
Abstract
The human toll which has resulted from the coronavirus disease 2019 pandemic is clearly recognised. No single event in recent times has had such profound effects on health services and their staff wellbeing around the world. Policy making has been led by the requirement for confinement and surveillance to limit spread of the disease, and in clinical settings the impact of the necessity for the use of personal protective measures has caused huge strains on practice clinically and professionally. In this paper we share experiences from the pandemic, explore the social and organisational factors at stake and make some suggestions for both personal wellbeing practice and a systems response to the ongoing staff wellbeing challenges of the pandemic.
Introduction/background
Coronavirus disease 2019 (COVID-19) has created unprecedented demands on healthcare workers and services around the world. Staff have experienced profound psychological distress, and burnout rates have increased. The 2021 National General Medical Council Survey found that around one-third of medical trainees felt burnt-out because of work, compared to a quarter in the previous survey. 1 A survey conducted by the Royal College of Nursing 2 years into the pandemic, and submitted to Scottish Government, details that more than 6 in 10 nursing staff in Scotland are considering or planning to leave their jobs, that 72% are under too much pressure at work and that 67% are too busy to provide the level of care they would like. 2 In further data, 50% of Intensive Care Unit nurse respondents met threshold criteria for severe anxiety, severe depression, harmful use of alcohol or probable post-traumatic stress disorder (PTSD); just under 15% had experienced thoughts of self-harm or suicidal ideation in the last 2 weeks. 3
To those who have worked in healthcare over the past 2.5 years, these findings are unlikely to be surprising. Many of the issues are not new, but have been massively amplified as a result of the pandemic.4,5 In this paper we share personal experiences, signpost approaches to self-care for individuals and consider the wellbeing implications of the pandemic from an organisational and structural perspective.
A clinician’s perspective: Dr Rowena Clark
I am a National Health Service (NHS) consultant in anaesthetics and critical care. In March 2020, at 32 weeks pregnant and having been heavily involved in the practical and strategic planning for a potential influx of patients requiring critical care, I was asked to stop all clinical work and stay at home. While my colleagues faced the most unpredictable and frightening clinical future of their careers, I found myself in the position where my most pragmatic input was in trying to improve morale, signpost for support and gather practical help for those ‘in the firing line’.
In those first few weeks, anticipatory fear and struggle with the lack of control were tangible. Clinical stress spilled over into family worry, concern about personal health and angst about the potential of onward viral transmission to others. Panic due to lack of Personal Protective Equipment (PPE), unanticipated guilt felt by those unable to work in their normal clinical roles and the difficulty of working outside a normal clinical role, were almost overpowering. Social media hype and information overload risked overwhelming staff. These psychosocial effects of the pandemic compounded the well-documented, everyday stresses of intense work in the NHS.
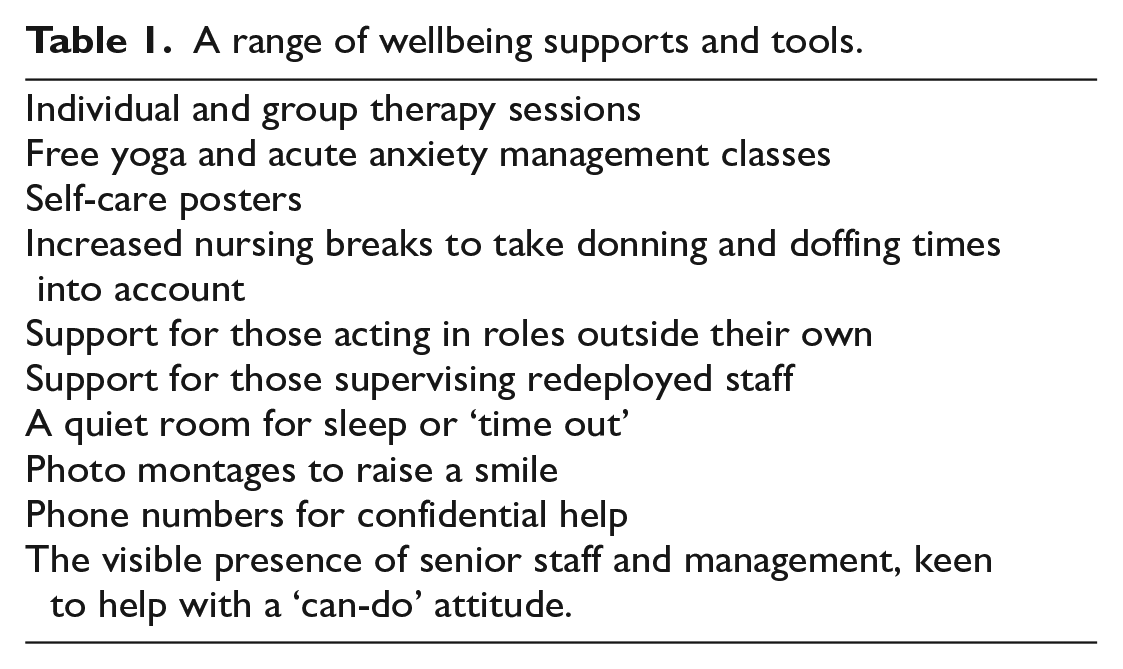
Alongside staff wellbeing resources at governmental and regional level, wellbeing management focussed on crisis coping strategies, gaining input from clinical psychology and sourcing comforts and safe spaces for staff. In keeping with many departments, mine has wellbeing groups, leads providing a range of support and tools, detailed in Table 1.
A range of wellbeing supports and tools.
The experience of trying to improve morale felt both fulfilling and woefully inadequate. It remains hard to tell how objectively helpful these ‘interventions’ were, given the lack of pre-pandemic comparison, dearth of qualitative research 6 and the non-homogenous approach taken across the country.
As time has progressed, the challenges facing those trying to improve staff welfare have shifted and changed. More accurately, perhaps, wellbeing priorities have drifted back to concerns surrounding long-term workplace aggravations. 7 Individual interventions have been curtailed as funding, and the will to persevere with time-consuming self-care processes, have dried up. Exhaustion, redeployment, chronic lack of staffing, basics such as lack of parking and the loss of initially overwhelming executive and public support now compound wellbeing fatigue; entrenched issues ‘at the coalface’ stubbornly persist.
How do we, as a heterogenous group of healthcare workers, practise self-care and fine-tune the art of wellbeing support, given the myriad challenges during and following a pandemic in the NHS? There are innumerable inspirational interventions and long-term mental health and wellbeing initiatives across the NHS, among them the new Workforce Specialist Service, a confidential mental health service for all regulated health and social care professionals in Scotland. 8 Data from short-term digital wellbeing interventions also look promising, with the possibility of context-specific and rapidly modifiable application. 9 In addition to these, organisational support to address long-term occupational issues, and persevere with awareness and training in psychological first aid and staff welfare, may improve overall engagement and morale.
I ache for the Art of Medicine’s most profound loss: I cannot touch my patients anymore. The void left by the loss of what defines us, is witness to unspeakable grief. Physician, male, South Africa, MSc in Critical Care, University of Edinburgh
An educationalist’s perspective: Dr Graham Nimmo
I retired from the full-time clinical practice of intensive care in the summer of 2019. In September 2019 we launched our MSc in Critical Care at the University of Edinburgh with David Griffith (Reader in Anaesthesia and Critical Care) and myself as joint directors. Our students are from countries around the world, representing multiple health care professions, all of whom were working in frontline acute care.
In March 2020, when we were less than two-thirds of the way through the academic year, the World Health Organisation declared the COVID-19 pandemic. We realised that our students and faculty would be involved in the clinical response to this and we approached the University to request that our programme be suspended. This happened almost immediately. Simultaneously, we wondered what the MSc Critical Care programme could do to help. With a rapidly assembled team, we curated and launched a Massive Open Online Course (MOOC) on Critical Care, in a record time of 10 days from start to finish. Over 53,000 learners have now enrolled on this course globally. 10
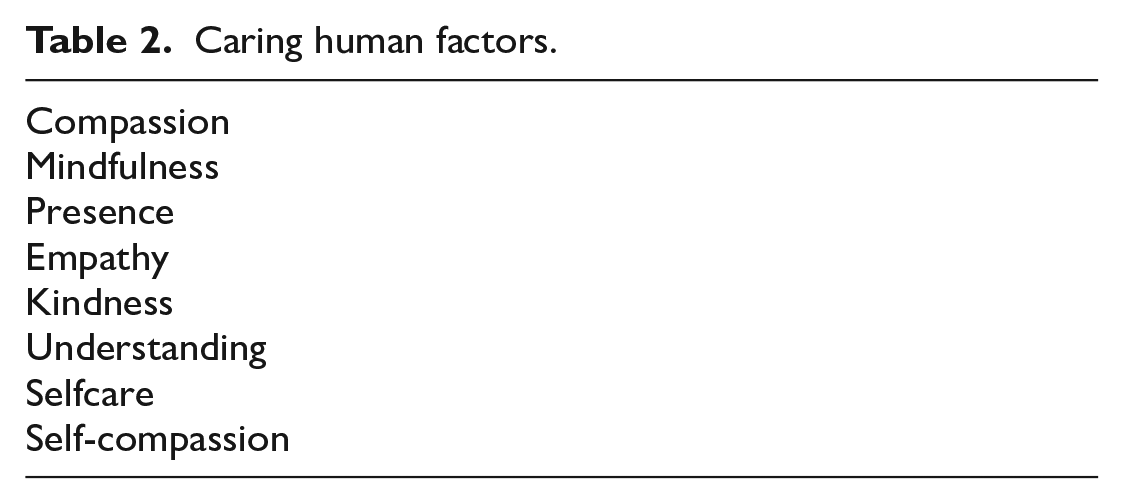
As an integral part of this we included a module on Self Care and Staff Wellbeing, whose popularity is evidenced by the large number of learner visits (Figure 1). The Self Care and Staff Wellbeing module distilled concepts and practices which we have developed and categorised as ‘Caring Human Factors’ (Table 2). Figure 2 illustrates how these relate to the domains of Human Factors Science and Clinical Human Factors. A key component of Caring Human Factors is looking after ourselves physically, mentally, emotionally and spiritually: if we care effectively for ourselves, we can then care for others better. As Neff writes, this is ‘putting on your own oxygen mask before you start to put on others’. 11 We now advocate for self-care training for all healthcare staff and students. In collaboration with nursing and mindfulness colleagues at the University of Edinburgh, and recognising the ongoing workplace context of cumulative trauma in which the pandemic occurred, we have created a free trauma-sensitive Self Care and Wellbeing MOOC for health and care professionals and students. 12 At the time of writing this has had 4,770 learners enrol from around the world.
I have heard fathers’ voice crack with emotion as I deliver devastating news, via the telephone. I have held up tablets as families say goodbye to loved ones, a stranger in the corner of the room. I have listened to relatives tell me all about their loved ones, without even being able to offer them a weak, plastic cup of NHS tea. Anaesthetist, female, UK, MSc in Critical Care, University of Edinburgh
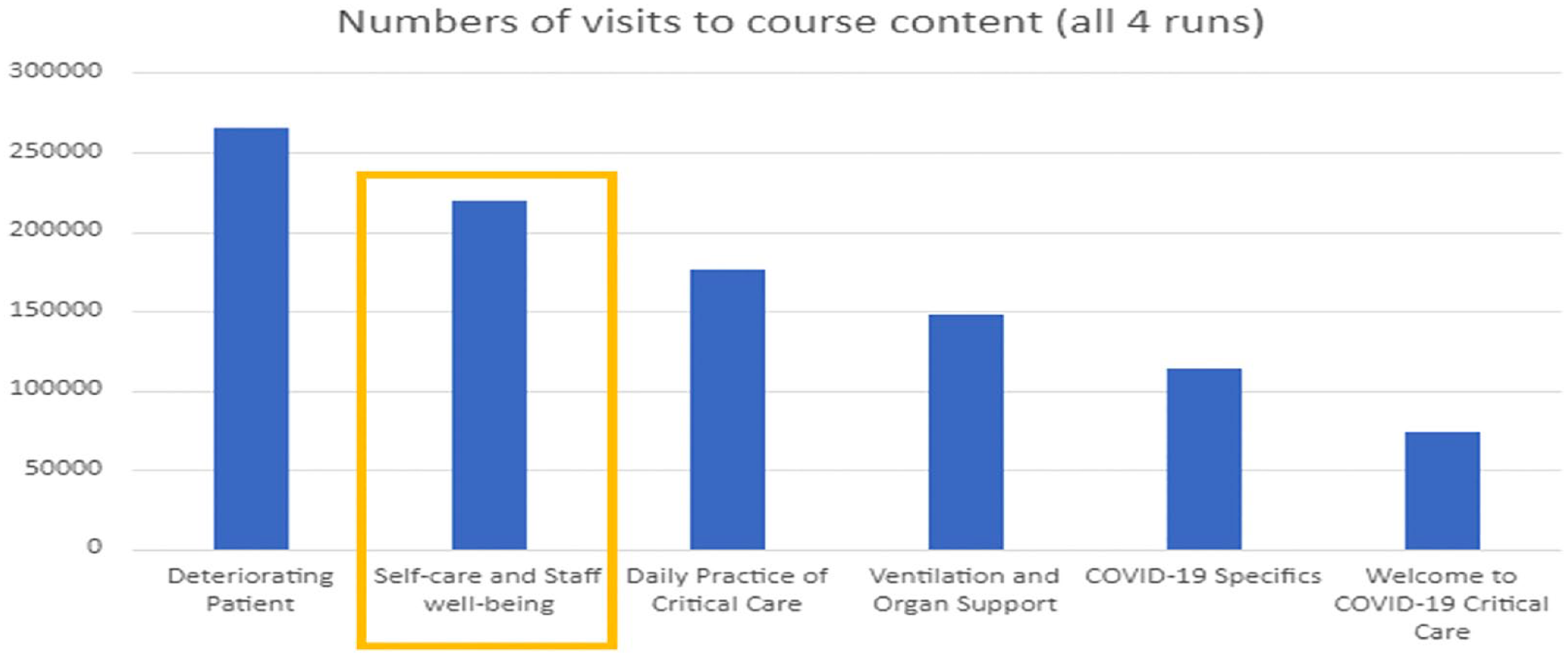
COVID-19 critical care MOOC runs 1–4.
Caring human factors.
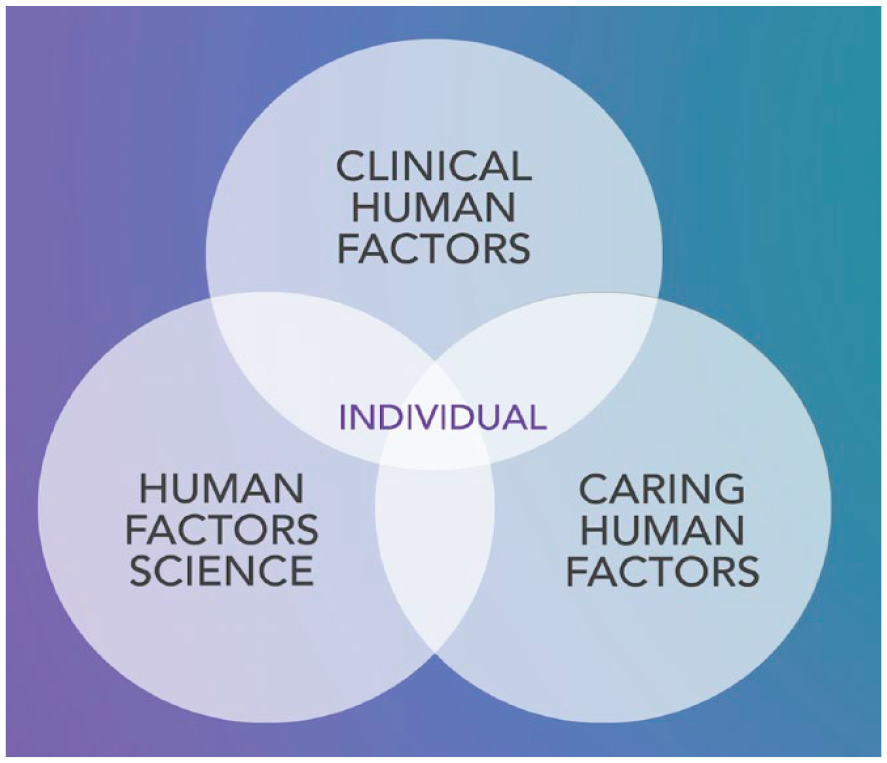
Human factors relationships.
A trauma-sensitive mindfulness perspective: Dr Kitty Wheater
Over the last few decades mindfulness has been hailed as a powerful method of self-care, yet concerns have also been raised about its co-option as a bandaid for systemic failures of responsibility and care. ‘Self-care’ as bandaid among healthcare workers could – during a global pandemic, for example – perpetuate those failures, and aggregate the suffering of those subject to them. A trauma-sensitive mindfulness (TSM) perspective on self-care and wellbeing during the COVID pandemic is therefore two-fold. As a Mindfulness-based Cognitive Therapy and TSM practitioner, and medical anthropologist, I argue both for the value of self-care measures when grounded in an understanding of nervous system dysregulation, and for clarity as to the systemically traumagenic environment of health care during COVID-19. Self-care without systemic care stores up trouble – because trauma calls in its debts.
My exploration of trauma-sensitive practice comes from the US National Centre for Trauma-Informed Care, via the work of David Treleaven, TSM practitioner and social worker (2020). 13 The 4 ‘R’s of trauma-sensitive practice are: realising the ubiquity of trauma; recognising symptoms; responding effectively; and preventing re-traumatisation.
Realising the ubiquity of trauma
Worldwide, 90% of us will experience a traumatic event at some point in our lives, ranging from physical and sexual violence to illness, accident and injury. ‘Ninety per cent of us’ is the context within which healthcare workers ordinarily experience cumulative trauma in the course of their work; that cumulative trauma is the context within which the pandemic, itself a societal and prolonged trauma, occurred.
The implications for healthcare staff are three-fold: the incurring of new trauma at work; the incurring of new personal trauma; and the amplification of historic trauma. The COVID pandemic has been the perfect mental health storm for healthcare workers. A major study of PTSD and major depression (MDD) among frontline healthcare workers found that ‘Forty-four percent met criteria for PTSD and 39% met criteria for MDD. Twenty-four percent reported COVID-19 trauma as their index event, with the majority of staff reporting trauma that pre-dated the pandemic. While PTSD was likely to be pre-existing, MDD was more likely to develop during pandemic working’. 14 This means that in addition to healthcare workers’ current toll of categorically poor mental health, individual and systemic conditions for future trauma may already be in place.
Recognising symptoms
Acute stress triggers hyper-arousal. The sympathetic nervous system engages, and we typically feel highly agitated, anxious and easily overwhelmed, with racing thoughts. This is commonly known as fight or flight. If there’s no escape from the stress, the parasympathetic nervous system slams on the brakes, and we go into ‘freeze’, or hypo-arousal. We may feel numb, stuck, cut off from our bodies, and unable to concentrate.
The ‘window of tolerance’, coined by psychologist Daniel Siegal, is the space in-between hyper- and hypo-arousal. In this space, we are well-regulated: that’s not to say that we don’t experience difficulty, but the nervous system is able to regulate stress as it arises, meaning that we’re not pushed into overwhelm. 15
Trauma and chronic stress both narrow the window of tolerance. This means that we oscillate between hyper- and hypo-arousal: anxious/agitated, depressed/numb, with small respite in-between. ‘Resilience’ is diminished: healthcare workers may find that things that didn’t used to provoke stress now feel unmanageable; they may over-react and under-react in equal measure. For the window of tolerance to expand once narrowed, it is not enough for the trauma to pass; the nervous system requires positive safety and containment. Both self-care and systemic care are required in that response.
Responding effectively
Wellbeing initiatives that foreground self-inquiry and investigation, rather than simple palliation, are important. Best-practice mindfulness programmes, such as Mindfulness-based Cognitive Therapy, teach individuals skills of psychological self-literacy and self-regulation. For an effective trauma-sensitive response however, wellbeing and self-care initiatives need to occur as part of a ‘mindful culture’ in healthcare that promotes inquiry and action as to the causes, manifestation, and easing of traumatic stress among its staff.
Rowena’s example of the promotion of wellbeing measures amidst absent PPE is particularly pertinent. Techniques to promote the nervous system’s sense of safety, amidst an unsafe environment, may help some to reduce stress and navigate those risks effectively; but the systems that have given rise to that lack of safety endure. At worst, wellbeing techniques become a misguided means to compensate for systemic failures. Healthcare workers are thus both exposed to physical harm at work, and incur potentially traumatic stress from that exposure. A trauma-sensitive response to healthcare workers’ wellbeing in the wake of the pandemic must therefore operationalise a systemic, rather than individual, definition of ‘wellbeing’.
Preventing re-traumatisation
As Wild et al. show, the toll of COVID on healthcare staff’s wellbeing is bigger than COVID itself. 14 The pandemic incurred new trauma and aggravated old; moreover, even with a return to something like ‘normal’ business in the NHS, the nature of that normal business for frontline staff is one of chronic stress. The collective ‘window of tolerance’ has narrowed, and the urgent systemic question must be how positive change can be effected. The risk is that when healthcare’s next crisis comes, the traumatic legacy of the last will exact an aggregated toll.
A patient of mine had been tested positive for the virus. It was fever, and aggravating shortness of breath, that had made her present herself to the health authorities. Until the time she was put on artificial respiration, she shared some painful messages about how she was being treated. It was evident that most members of the treating team showed fear, if they ever showed themselves. Physician, male, Mauritius, MSc in Critical Care, University of Edinburgh
A sociological perspective: Dr Catherine Montgomery
From a sociological perspective, self-care needs to be considered within the wider social and structural environments in which healthcare workers are positioned. Indeed, Rose et al. (2020) argue that individualised psychology-based interventions will be ineffective unless the social preconditions for wellbeing are in place, resonating with the systemic approach to wellbeing described above. 16 Rather than focusing on the actions that individuals can take to enhance their wellbeing, therefore, qualitative social research into the experiences of frontline staff during COVID-19 underscores the importance of actions that must be taken at the level of organisations, national policy and society as a whole.
Between August and October 2020, a multi-disciplinary team of colleagues and I conducted research into staff experiences of working in critical care during the first wave of the pandemic. 17 Our team combined sociological with clinical expertise: we consisted of a critical care consultant, clinical professor of nursing, professor of sociology, nurse researcher in critical care, research nurse and myself, a medical sociologist. Our aim was to generate theoretically informed, actionable insight into changes in working practice in critical care, including interaction with patients, technology for family communication, end of life and personal wellbeing and support.
Based on an analysis of interviews with 40 staff across 4 hospitals, we characterised frontline staff as a ‘community of fate’, whose experiences of extreme duress bound them together. Staff mobilised around a shared purpose and resources to take collective action in the face of existential threat. Solidarity and teamwork were essential to a functioning COVID-19 critical care system, not least because these factors supported staff in terms of their own wellbeing. We stressed the importance of structural resilience in critical care and the need to attend to the conditions under which teams can prosper. This includes adequate resourcing and provision of PPE, as well as systems to develop transparent plans for managing surge situations.
The structural nature of healthcare worker vulnerability and distress are dealt with by Smith (2020) and Sukhera (2021) respectively.18,19 Smith argues that to design interventions that are equitable, we must acknowledge the structural nature of differential vulnerability 17 : subgroups of the healthcare workforce – those who are marginalised, under-represented or have less collective power to advocate for safe working conditions – face differential risk. Other studies also highlight the gendered and racialised effects of the pandemic on the healthcare workforce.20,21
Providing more nuance, Sukhera et al. (2021) describe the intersection of moral distress with structural stigma, defined as ‘societal-level conditions, cultural norms, and institutional practices that constrain the opportunities, resources, and well-being for stigmatized populations’ (p. 223). 19 The authors found that Canadian resident physicians experienced ‘structural distress’, whereby their relative powerlessness led them to over-perform in their role, worsening their psychological wellbeing. They recommend that faculty and organisations enhance students’ agency by creating a culture of transparency and involvement in policy decisions; and that medical programmes draw explicit attention to structural distress, and critical perspectives on the ‘hero narrative’ as part of residency training.
The hero narrative has been a consistent focus of critique in sociological and anthropological studies of healthcare worker experiences during the pandemic.22,23 This refers to the way in which healthcare staff have been glorified as heroes – and sometimes angels – in the media and popular culture, exemplified in the UK by the ‘Clap for Carers’. Navuluri et al. (2021) describe how the trope of the ‘healthcare hero’ bleeds into resilience narratives, in which healthcare workers are both responsible for developing their own resilience strategies, and simultaneously presented as possessing superhuman capacities to withstand pandemic pressures. 22 Studies show that not only does heroism discourse fail to resonate with the people it describes, it also mischaracterises as a superpower the labour they perform, erasing unequal conditions of employment risk and diminishing the ability of individuals to express their need for support.22 –24
In light of these critiques, we may ask how support should be conceptualised and designed. Willis and Smallwood (2021) provide much-needed insight into this question, analysing free text responses to a survey of over 9,000 healthcare workers in Australia. 24 They focus on the ‘spillover’ of risk between work and home; within this context, interventions focussed on individual wellbeing, such as meditation, were seen as a poor substitute for organisational health and safety measures, such as adequate provision of PPE. Willis and Smallwood describe the latter as a ‘major signifier of perceived personal value to the organisation’ (p. 178), underscoring that such interventions must form the foundation for any subsequent approaches to self-care. By the same token, Billings et al. (2021) note that when institutional interventions were removed and resources taken away after the perceived need subsided (e.g. staff rooms for rest, provision of hot meals, etc.) staff felt demoralised and de-valued. 22 This underscores the need for long-term commitment to healthcare worker wellbeing rather than short-term ‘crisis’ responses alone.
I am growing weary of undressing in the garage. We are forced to adopt new practices to keep ourselves safe and these can be both strange and unsettling. Prior to the pandemic my usual post-work routine consisted of walking in the door and kicking off my boots. Paramedic, male, Canada, MSc in Critical Care, University of Edinburgh
Commentary
‘Both fulfilling and woefully inadequate’: Rowena Clark’s description of wellbeing work during the COVID pandemic perhaps best summarises the state of self-care and wellbeing initiatives among healthcare staff over the last 2 years. In this paper, we have brought together perspectives from clinical staff, a clinical educator, a TSM practitioner and a medical sociologist. While diverse, they all point to a similar conclusion.
Rowena describes how clinical staff put great effort into practical and community-spirited wellbeing measures during the pandemic. This notwithstanding, the structural problems and long-term occupational issues underpinning clinical work, which never went away, have predictably re-emerged as foci for discontent. She describes this in the context of fading funding and motivation for self-care measures; to this we would add, the fading of hope that they might make long-term difference in the face of systemic dysregulation.
Graham’s account shows the resourcefulness of healthcare staff in creating and disseminating high-quality self-care and wellbeing educational and practical materials during the pandemic, as well as the willingness of frontline staff to engage. This is suggested by high numbers of online learners on a COVID Critical Care MOOC. This indicates that poor wellbeing among the healthcare workforce is not reducible to disengagement with wellbeing practices.
Nuancing the emerging structural perspective, Kitty offers an explanation from a TSM lens of why poor wellbeing among healthcare staff endures. She suggests that the COVID pandemic occurred in a context of cumulative workplace trauma, and in a population in which post-traumatic stress is more widespread than commonly realised – a traumagenic ‘perfect storm’. She argues that self-care measures, while vital, are in themselves insufficient without systemic care, and suggests that without systemic action, come the next crisis, the conditions for future workforce trauma are already in place.
Through a sociological perspective, Catherine identifies mechanisms by which the structural problems occasioning poor staff wellbeing are obscured. She critiques the ‘resilience’ and ‘hero’ narratives about frontline healthcare workers, arguing that these obscure problems such as a lack of organisational health and safety. While poor wellbeing is often individualised in both proposed aetiology and solution, she notes that its structural causes mean we might better term it ‘structural distress’. This experience echoes the findings of other investigators including De Cock and colleagues. 25
These accounts paint a clear picture. We have seen the strong community spirit of healthcare workers, from those behind the clinical and educational scenes, to those on the ‘communities of fate’ frontline; the development of innovative self-care and wellbeing resources to meet COVID pandemic demand; and the willingness of healthcare staff to engage with these resources where available. New mental health and wellbeing resources for regulated healthcare professions are a welcome boost to the landscape of healthcare staff wellbeing provision. Nonetheless, the systemic economy of staff wellbeing retains room for improvement. The debacle over PPE is a recurring trope across the accounts presented here, as are staffing shortages and overwork. Seemingly small and casual efficiencies, such as the removal of comfort resources, also dehumanise staff. We conclude that while self-care and wellbeing initiatives are and will continue to be vital to healthcare staff, organisational failures and discrepancies during the pandemic have been highly productive of distress, in ways that the terms ‘mental health’ and ‘wellbeing’ may discredit, unless understood and addressed systemically.
Footnotes
Acknowledgements
We are grateful to the following University of Edinburgh MSc Critical Care students who gave permission for us to include excerpts from their written work: Kevin Lambert, Ashveen Puryag, Robert Smith, Claire Snelling, Lucy Stevenson.
We thank Professor Tonks Fawcett, Nursing Studies, University of Edinburgh for her helpful comments and review of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Belmont University, Payment to me for mindfulness workshop in private practice.
Shepherd and Wedderburn (Services) Limited, Payment to me for mindfulness workshop in private practice
Various, Payment to me for mindfulness teacher supervision in private practice.
Medical Research Scotland COVID-19 Research Grant [CVG-1739-2020], Awarded to PI for the project ‘Caring, Learning And Pandemic response during COVID-19: Staff Experience of Working in Critical Care’.
Regional Rep and Lead for Wellbeing on the Council of the Scottish Intensive Care Society, Unpaid position.
None.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.