
Abstract
Introduction
Previous studies have shown that, during the coronavirus disease 2019 (COVID-19) pandemic, nurses were being reassigned to non-COVID-19 wards, opting to take leave, or resigning because of concerns of infecting their families. Even so, many nurses decided to continue working. However, a literature review revealed a lack of research clarifying how nurses coped with their anxiety and came to the decision to work in a COVID-19 intensive care unit.
Objective
To determine the process by which nurses living with their families decided to work in an intensive care unit during the COVID-19 pandemic and the factors that influenced their decision.
Methods
Fifteen registered nurses who lived with their families and decided to work in a COVID-19 intensive care unit during the pandemic were recruited for an individual, semi-structured interview. Charmaz's constructivist grounded theory was used to analyze the transcripts.
Results
Four core categories were identified. When the nurses perceived their facility would accept a patient with COVID-19, they: (1) assessed the risk of infection to their family, (2) weighed their anxiety against their sense of mission, (3) reduced the risk of infection, and (4) discussed the decision with their family members.
Conclusion
The decision involved fear of infecting families, trust in the hospital, and sense of mission. Hospitals’ consideration of the situation was important in motivating employees and reducing anxiety. There was a gender bias in this study. The large number of male participants resulted from the characteristics of the participating COVID-19 intensive care units, reflecting gender roles in Japan, where men often work and women are responsible for housework and childcare. Facilities and managers should foster a workplace culture that values employees, even in ordinary times. Our findings may help healthcare organizations support nurses in an emerging infectious disease pandemic and ensure nurses are available in healthcare systems with limited resources.
Introduction
In 2020, the coronavirus disease 2019 (COVID-19) pandemic caused tremendous emotional distress among nurses providing frontline care. Ching et al. (2021) noted that nurses were at a particularly high risk of depression and anxiety. They stated that one-third of healthcare workers who cared for affected patients had depression, anxiety, and stress, and more than two-thirds reported experiencing fear and burnout.
Patients with severe COVID-19 require advanced life support in an intensive care unit (ICU), with interventions including artificial respiration, extracorporeal membrane oxygenation (ECMO), and renal replacement therapy. Consequently, frontline nurses experienced enormous workloads, prolonged fatigue, the threat of infection, and frustration over patient death during the pandemic (Shen et al., 2020).
Patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19, were admitted to a dedicated ICU when they required prolonged nursing care (Bruyneel et al., 2021). In a survey of ICU staff, 60% said they were at high risk of infection at work, and 76% said they were concerned about infecting their families. As a result, 37% said they “considered quitting their job” (Mehta et al., 2022). Greenberg et al. (2021) reported that almost half of ICU staff members showed symptoms of disorders such as posttraumatic stress disorder, severe depression, or anxiety, and about one in seven reported self-harm or thinking they would “rather die.” The authors reported that nurses were more likely than physicians or other healthcare workers to do so. It has also been shown that symptoms of depression, anxiety, and stress increased when nurses had an intense fear of infecting themselves or family members (Sampaio et al., 2021). Nurses spend much of their time providing direct patient care; among ICU healthcare workers, they had more direct contact with patients with COVID-19 and were more likely to express anxiety and fear of infecting themselves or family members.
For nurses caring for patients with COVID-19, “serious concerns about family safety” were a barrier to their willingness to continue working. They were particularly worried about infecting their children and parents (Joo & Liu, 2021), even when wearing personal protective equipment while working; to reduce the risk of infection, Nashwan et al. (2021) reported that some nurses ate, slept, or even lived separately from their families.
Ohue et al. (2021) discovered that nurses were being reassigned to non-COVID-19 wards, opting to take leave, or resigning because of concerns about infecting their families. Even so, many nurses decided to continue working. During the pandemic in Wuhan, China, 96.8% of frontline nurses reported willingness to work (Ke et al., 2021). In Qatar, 88.1% of nurses also expressed a willingness to provide care for patients with COVID-19 (Nashwan et al., 2021).
Review of Literature
In previous studies, nurses caring for patients with COVID-19 often described anxiety and stress related to infection of themselves and their families. However, there is a lack of research on the process by which nurses dealt with their fears of infection, how they came to the decision to work in a COVID-19 ward, and what factors influenced their decision.
Increased nurse turnover during infectious disease outbreaks poses a significant risk of healthcare disruption and presents a major problem for society as a whole. Therefore, identifying the process by which nurses with live-in family members decided to work in COVID-19 ICUs and the factors that influenced their decision may provide a basis for policy makers, healthcare organizations, and facility managers to develop measures to ensure nurses are available to work on the front lines during a pandemic.
This study aimed to determine the process by which nurses living with family members decided to work in a COVID-19 ICU during the pandemic, as well as the factors that influenced their decision.
Methods
Design
To elucidate the social conditions, work environments, and interactions with colleagues and family members that influenced the decision to work in a COVID-19 ICU, the researchers applied a qualitative research method using the grounded theory approach. Grounded theory is a method used to examine social structures and the interactions of people, which can be explained in different ways by different methodologies (Rieger, 2019). Charmaz (2006) theorizes that people construct reality through their own experiences, a position known as “constructivist grounded theory.” Based on a social constructivist perspective, this approach explores how research participants construct meaning and determine behaviors in specific situations (Charmaz, 2006). Therefore, in the social context of the COVID-19 pandemic, the focus was placed on the relationships between nurses and their live-in family members, as well as the demands of society, rather than only on individual nurses, to better understand the decision-making process and meaning of the choice to work in a COVID-19 ward despite the risk of infection. This perspective offers a deeper understanding of the decision-making process and its implications for nurses who chose to work in COVID-19 wards under such circumstances. In accordance with this aim, Charmaz's (2006) constructivist grounded theory was used to analyze the data. Through this method, it was possible to theoretically interpret how nurses’ decisions were shaped by social interactions and family influences.
The tenets put forth in the Consolidated Criteria for Reporting Qualitative Studies (COREQ) (Tong et al., 2007) were followed throughout the study design, data collection process, analysis, and writing of the manuscript.
Sampling and Recruitment
Data were collected from December 2022 to May 2023. Candidates were selected by the researchers through theoretical sampling, and participants were determined through direct recruitment or snowball sampling. The researchers had prior acquaintances with several participants.
Inclusion and Exclusion Criteria
Participants included nurses who worked full-time in a COVID-19 ICU between February 1 and December 31, 2020 and had a cohabitating family member. Eftekhar Ardebili et al. (2021) found the “fear of infecting family members” was most intense from the early stages of the pandemic to its peak. Based on this, this study focused on nurses who were engaged in the early stages of the outbreak, when infection control and treatment had not been established, vaccination had not begun, and healthcare workers were most anxious. Inclusion criteria did not restrict participants by employment at the target institutions, years of experience, or job title.
Data Collection
Interviews were conducted by one of the authors, a registered male nurse who was a master's degree candidate. Before the start of this study, he received systematic training in qualitative research and gained experience in conducting interviews. He also lived with his family and had experience working in a COVID-19 ICU.
The researcher conducted interviews one-on-one via Zoom while in a quiet place such as a conference room or home. This method allowed us to reach participants in a wide range of facilities, transcending geographic constraints (Archibald et al., 2019). It also allowed participants to answer questions while in familiar settings, such as their homes, making it easier for them to speak candidly about sensitive content (Janghorban et al., 2014). On the other hand, this method made it difficult to understand nonverbal communication (facial expressions and gestures) and was easily affected by the communication environment (Seitz, 2016). Managing recorded data and ensuring privacy are also important issues. To address these challenges, procedures such as conducting a connection test prior to the interview to confirm the communication environment were implemented, and participants were asked to provide feedback to supplement their nonverbal communication.
The interviews were recorded with the participants’ permission. All questions were asked in Japanese.
Participants chose the time and day of the week for their interview. They were asked the following questions: Can you tell us how you came to work in a COVID-19 ICU? How did you feel when you were first asked whether you could work in a COVID-19 ICU? When and how did you tell your family about working in a COVID-19 ICU? (What was their reaction?) What factors contributed to your eventual decision to work in a COVID-19 ICU? (Why?) (See supplemental materials for the interview guide.)
Reflective notes were taken after each interview to capture the participant's nonverbal communication and debrief the research team.
The study included 15 participants (nine men and six women) with between 5 and 23 years of nursing experience at the time of the interview. Family members living with the participants included spouses, parents, children, infants, grandparents, and dating partners. One participant was a single mother. One participant provided a particularly rich narrative in the initial interview and offered valuable insights relevant to the research topic. Therefore, one additional interview was conducted with this participant to delve deeper into the content and reinforce our understanding of her experience. This was the only participant for whom two interviews were conducted. No participant refused to participate or withdrew from the study. Participants worked at seven facilities nationwide, including duplicates, and all began working in the COVID-19 ICU between February and May 2020. A summary of participant characteristics is presented in Table 1.
Summary of Participants.
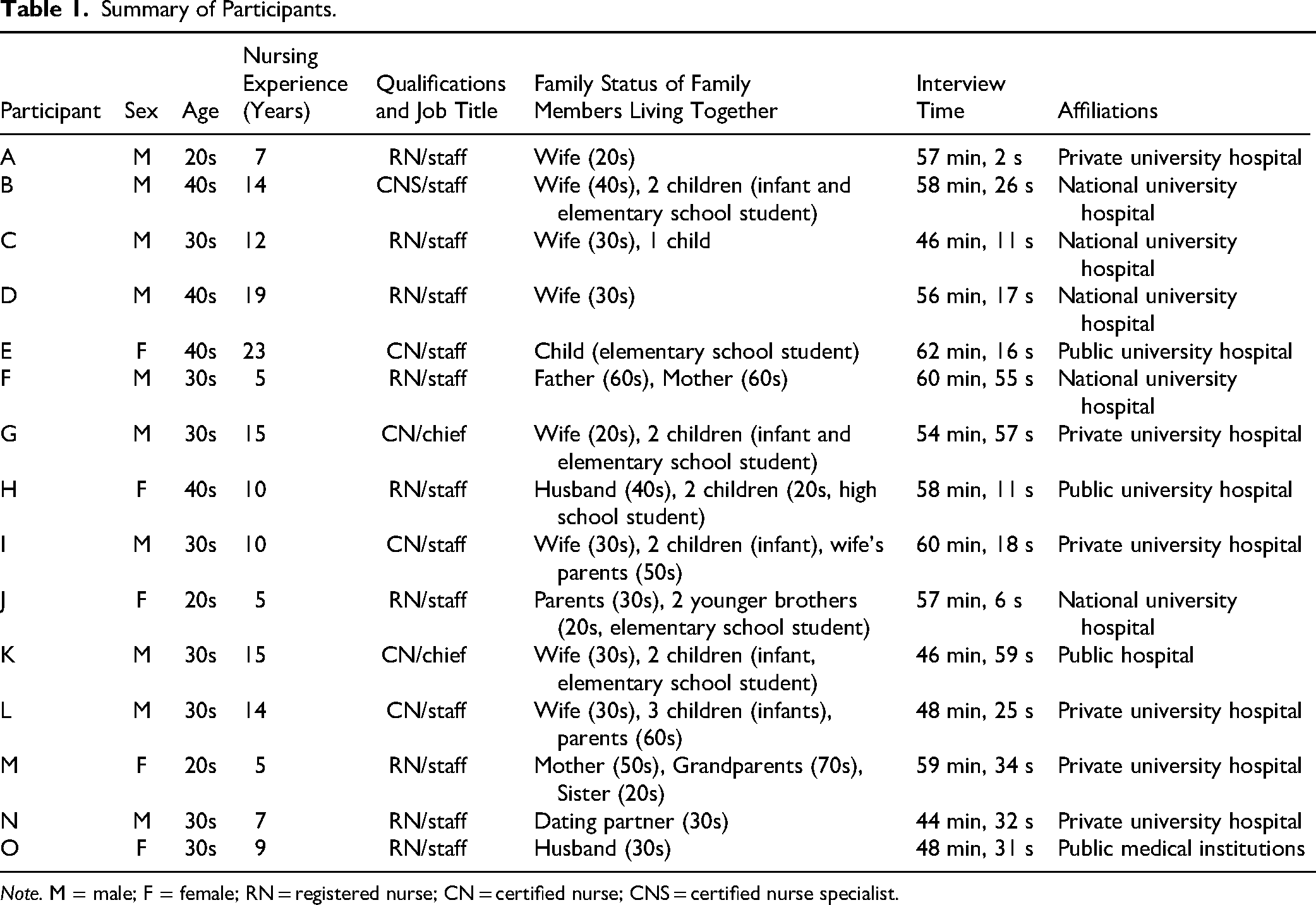
Note. M = male; F = female; RN = registered nurse; CN = certified nurse; CNS = certified nurse specialist.
There was a gender bias among participants. This was due to the small number of female nurses living with their families and working in the COVID-19 ICUs at the study sites.
Interviews lasted between 44 and 62 min, with an average of 54 min. Data collection continued until the characteristics of the theoretical categories were saturated.
Once the 12 interviews were analyzed, the major categories were considered sufficiently clear, and no new concepts appeared to be emerging (i.e., theoretical saturation had been reached). However, data from three additional individuals were collected to address gender bias and to ensure that the experiences of female nurses in different institutional settings were adequately represented. An assessment was conducted to determine whether the addition of these interviews would contribute any new concepts to the existing categories. Ultimately, data collection was terminated when no new major concepts emerged. This decision process was consistent with the principle of theoretical saturation in grounded theory, which holds that “no new meaningful findings will result from continued data collection” (Birks & Mills, 2015).
Data Analysis
In this study, data coding was performed by three researchers to ensure reliability. Data were coded row by row and then reviewed for code appropriateness by another researcher, a qualitative research expert. Following this process, focus coding was conducted. Common codes were merged across participants to form categories. MAXQDA 2022 software was used for analysis, and interviewer notes were also integrated. Through this multi-step coding and categorization process, a theoretical model was developed of the process by which nurses living with family members made the decision to work in the COVID-19 ICU. The research team discussed new ideas, concepts, and theoretical models throughout the analysis process in an effort to broaden the researchers’ perspectives. When disagreements arose, they were discussed, and categories were finalized based on consensus.
Ethical Considerations
The study was approved by the ethics review board of the researchers’ university. Nurses who agreed to participate in the study were informed that they could withdraw from the study at any time, interrupt the interview, or refuse to answer any questions they did not want to answer. Only audio recordings were obtained from the ZOOM interviews. Audio data were deleted after transcription. Confidentiality was maintained by removing all personally identifiable information from the interview transcripts. All research data were password protected.
Rigor
To ensure credibility, the interview and analysis processes were supervised by individuals with expertise in qualitative research methods. After generating focused and theoretical codes, the participants reviewed and confirmed the codes through member checks (i.e., interview transcripts and brief analyses were sent to participants for their confirmation). Furthermore, a non-participating individual with experience working in a COVID-19 ICU and who had cohabitating family members was consulted to verify the consistency of the analysis.
Results
Categories and Storylines
The analysis yielded 41 subcategories, 13 categories, and four core categories. Figure 1 illustrates the relationships among these categories.
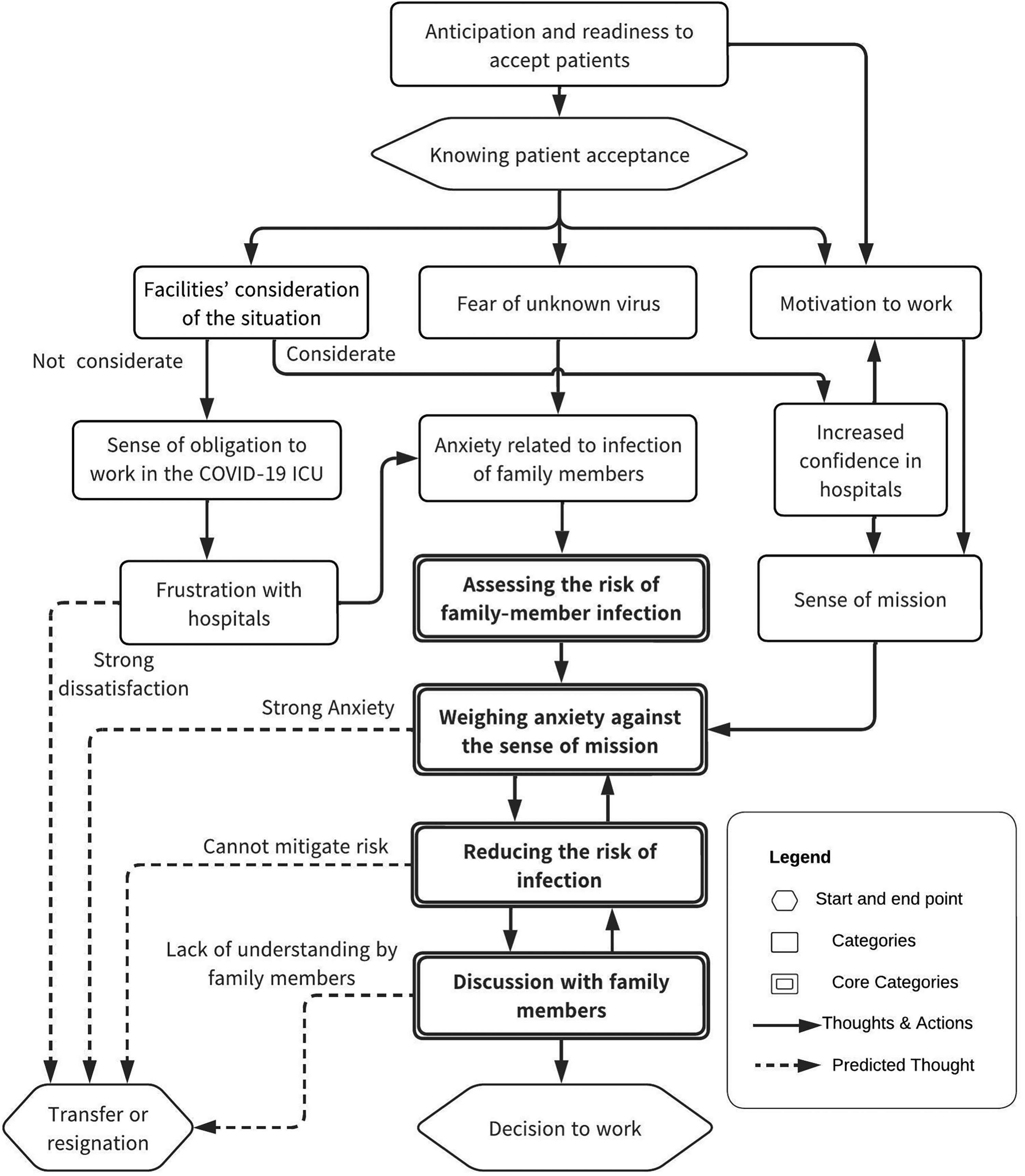
Process of a Nurse who Lives with Family Members Deciding to Work in a COVID-19 ICU.
The following recounts the “process of a nurse who lives with family members deciding to work in a COVID-19 ICU” as reported by participants in this study. (The endings have been changed to fit the context.)
Nurses who lived with their families and worked in an ICU learned of the spread of SARS-CoV-2 from news reports and were prepared to accept affected patients. When they were informed of the hospital's policy to accept patients with COVID-19, their trust in the hospital increased if the facility gave sufficient consideration to the situation (e.g., confirmation of willingness to work). On the other hand, a hospital's insufficient consideration of the situation led to dissatisfaction with the hospital and affected the nurse's subsequent continuation of work.
Many nurses expressed fear of the unknown virus and of infecting themselves or their families. When considering whether they could continue to work, they assessed the risk of family-member infection, including whether there were infants in the home or elderly family members with underlying medical conditions who were considered to be at high risk of serious illness at the time. In addition, any dissatisfaction with the hospital led to distrust regarding whether the hospital would take adequate infection control measures and truly protect employees and their families from infection, thus augmenting their anxiety.
However, most nurses expressed a sense of mission tied to their professional identities. This sense of mission was influenced by their trust in the hospital, as well as their desire to serve society in the fight against infectious diseases. The nurses weighed their sense of mission against their anxiety before consulting their family members about the decision. If the sense of mission outweighed the anxiety, the nurse developed strategies to reduce the risk of infection (i.e., living away from the family or implementing infection control measures at home). In the final discussion with family members, the nurse attempted to gain the understanding of any individuals who disagreed with the decision. These three themes (the sense of mission, infection control measures, attempt to gain understanding) had an impact on each other and were re-examined in subsequent discussions with family members.
The four core categories (“assess the risk of infection in the family,” “weighing anxiety against the sense of mission,” “reducing the risk of infection,” and “discuss the decision with family members”) interacted with each other and influenced whether the nurse decided to work. The ability to gain the understanding of cohabitating family members was critical to this decision.
Categories Within the Decision-Making Process
The 13 categories revealed by our analysis are described herein. Quoted narratives are italicized.
Anticipation and Readiness to Accept Patients
In Japan, the first outbreak of SARS-CoV-2 was reported in January 2020, and the pandemic spread rapidly. A state of emergency was declared in April (Ishii et al., 2022). Participants foresaw the possibility of receiving patients with severe COVID-19 at the facility where they worked after learning of the global situation via news reports and other media, and they were prepared to deal with the situation. I had already heard on TV that there were several severely ill patients in the province. Therefore, I knew there was no way they would not come to the hospital where I work. I think I was prepared. (Mr. G)
Facilities’ Consideration of the Situation
While some facilities surveyed and considered the preferences of employees before accepting patients with COVID-19, others decided to accept patients at short notice and did not consider the wishes of the staff members. At one participant's facility, the policy was communicated to the staff on the day of acceptance. No special consideration was given to whether the staff members were living with vulnerable family members (i.e., pregnancy, chronic illness). When I asked the manager how I would be compensated if I had a family-member and was infected, he told me it was a work-related injury and that I had no choice. I was forced to go back to work. (Ms. E)
Increased Confidence in Hospitals
The nurses reported having more trust in the hospital if their wishes were given sufficient consideration by the facility. At one facility, the hospital directors explained the situation directly to the staff members before they started accepting patients, and their willingness to work was also surveyed. One participant reported that these responses made him feel that the hospital was listening to and protecting him and gave him a sense of trust in the hospital. The hospital director, the university president, and other very important people came to see us. They talked to us openly. I think those things gave me a sense of trust in the hospital. (Mr. D)
Sense of Obligation to Work in the COVID-19 ICU
A lack of consideration for nurses’ desires led to the perception that they had no choice but to work in the COVID-19 ICU.
Although some staff members did not want to work because they lived with their families, several participants reported an atmosphere in which it was difficult to refuse. Some also described an atmosphere in which male nurses took it for granted that they would work, even if they had families. I’m in the ER, and I work in the critical care unit, so it was natural for me to work. There was still a lot of peer pressure. I think there were probably people who didn’t want to work in the COVID-19 Intensive Care Unit. (Mr. B)
Frustration With Hospitals
Nurses reported dissatisfaction with the hospital when employees’ wishes were not considered. Some participants considered transferring or leaving their jobs due to this dissatisfaction and distrust; one participant reported feeling resentful of the organization's system, which did not listen to the voices of the frontline caregivers. I received an e-mail out of the blue, without any explanation, telling me that I would start receiving patients the next day. I was very angry that they didn’t pay any attention to us. (Ms. M)
Fear of the Unknown Virus
All participants had been caring for patients since the beginning of the outbreak, and at the time, infection control and treatment methods were not fully understood. Therefore, the participants reported fearing the presence of the unknown virus. One participant said that she felt a fear of death, something she had never felt before in all the years she had worked at the hospital. When I was told that I was going to see a patient with an infectious disease for which I didn't know how it was transmitted or how to treat it, I was upset and thought I might die. (Mr. H)
Anxiety Related to Infection of Family Members
All participants reported they were concerned that, by caring for a critically ill patient with COVID-19, they would become infected and transmit the infection to the family members living with them. Some participants reported concern regarding the impact of the virus on their surroundings such as at work, in the community, or at school. I work and then go straight home. At that time, I still felt anxious about infecting my family. (Mr. B)
Assessing the Risk of Family-Member Infection
Because of their concerns regarding infection, participants assessed the risk of infecting their family members if they continued to work in the ICU; they wondered if the work was worth the risk.
Nurses who lived with infants or elderly family members were particularly concerned, as those family members were at high risk of serious illness.
Some participants said they might have refused to work if their wives were pregnant.
One participant's mother, who lived with her, developed cancer after the participant started working in the ICU; this development added to the fear that she might infect her. She said she would have hesitated if the risk of serious illness in her family had been present at the time she decided to work. If my parents had been weaker or older, I think I would have been more concerned. (Ms. J)
Motivation to Work
Many participants spoke of their motivation to care for critically ill patients with COVID-19. This motivation involved a personal mission to serve society in the fight against infectious diseases, an interest in fighting an unknown virus, and a desire to be on the frontline together as part of a medical team. One participant said she was elated to fight on the frontlines of the pandemic and was happy for the opportunity to treat patients with severe COVID-19 at her facility. In the midst of a global crisis, I was delighted to be on the front lines. (Ms. M)
Sense of Mission
Many nurses who decided to work cited their sense of mission as the reason behind their decision. Some participants attributed their sense of mission to their ability to work with severely ill patients with COVID-19, such as those on ECMO. Others attributed it to their qualifications as certified nurses or specialists.
One participant said he was already prepared to deal with infectious diseases and felt that, as an ICU nurse, it was natural for him to care for patients with COVID-19. I figured that, since I was a nurse, and an emergency nurse at that, it was only natural that I would deal with the infectious disease patients. “If we don’t do it, who will?” I thought. This pandemic was like a disaster. We thought it was our mission as emergency nurses to be on the front lines if something happened. (Mr. D)
Weighing Anxiety Against the Sense of Mission
Participants weighed their sense of duty as a nurse against the fear of infecting their families. When I weighed my sense of duty against my fears, my sense of duty won out. (Mr. F)
Reducing the Risk of Infection
Many participants considered strategies to reduce the risk of infection among the family members living in their home. Some participants mentioned living separately from their families, eating meals separately, maintaining a distance within the home to reduce contact, and taking infection control measures to increase family protection, such as showering before going home.
Examining the risk of infection when personal protective equipment was worn and adequate infection control measures were in place at the hospital helped reduce concerns about infection. When I came home, I made sure to take off all my clothes at the door. I took off my clothes, dipped all my clothes in detergent at the door, and went straight to the bath. We all discussed and implemented this lifestyle of washing ourselves in the bath and then going inside the house. (Mr. I)
Discussion With Family Members
After establishing their intentions, many participants met with family members to gain their understanding before making the final decision to work. In most cases, family members understood the nurse's reasoning and agreed to work together to reduce the risk of infection. One participant said that he would not have worked if his family members had objected and that he tried to convince them of the significance of caring for severely ill patients with COVID-19 when they objected due to infection concerns. The family was against it at first, but I convinced them that this was a place where they could show their value, and they finally agreed. (Mr. A)
Discussion
This study presents a unique focus by exclusively examining the decision-making processes of nurses who resided with their families during the COVID-19 pandemic.
The researchers investigated the factors influencing nurses’ decisions to work and identified the types of support that policymakers, hospitals, and administrators should provide in the event of a future pandemic.
Factors That Influenced Nurses’ Decisions to Work
Trust in the hospital and a sense of duty were key factors in the decision to work despite concerns about infecting cohabitating family members. A survey was conducted among nurses at multiple healthcare facilities, revealing varying levels of hospital support for nursing staff. Prior explanations and consideration of employees’ work preferences may have increased nurses’ trust in the hospital and commitment to the organization, thereby positively affecting their decision to work.
Monetary incentives were not offered at the time of the decision to work and, as found in a previous study (Ke et al., 2021), participants were motivated by a sense of mission rather than external recognition or rewards. A sense of mission is believed to arise from a sense of responsibility rooted in professional identity (Liu et al., 2020) and professional self-actualization (Sheng et al., 2020), both of which could increase professional commitment.
Some participants were offered financial incentives later, as the pandemic spread. There was testimony that some nurses wanted to work because of the incentives offered; for those who did not want to work initially, the availability of incentives may have influenced their decision to work.
Some participants expressed a desire to serve on the front line as members of a medical team. While the feeling of solidarity bolstered the decision to work and the willingness to do so, certain participants also reported experiencing peer pressure to work during the emergency. For instance, while previous studies conducted in China (Ke et al., 2021) and Saudi Arabia (AlOmar et al., 2021) reported patriotism and faith as determinants of work motivation, these factors were not observed in the present study. This discrepancy may be attributed to Japan's distinct cultural context, in which group peer pressure is known to exert a significant influence on behavior.
Moreover, during the recruitment stage of this study, there was a low representation of female participants with infants and a higher proportion of male participants. This deviates from the usual male/female ratio of nurses. During the pandemic, female nurses demonstrated a greater tendency than their male counterparts to avoid work and express an intention to leave the medical profession (Woo et al., 2022). This might be attributed to the fact that mothers, who are usually responsible for childcare, faced challenges in living apart from their young children, had difficulty implementing appropriate infection control measures at home, and were more concerned about transmitting the virus to their families (Mele et al., 2021). Furthermore, the pandemic-induced closure of schools and daycare centers resulted in increased childcare responsibilities for mothers of young children (Apple et al., 2023).
Some participants noted that male nurses were expected to work despite having families. Stereotypical gender roles (Collins et al., 2021) regarding work and childcare may have influenced nurses’ decisions to work.
In Japan, in particular, the traditional norms of role division (men as breadwinners and women as caregivers) are said to persist in society due to the lack of strong government support for balancing work and family life despite the changing socioeconomic conditions surrounding men and women (Kato, 2018). It is possible that Japan's cultural background regarding gender role consciousness and social expectations may have influenced nurses’ decisions to work.
One surprising finding of this study was that several participants privately evaluated job availability before conferring with their families. Family meetings were not held to discuss the employment decision itself, but rather to gain insight into relatives’ understanding of the decision. However, it should not be overlooked that family support played a significant role in nurses’ decisions to work; several participants noted that they would not have pursued a career in nursing if their families had objected. Additionally, all participants who chose to work acknowledged their desires and received support and understanding from their families. This suggests that, for nurses who reside with their families, familial support is the primary factor influencing their decisions to work.
Assistance Provided by the Hospital or Administrator
The nurses in this study were divided in their assessment of the hospital's response. While some participants developed trust in light of the hospital's consideration, many nurses were dissatisfied with the communication at the start of patient intake. Others strongly objected to the hospital's one-sided attitude of encouraging work without taking into account the individual staff members’ situations and the voices of the field. These frustrations and lack of trust raised concerns about whether adequate infection control measures were in place to protect healthcare workers and their families, as well as the hospital's ability to respond appropriately in the event of an infection outbreak. The COVID-19 pandemic in early 2020 forced hospitals to make rapid top-down decisions in response to societal demands (Ahlsson, 2020). However, the importance of listening to frontline nurses and demonstrating organizational commitment to their protecting became apparent. Such efforts can lead to increased motivation among nurses and their willingness to work. Therefore, fostering a workplace culture that values employees during normal times will contribute to effective decision-making in emergency situations.
Some nurses decided to use showers in the hospital and temporarily relocate to reduce the risk of infection to their families. Similar cases were reported in the international literature (Nashwan et al., 2021), but support systems and facilities varied among hospitals. The availability of nurses is essential for maintaining healthcare delivery, which highlights the importance of improving infection control measures. Furthermore, promoting work–life balance and improving the work environment, not only during a pandemic, are effective strategies for recruiting and retaining staff during an emergency. The results of this study are consistent with those of previous studies (Schaufeli & Bakker, 2004; Shimazu et al., 2015) showing that nurses with higher work engagement had lower turnover intentions. This supports the thought that work engagement is key to preventing turnover. Our results are also consistent with those of studies showing that improving the work environment and promoting work–life balance increases work engagement and reduces turnover (Bakker & Demerouti, 2007; Karanika-Murray et al., 2015). Therefore, healthcare organizations should strengthen organizational efforts to increase nurses’ work engagement, thereby securing sustainable human resources.
It is also important for hospitals to address Japan's unique cultural background, such as gender-based role awareness and social expectations, to respect the wishes and secure human resources for nurses of both genders. Administrators, hospitals, and managers are expected to promote measures such as the enhancement of childcare facilities in the workplace, the introduction of flexible work schedules, the promotion of male participation in childcare, the strengthening of mental health support, and the raising of awareness of gender equality.
Strengths and Limitations
This study included a diverse group of participants with regard to family structure, years of work experience, and roles. Additionally, it involved nurses working in seven different settings across the country, offering insights into the lives of nurses working in various settings and organizations.
However, the study inquired about experiences that occurred over 2 years before the interview, which raises the possibility that participants’ memories may have faded or their views evolved. As this study only surveyed nurses who were employed, the decision-making process may have differed from that of nurses who were not employed, and their experiences were not accounted for.
There was a gender bias in the study population, with a large number of male participants. Therefore, the study results primarily reflect the perspectives of male nurses, and the experiences and decision-making processes of female nurses may not have been fully explored. Future research could potentially gain new insights by increasing the number of female nurse participants, leading to a more comprehensive understanding of their perspective. The results of this study suggest that Japan-specific cultural backgrounds, such as gender role awareness and social expectations, may have influenced the decisions of nurses to work in the COVID-19 ICU. Therefore, studies on nurses in countries with different cultural backgrounds may result in different outcomes and reveal different decision-making processes.
Implications for Practice
Future research should include nurses who chose not to work to distinguish differences in the decision-making process between the two groups and investigate the additional support necessary for employee retention.
Conclusions
This study revealed the process by which nurses who lived with their families made the decision to work in the COVID-19 ICU. A sense of mission and trust in the hospital were important factors in overcoming concerns about infecting family members. It was also shown that the hospital's attitude toward the of care nurses contributed to the nurses’ willingness to work and reduced their anxiety. To secure a sustainable workforce, it is essential to strengthen organizational efforts to increase nurses’ work engagement from normal times. The findings of this study provide useful suggestions for considering appropriate nurse staffing and support measures during future pandemics. Furthermore, the study indicates that the promotion of gender equality may contribute to the recruitment of nurses. Traditional gender role perceptions in Japan influence nurses’ decision making, and different results may be obtained in countries with different cultural backgrounds. Future studies should consider measures that take cultural factors into account.
Supplemental Material
sj-docx-1-son-10.1177_23779608251345709 - Supplemental material for Determining How Nurses Living With Their Families Decide to Work in a COVID-19 Intensive Care Unit: Grounded Theory Study
Supplemental material, sj-docx-1-son-10.1177_23779608251345709 for Determining How Nurses Living With Their Families Decide to Work in a COVID-19 Intensive Care Unit: Grounded Theory Study by Akira Sato, Yoshiko Sasaki and Yoko Imazu in SAGE Open Nursing
Footnotes
Author Note
Tokyo Medical and Dental University was officially renamed Institute of Science Tokyo in October 2024.
Acknowledgements
The authors would like to thank the participants in this study.
Ethical Considerations
This study was approved by Tokyo Medical and Dental University's Institutional Review Board (Study ID # M2022-170) on December 4, 2022.
Consent to Participate
All participants provided their written consent to participate in the study, which was obtained prior to the interviews.
Consent for Publication
All participants provided written consent regarding the publication of the research findings.
Author Contributions
Akira Sato: conceptualization, methodology, investigation, formal analysis, and writing—original draft preparation. Yoshiko Sasaki and Yoko Imazu: supervision, and writing—review and editing. All the authors have agreed to the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.