwhelm some nurses. Often, nurses became family for patients with COVID-19 and were usually the only person at the bedside of the patient who was dying (Stilos and Moore 2020). Providing ICU nurses with opportunity to practice self-care would positively impact their wellbeing and reduce some of the stressors they experienced (Watson 2018).
As the number of patients with COVID-19 increased and flu season began across the United States, ICU nurses measured the risk of staying in the patient care workforce versus leaving their position to achieve peace and safety for themselves and those they love. ICU nurses must feel supported and cared for instead of fearing they will die while doing their job because of a lack of adequate supplies (Carbajal et al. 2020). The aim of this study was to describe ICU nurses’ lived experiences caring for patients with COVID-19 while engaging in self-care and care for their families. The following research questions were explored: What are ICU nurses’ lived experiences with caring for patients with COVID-19 as the pandemic continued? and What are ICU nurses’ lived experiences with caring for themselves and their families while caring for patients with COVID-19?
Watson's Theory
Watson’s (2018) Theory was used to understand how nursing as a caring practice is rooted in emotional and sacred spiritual values via Unitary Caring Science. Healing is understood to be a holistic process, which involves intention, recognition, love and kindness. Watson offered a philosophy by which nurses can live to take care of patients in a sustainable way and, in doing so, care for themselves. Watson's Unitary Caring Science can help nurses strengthen their core values and prepare for the worst situations through self-care and kindness. When nurses are experiencing increased stress, Watson invited them to be mindful of their consciousness and be present in the moment.
Watson (2018) explained a lack of growth could reflect on caring for others. If nurses are unkind to themselves, they can hurt their patients and coworkers. Nurses often give of themselves sacrificially and neglect their own needs to care for others. Watson's theory has been used to develop practical programs to support nurses. Van Wijlen (2017) applied Watson's Caring Science approach to advocate for a reexamination of how nurses should be caring for themselves in practice and be educated to care for others and themselves.
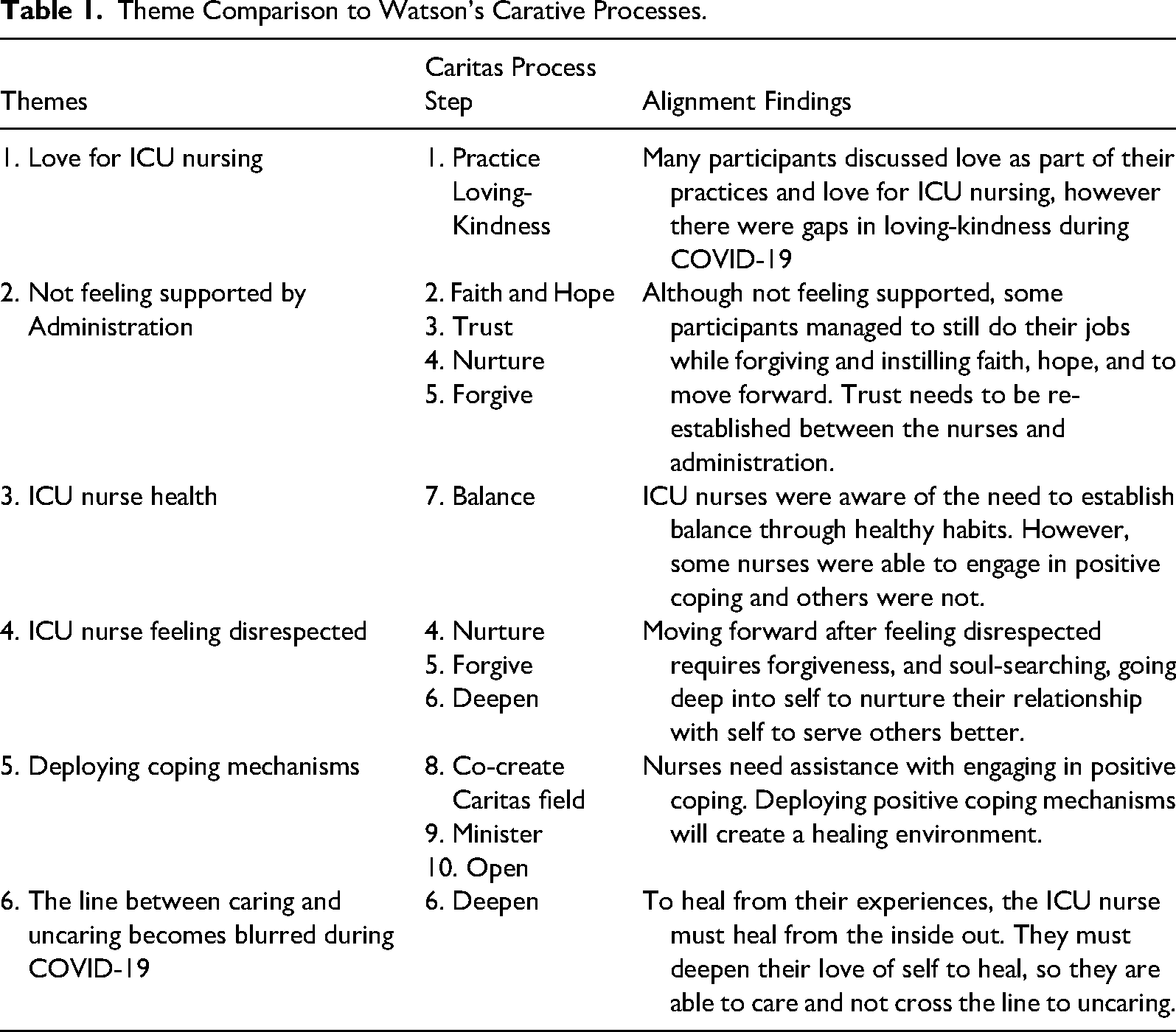
For ICU nurses caring for patients during the COVID-19 pandemic, Watson's framework could have been a critical way to approach self-care. (See Table 1)
Theme Comparison to Watson's Carative Processes.
Because of measures like isolation, nurses and patients were separated from sources of support and nurses found themselves the sole human support for patients who were fighting for their lives. Being the sole support can exhaust nurses mentally and emotionally. Witnessing the pain and sadness of patients could also lead to burnout. Using Watson's framework, nurses are not asked to compromise the expression of their emotions and authentic compassion but to provide ways to hold onto those values by being as kind to oneself as to others, thus reinforcing the foundational values of care. Nurses need to learn how to self-care through healing the healer (Van Wijlen 2017).
Watson's Theory of Human Caring/Caring Science provided a framework for understanding the experiences of ICU nurses caring for patients with COVID-19 during the pandemic of 2020–2021. The theory emphasizes the importance of self-care for nurses, which is essential for incorporating transpersonal caring. While a Magnet hospital in this study followed Watson as their nursing theorist, some participants discussed their experiences with not feeling cared for. Watson's theory suggests that professional nurses focus on caring for others rather than curing them and that self-care is essential to enable nurses to better care for others.
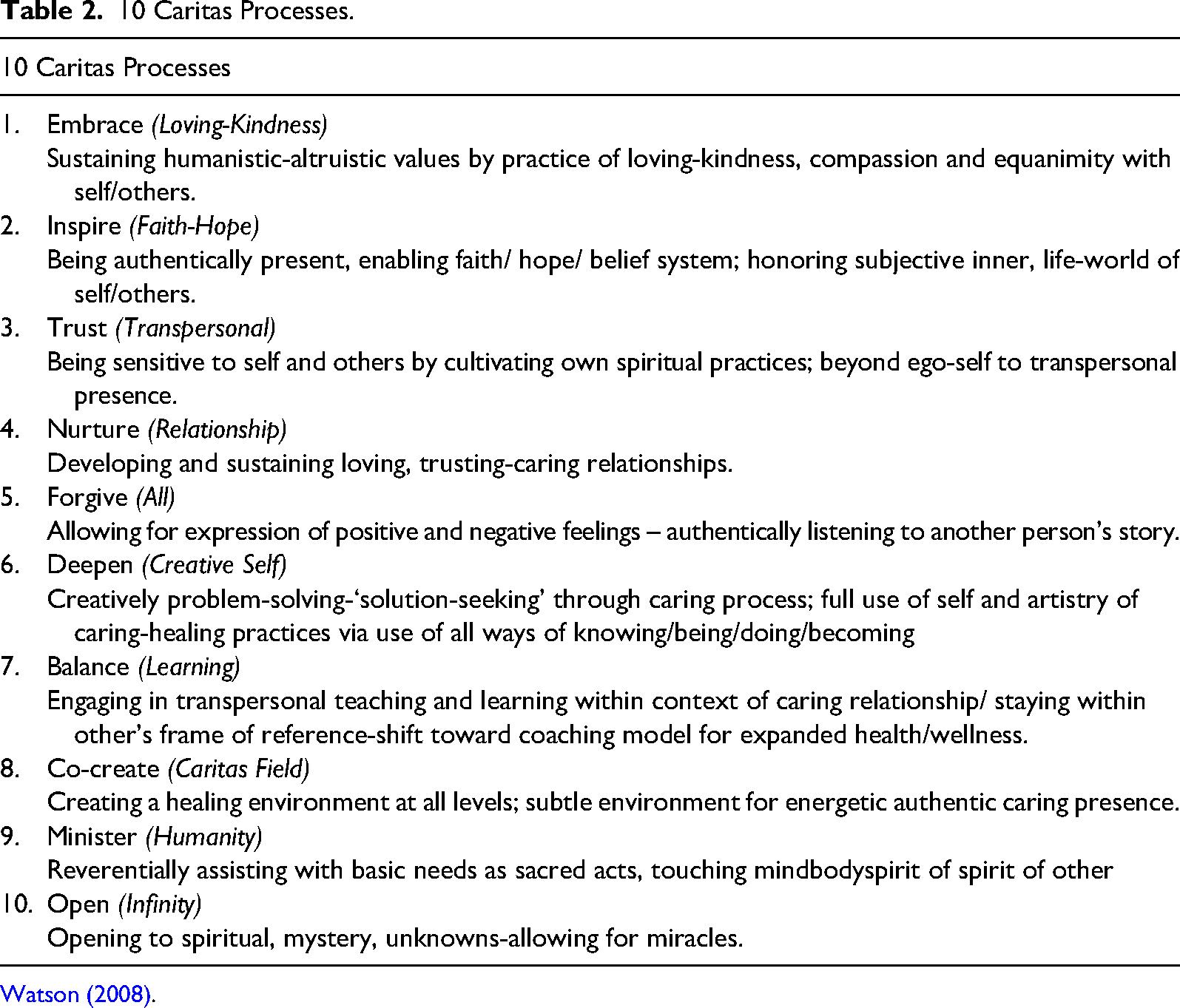
The current study's findings indicated that some of the emerging six themes aligned with Watson's theory, while others do not. For instance, some participants felt that the administration was not effectively using Watson's theory because of the lack of care and support they experienced. The 10 Caritas process (see Table 2) provides a framework for transforming an organization from the inside out by implementing specific care techniques that deepen and sustain individuals’ shared humanity. In interpreting the themes that emerged from participant experiences, the Caritas processes of Watson's theory were not always present.
10 Caritas Processes.
RQ 1 – Theme 2, not feeling supported by the administration, aligned with the Caritas process but not positively. RQ 1 – Theme 3, ICU nurse health, aligns with Caritas process number seven, which emphasizes the need for balance as nurses ask for help, particularly with their mental health. RQ 1 - Theme 4, ICU nurses feeling disrespected, represents a negative example of the fourth, fifth, and sixth Caritas processes. See Table 1 for a comparison of each Caritas Process and the themes revealed in this study. Overall, the study highlighted the importance of incorporating self-care and transpersonal caring into nursing practice, particularly in the context of caring for patients with COVID-19.
Method and Design
Qualitative methods were used to describe ICU nurses’ lived experiences caring for patients with COVID-19 while maintaining self-care and caring for their families. A phenomenological design using an interpretive approach revealed the meaning of the lived experiences of ICU nurses. The outcome was an interpretation of how ICU nurses made meaning of their firsthand experiences in which they exercised openness, empathy, and reflexivity.
Population and Sample
Eleven ICU nurses were selected from a population of 123 day and night shift ICU nurses in one large hospital in western United States. The participants were registered nurses for more than 17 years with more than 15 years of ICU experience. Their age ranged between 40 and over 60 years. Most were female. Following approval from the organization's IRB and before conducting the study, each participant received an explanation of the study, ensuring informed consent and confidentiality for participants.
Instrumentation
The primary instrument was the primary investigator who conducted semi-structured, one-on-one, open-ended interviews. She was an ICU nurse who had cared for patients with COVID-19 since the beginning of the pandemic in an ICU setting that was not in the same hospital as the participants. The semi-structured interview questions provided an opportunity to explore the nurses’ experiences and develop a discussion around the experiences. The interviews were audio-recorded and transcribed, which provided texts that could be further interpreted.
Data Collection and Analysis
Voluntary participation consisted of a one-time 60-min, audio-recorded, one-to-one, Zoom interview. Due to COVID-19, the semi-structured interview questions were asked using the Zoom platform. Data were collected from interviews using semi-structured, open-ended questions with probing questions to encourage participants to look deeper into their lived experiences. As part of the hermeneutic process, some participants required the use of probing questions in addition to the semi-structured interview questions to ensure participants relayed in-depth information. All audio recordings were transcribed and emailed to each participant to confirm the accuracy of the transcription. Upon verification of transcription from the participant, the audio files were deleted, and only the transcriptions were saved. Once the interviews were completed, the researcher updated the field notes and transcribed the interviews.
Results
Data analysis revealed four themes and 10 subthemes associated with research question (RQ)1 about how ICU nurses experienced caring for patients with COVID-19 during the early phase of the pandemic: RQ1 - Theme 1) love for ICU nursing, RQ1 -Theme 2: not feeling supported by administration RQ1 - Theme 3: ICU nurse health, and RQ1 - Theme 4: ICU nurses feeling disrespected. The answer to RQ 2 about how the ICU nurses cared for themselves, and their families yielded two themes and five subthemes. However, the data for RQ2 were not fully saturated because the nurses wanted to focus more on their experiences in ICU. The themes were: RQ2 - Theme 1: deploying coping mechanism and RQ2 - Theme 2: the line between caring and uncaring becomes blurred during COVID-19.
Discussion
To answer RQ1, “What is the meaning of the ICU nurses’ lived experiences with caring for patients with COVID-19 during the early phase of the pandemic?” the four themes were compared to existing literature.
RQ1 - Theme 1: Love for ICU Nursing
All 11 participants mentioned their love for the ICU. Prior to COVID-19, participants in this study loved their jobs as ICU nurses. Most of them chose to become ICU nurses because they had an apparent love for the profession. Many shared how they loved taking care of ill patients and were fulfilled when their patients recovered. One participant stated, “I love nursing, and I’ve never wanted to do anything but ICU.”
Participants recalled things like spending time together outside of work and functioning independently as some of the reasons they loved ICU so much. The memories participants shared were vividly described during the interviews and provided sufficient data to support two individual subthemes: 1) experiencing autonomy and 2) working and doing things together. The participants explained, “The biggest reason I loved ICU was the autonomy” and “I love being an ICU nurse. ICU nurses have a significant degree of autonomy.” For RQ 1 - Subtheme 2, the participants said, “I loved the camaraderie and the friends” and “We all scheduled ourselves and made sure we worked the same shifts.” The findings of the current study supported previous studies that identified that the ICU nurse who cared for patients with COVID-19 loved nursing (Sadang 2021). The finding of the current study agreed with previous findings that nurses felt self-fulfillment and a genuine love for the field (Sadang 2021).
RQ1 -Theme 2: Not Feeling Supported by Administration
Participants in the current study compared their experiences during the pandemic to their past experiences, stating that they believed the ICU unit functioned effectively before the pandemic. While they loved their work in the past, a few participants indicated they were planning to leave the hospital to seek other opportunities in healthcare due to the negative experience during the pandemic. Participants felt they were ready to leave their work if they earned the same pay in another job.
When discussing their COVID experiences, some participants became angry while criticizing hospital administration for not providing them with the necessary materials and resources to adequately do their jobs, particularly personal protective equipment (PPE). One participant said, “There was not enough of anything. We even made our respirators because there were not enough N-95 masks” Another reported, “The N-95, we were issued one to last a week or the three days you worked although many of us worked overtime and 4–6 shifts a week.” Some participants indicated that they created makeshift PPE out of old equipment and reused some of the single-use PPE, which put them at risk.
Participants also compared their experiences to being in a war-like situation, with management doing little or nothing to address their concerns about working long hours or being short-staffed. One participant said “…we were in a battle zone. I felt like I was living at the times of the Crimean war, you know, back in Flo's days. We were working in places not meant to handle ICU patients, but we did.” Another participant stated, “It made me feel like the military. I was sacrificing my safety for total strangers.”
Many participants blamed both administration and the government for the inappropriate supply of PPE. ICU nurses were willing to sacrifice their time and energy to win the war and save the lives of their patients, but they felt unsupported by their administration. Some participants complained about excess workload and working longer than regular hours. One participant said, “I worked 60–70 h a week.” Another shared, “We could have died working 12–24-h days, right there with the sickest of the sickest.” Participants felt “The government surely doesn’t have our back. This was war. COVID hit like a tsunami with force, and it has been hell.” These findings agreed with findings in a study conducted in Iran (Ahmadidarrehsima et al. 2022).
The findings of this study contradicted previous reported findings in other hospital systems (Oehlert et al. 2022; Sun et al. 2020) In a health care system where nursing leaders supported nurses by using Watson's human caring theory, nurses reported that they had space for self-care and felt supported by nursing administration. The nursing leaders provided various approaches to support a culture of well-being (Oehlert et al. 2022).
RQ1 -Theme 3: ICU Nurse Health
The third emerging theme described concern for ICU nurse health and how some participants reported experiencing depression and mental breakdowns due to the unprecedented number of deaths. One interview question asked participants about how their experience has changed as the pandemic continued through multiple waves. Many participants related this interview question to their health and struggles.
One participant volunteered, “We have so much pain. I am sick of it.” Another recalled, “I remember sleeping in my car and then a tent in my backyard. Just thinking of those times makes me sick.” Still another was visibly emotional with tears in their eyes as they shared, “I know I’ve aged; I have so many wrinkles I never had and scars from wearing the damn mask. I cried every day” and one sadly stated, “We have so much pain. I am sick of it.”
Additionally, most participants attributed their feelings and emotions to post-traumatic stress disorder (PTSD). One participant said, “I honestly believe I have PTSD, my dad had it from the war, and I think I understand him now.” Again, some participants shared that although the pandemic has significantly decreased, some aftereffects remain as they continue supporting patients. A participant shared, “I can honestly say I am proud that I served during COVID-19, but I probably have PTSD; I still get a little anxiety walking into the unit or when the code blue button goes off.” Participants admitted that they would need professional help to navigate through their experiences of PTSD and mental health issues. They believed that exposure to the multiple waves of the pandemic contributed to the development of and unresolved mental health issues. Thus, the first emerging subtheme from the data was struggling with PTSD which agreed with Moore et al.’s (2021) whose participants experienced elevated stress levels.
Participants also shared that they were no longer saving patients’ lives because they went from saving lives to managing death in an environment where no family was allowed, and they were the only person near the patients who were dying. One participant shared, “I can probably count how many of my patients survived on the one hand during the first year of COVID-19. Death on top of death, I mean they were all dying.” Another participant shared the same sentiment by stating, “Death was measured by refrigerated trucks.”
Sadly, patients sometimes died alone and without touch, and nurses described their difficulty managing their thoughts about patients’ bodies, which were amassing in morgues and closets. One participant shared that their perceptions had slightly shifted, “During COVID-19, it was a matter of treating the dead,” while another described, “It got harder because death was a common theme, man. Death was a constant; it happened every day, several times a day.” Participants faced their biggest struggle as ICU nurses being surrounded by constant death, which was reflected in the second emerging subtheme of being surrounded by death. Findings from the current study were in agreement with nurses’ experiences during the SARS epidemic (Wilder-Smith, Chiew and Lee 2020).
Most participants reported often breaking down in tears. Some participants who once enjoyed working together became hostile to one another. Working in ICU during COVID-19 was a significant contrast to what participants had experienced in the past. Some participants complained about weight gain, drinking too much, feelings of exhaustion, and working mandatory overtime as there was no one to replace them. One participant 2 explicitly described, “I mean, I hate when the alarm goes off now. It just makes me sick. I am physically sick.” Another said, “They (the patients) had to be pronated every two hours. I couldn’t do it. My body was too tired.” Participants also explained how they often relied on junk food and were unable to exercise during this pandemic because of how much overtime they had to work due to the staff shortage. The abundance of overtime led participants to experience periods of exhaustion. A participant stated, “I mean truly we should be fighting for our patients, caring. But we were trying to fight for ourselves because we were trying to stay alive. I am exhausted all the time.” These findings led to the third subtheme of negative physical health issues. Some participants experienced anxiety, depression, tearfulness, and anger, while others indicated planning to leave the hospital to seek other jobs due to their negative experiences during the pandemic. These findings led to the final subtheme of adverse mental health issues. These findings agreed with findings in which lack of PPE and staff shortages led to increased mental health issues (Ahmadidarrehsima et al. 2022). On the contrary, Shen et al. (2020) found that leadership interventions seemed to mitigate nurses’ mental health problems.
During the interviews, participants’ body language demonstrated signs of pain and trauma, such as a slouched, defeated posture, tears, flat affect, and not being present emotionally when they discussed the trauma they experienced. Other participants demonstrated their anger with curse words and closed fists. One participant expressed, “I am short-tempered, angry, and depressed. Financially it may be worth it to quit and get a travel assignment. The pay is good. I no longer feel a sense of commitment to this place.” Another added, “I would leave in five seconds if you gave me a financial opportunity like this.”
The findings from the current study supported previous research which described nurses working tirelessly as they almost gave up due to working long hours, often until three o’clock in the morning many days (Sadang 2021). The current study's third theme, in which ICU nurses described how they suffered from exhaustion, is similar to nurses feeling tired found in a study by Sadang. According to Oehlert et al. (2022), healthcare worker's suboptimal health can affect their well-being and threaten the patients’ and organizations’ outcomes by affecting job performance and safety.
RQ1 -Theme 4: ICU Nurses Feeling Disrespected
The participants felt disrespected because of their perception that the public viewed ICU nurses as a source of spreading the virus to the community. Participants also felt disrespected because some employers imposed mandatory vaccinations for nurses. One participant stated, “Many nurses who didn’t get vaccinated never got COVID-19. I got vaccinated, but why all the division?” Another participant further elaborated that, “I was one of the last to get vaccinated only because I didn’t want to lose my job. I mean, the CDC has flipped and flopped so much.” Another agreed, “How can you fire ICU nurses for not vaccinating? We cared for total strangers without proper equipment and never got sick?”
These feeling of disrespect agreed with findings of a recent study that found that despite the sacrifices made by ICU nurses during the pandemic, they felt disrespected due to the hostility and stigma they experienced from society. Nurses were most worried about being viewed as carriers of the virus instead of heroes and feared that they transmitted the disease from hospitals to homes and vice versa (Ahmadidarrehsima et al. 2022) This societal issue led to participants feeling like the public was turning their backs on them and made their experiences much worse. Participants in the current study said, “Nurses felt threatened because [external] people assumed we were carrier.” and “I didn’t feel so contagious, although the public no longer liked us.” Another participant agreed saying, “First I’m a hero, then I’m bringing the disease out of the hospital.” The media's conflation of the vaccine situation also led to nurses’ perceptions and feelings about vaccine resistance.
Participants in the current study felt that their colleagues from other hospital units lacked empathy and the participants believed that people would pull away from them if they knew they worked on the COVID-19 team. Mental and physical health was a general complaint from participants, with many feeling that mental health support should have been provided to all ICU nurses. These findings were similar to the findings of another study in which many people in the community were afraid to have interactions with nurses, creating a stigma toward health workers (Sadang 2021).
Contrary to the findings of disrespect in the current study, ICU nurses in Iran were happy with their government and medical environment and found calmness and relaxation at work (Sun et al. 2020). However, some negative emotions did exist, when some nurses became upset that some of their coworkers did not want the vaccine and were fired or that vaccines were being made mandatory instead of voluntary. The findings that nurses had feelings of disrespect in this study highlight the need for society to recognize and appreciate the sacrifices and hard work of ICU nurses during the pandemic and to provide them with the necessary support and resources to maintain their mental and physical well-being.
RQ2 Themes – Discussion
RQ 2 asked, “What are ICU nurses’ lived experiences with caring for themselves and their families while caring for patients with COVID-19? Participants provided a mixed response to the interview questions aligned with this research question. Two themes, RQ 2 – Theme 1) deploying coping mechanisms and RQ 2 – Theme 2) the line between caring and uncaring becomes blurred during COVID were compared to existing literature. The themes were compared to previous studies of ICU nurses.
RQ 2 Theme 1. Deploying Coping Mechanisms
Participants reluctantly discussed how they cared for themselves and their families during the pandemic. Some nurses described ways they activated positive self-care mechanism through choosing healthier eating options. They shared, “I, for one, make sure I eat well, we know that COVID-19 likes sugar, so I have cut back because I have a sweet tooth” and “I am trying to make smoothies at nighttime and drink some decaf or tea, it has been about three weeks without a drink, but I am just taking a day at a time.” The responses provided insight into participants’ coping strategies and the challenges they faced. One participant said, “I was so out of balance and needed immediate relief to cope.” Some nurses described the poor choices they made. One participant acknowledged that when faced with dealing with the death of a patient “…I lost it; I just screamed at them in the unit. I said I just have to quit now because I cannot handle it anymore. I realized that I was not coping well and needed help.” Another said, “I ate way too much and drank much wine. I would just come home and veg in front of the TV.”
Some participants also explained how they tried to incorporate regular exercise into their routines. For example, participants said, “I did some yoga”; “I walk a lot and just try to be active”; “I don’t smoke or drink, and when I get stressed, I run.” Only one participant shared how they relied on family support to cope, “I have a wonderful man who supports me and listens and allows me to vent and wants to take care of me, and he does so very well, that was a big part of how I was able to cope.”
Mental health breaks were also one of the forms of self-care discussed by participants. One participant described, “There was a quiet room put together for meditation or Watson's self-care time, you know the hospital nursing theorist. I am working on my minutes in there.” Another participant mentioned their faith, “I relied on and hoped that things would get better by trusting in God, pretty much, just trusted God and hoped He had things under control.”
Some participants found caring for their families more difficult over time, which may have contributed to their poor coping choices. The study identified two subthemes of coping mechanisms: positive self-care and poor coping choices. While negative coping strategies provided immediate relief, they often brought on other problems. The findings of the current study emphasized the importance of positive self-care and the need for mental health support during times of stress and crisis. The findings of the current study were similar to other studies that identified exercise, good nutrition, and reliance on God as effective coping mechanisms (Ahmadidarrehsima et al. 2022).
The findings of the current study refuted the findings of previous research, which identified only positive coping mechanisms such as psychological adjustments, team support, and rational cognition among nurses (Sun et al. 2020). The findings of the current study emphasized the importance of positive self-care and the need for mental health support during times of stress and crisis.
RQ2 Theme 2: The Line Between Caring and Uncaring Becomes Blurred During COVID
Participants described what caring meant to them during the pandemic. Most of the participants equated caring with feeling safe and believed that it involved ensuring individual safety. Many participants associated caring with working in a caring hospital, and some discussed Watson's theory and the availability of the caring room in their ICU unit. To keep their families safe during the pandemic, many participants stayed away from them or isolated themselves. One participant explained, “My family has had to suffer because I am caring for total strangers, risking my own life.” Another participant stated, “I stayed isolated for quite a while to keep my family safe.”
Participants also shared that caring for the dead during the pandemic did not match their idea of caring. Many of the participants continued to express disappointment about their perception about the lack of caring despite practicing in a hospital that asserted the use of the caring philosophy for some time. Some participants felt that management did not care about their safety, which discouraged them from caring for others. One participant said, “My coworkers stopped caring. We went from a caring environment to an uncaring environment overnight.”
When relating their experiences with inadequate PPE and resources, as well as exhaustion due to staffing and administration issues, participants expressed their frustrations. Some nurses were not allowed to see their family members who had died due to COVID-19 restrictions at different hospitals, despite having COVID-19 experience. The finding of blurred lines between caring an uncaring were supported by findings from other studies that showed that some nurses lived in their backyard or garage for some time or did not visit their families at the beginning of the pandemic to keep them safe (Ahmadidarrehsima et al. 2022; Sun et al. 2020).
Limitations
Recruitment of participants for this study was challenging because potential participants feared losing their jobs if they were honest in answering the interview questions. Some nurses asked if they could give another name versus providing their real name and they asked if their identification would be verified. Although the study was open to all nurses employed in the ICU, data saturation was only met for female nurses’ perspectives about their experience working in the hospital ICU. Fewer male ICU nurses participated in the study than women, thus a recommendation for further inquiry into male ICU nurse experiences be considered to provide a complete understanding of ICU nurse experiences with caring for patients with COVID-19. Additionally, no nurses under the age of 40 participated in this study. Thus, this study was limited to exploring nurses’ lived experiences working in ICU who are forty and over. Data saturation of the participant experience in caring for families was not attainable in this study as most participants spoke about their personal experiences on the frontline and only one participant discussed the death of a family member during the pandemic.
Recommendations
This study found that ICU nurses who were caring for patients with COVID-19 believed that having adequate resources for nurses is essential to their safety and well-being. Participants interpreted that a lack of resources indicated a lack of care from the administration. As a result, participants harbored frustration, anger and a lack of trust toward management. Adequate resources extend beyond personal protective equipment and should include mental health support for nurses and a platform for them to voice their concerns. Executives of the organization should participate in the leadership training offered by the Watson Caring Science Institute. Developing and implementing a continuity plan to address staffing needs during a pandemic could mitigate stress and exhaustion. COVID-19 has reset the standard of care and nurses are now feeling unappreciated more than ever. Administration could call every ICU nurse just to see how they are doing and if they need anything. A simple two-minute call to make an assessment of those fighting on the frontline may provide comfort. The greatest insight from participant interviews is that nurses needed to feel cared for and should perceive that their leaders are taking care of them. Participants wanted nursing leadership to ensure that nurses were adequately prepared and had the resources to do their day-to-day jobs. The nurses desired to work in a caring environment.
Further research is recommended on the effectiveness of Caritas coach training and the 10 Caritas processes dealing with healthcare pandemics and Caring for nurses’ families. If the nurses’ families were cared for the nurses may focus without worry about their loved ones. In addition, there is a need for further information with retention of ICU nurses and innovation to improve mental care including posttraumatic caregiving during COVID. As more studies are conducted, systematic reviews and meta-syntheses can be done to address the pandemic's impact on nurses who cared for patients with COVID-19, especially those nurses who left bedside nursing due to this pandemic. Finally, a larger sample that included younger nurses may bring light to why there was such a mass exodus of ICU nurses both young and seasoned nurses who left the profession. The younger nurses cost the organizations the money invested in their training that and those seasoned nurses took their years of experience and priceless wisdom.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.